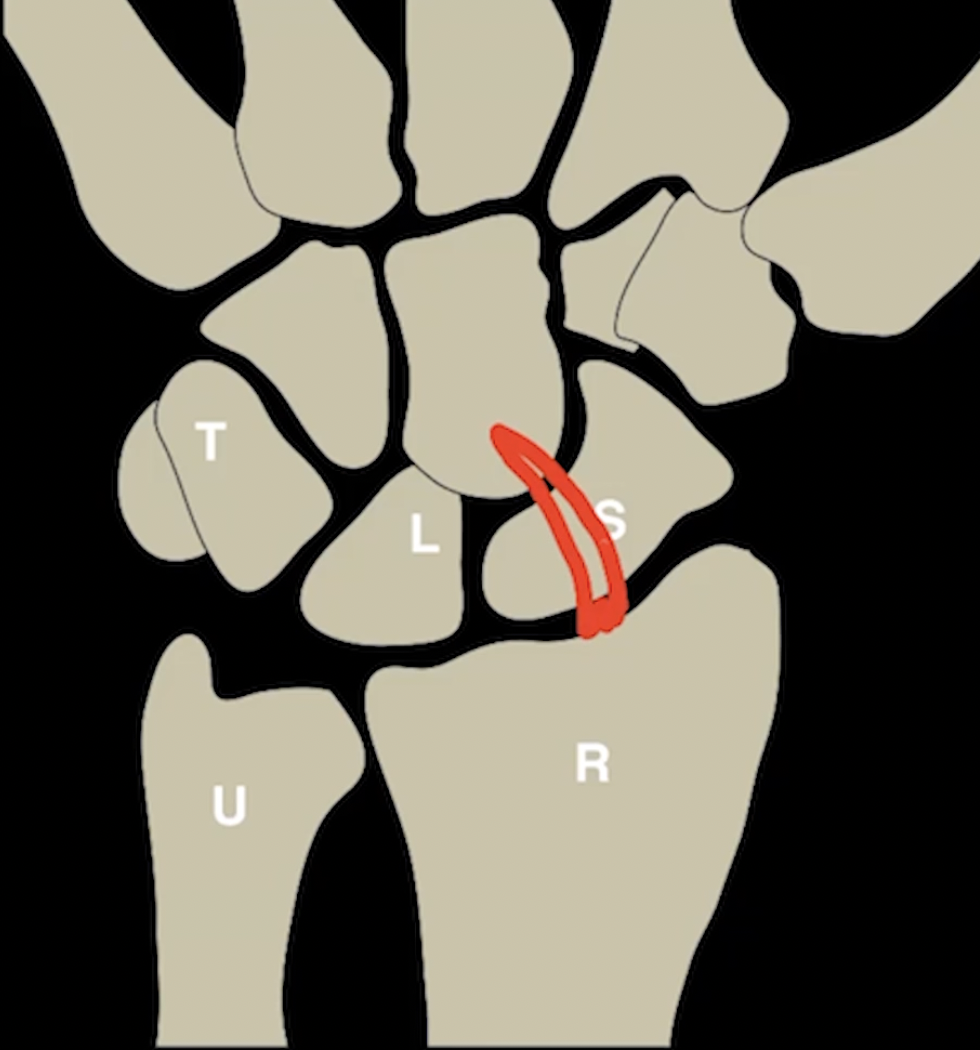
Wrist
Scapholunate ligament
Volar part (trapezoidal shaped)
Interosseous membranous component (triangular shaped)
Common to see signal in it and have asymptomatic tears
Dorsal part = strongest (striated-band shaped)
SLD & LTV
Scapholunate - dorsal is strongest
Lunate-triquetral - volar is strongest
Volar rhomboidal shaped

Ulnar Variance
Negative Ulnar Variance
Ulnar lower than radius at DRUJ
Associated with
Lunate osteonecrosis
Ulnar impingement
Interosseous Membranous (triangle shaped)

Scaphoid
Lots of pathology with this little bone
Gets retrograde blood flow (from distal hand to proximal)
Therefore the proximal aspect is last to get blood and therefore more likely to get AVN
Prieser disease = atraumatic AVN of scaphoid
Fractures
Most commonly fractured at the waist
Displacement >1 mm = likely surgical fixation
Associated with perilunate dislocation
Humpback deformity
Scaphoid waist fracture with angulation of fracture fragments
Progresses to collapse and non-union
Get abnormal healing that looks like a humpback
Associated with DISI
Fractrue
Scaphoid Stabilizers
Scapho-lunate ligament
Scapho-traezial-trapezoid ligament
Very thin lines between these bones that is very hard to see
SLING ligament (image below)
Radio-scapho-capitate ligament
Arises from mid radius to attach to capitate with debated attachment or overlying of scaphoid
References:
Dorsal (striated band shaped)

Scapholunate Advanced Collapse (SLAC wrist)
Most common cause of degenerative changes of the wrist from injury or degeneration typically from CPPD to the scapho-lunate ligament
Note: At baseline the scaphoid always wants to rotate in flexion but is restrained by the SL ligament, if the ligament is injured it will be allow to rotate
Scapholunate ligament
Volar part
Interosseous membranous component
Dorsal part = strongest
SLD & LTV
Scapholunate - dorsal is strongest
Lunate-triquetral - volar is strongest
If suspected injury on radiograph —> clenched fist view radiograph —> should make it worse
High risk of developing DISSI - dorsal intercalated segmental instability
Causes
Scaphoid fracture = bony DISSI
Distal radius fracture = compensatory DISSI
Radius malunion = adaptive DISSI
Dissociation of scaphoid and lunate = ligamentous DISSI
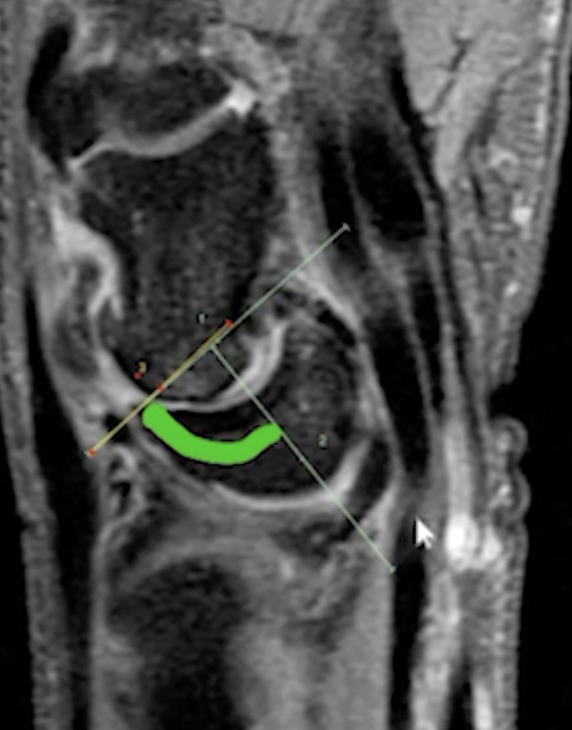
Results in a lunate basically angulated volarly
Look at angle below with green curved line
Should be less than 60 deg, if >70 deg almost always DISSI
Findings
Hypertrophy of the radial styloid (scaphoid rubs against it) - stage 1
Arthritis (joint space narrowing, degen of scaphoid) at scaphoradial joint - stage 2
Narrowing, erosions of capito-lunate articulation - stage 3
Generalized degeneration of the intercarpal and carpal-radial articulations - stage 4
DISI
Radial side injury
Injury to scapho-lunate ligament (i think)
Lunate rolls dorsally
Angle > 60
General
Multiple synovial spaces in wrist
The pisiform and radiocarpal joint synovial spaces communicate normall
If you see a wrist effusion would expect to see increased fluid around pisiform too
Can also use the pisiform space for wrist arthrography
Carpal Dislocations
Peri-lunate dislocation
Lunate and radius stay together but the otehr carpal bones move
High association with scaphoid fractures
Most benign of the dislocations
De Quervian Tenosynovitis
Entrapment of the first extensor tendon compartment containing
First extensor tendon
Abductor pollicis longus tendon
Extensor pollicis brevis tendon
Entrapment is typically at the radial styloid by extensor retinaculum
Positive finklestein test
F>M (pick up babies, typing etc.)
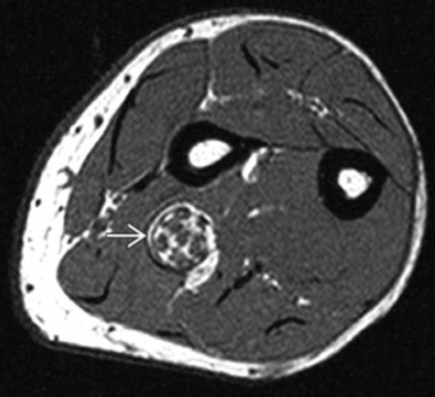
Lipomatosis of Nerve
Basically fatty infiltration of the nerve
If occurs in median nerve will result in thenar atrophy similar to carpal tunnel syndrome
Has the coaxial cable appearance
If you see fat in the lesion it excludes a neurofibroma or schwannoma which are other items in the ddx
VISI
Ulnar side injury
Injury to luno-triquetral ligament
Lunate and scaphoid move volar
Scaphoid-lunate angle <30
Rare
Intersection Syndrome
Tendinitis of the 1st & 2nd extensor tendon compartments where they cross over each other which is ~4cm proximal to listers tubercle
Occurs more proximally that DQT
First extensor tendon compartment contains
First extensor tendon
Abductor pollicis longus tendon
Extensor pollicis brevis tendon
Second extensor tendon compartment contains
Second extensor tendon
Extensor carpi radialis longus tendon
Extensor carpi radialis brevis tendon
Ulnar nerve hypertrophy
Seen in bicycle riders
Nerve should normally taper as it moves toward wrist
In this it will gradually get larger
Lunate dislocation
Lunate dislocated and other bones normal
Associated with dorsal radiolunate ligament injury
Most severe of the dislocations
Wartenberg Syndrome
Compression of superficial branch of radial nerve in distal forearm
Tight watches can cause
Pain at rest
Positive tinel test
Positive Ulnar Variance
Ulnar higher than radius at DRUJ
Can get lunate-ulnar impaction syndrome where the distal ulna abuts the lunate and you get degenerative shit/cyst formation, etc.
Mid-Carpal dislocation
Capitate and lunate lose alignment with radius
Associated with
Triquetral fractures
Triquetral0lunate interosseous ligament disruption