Nuclear Medicine
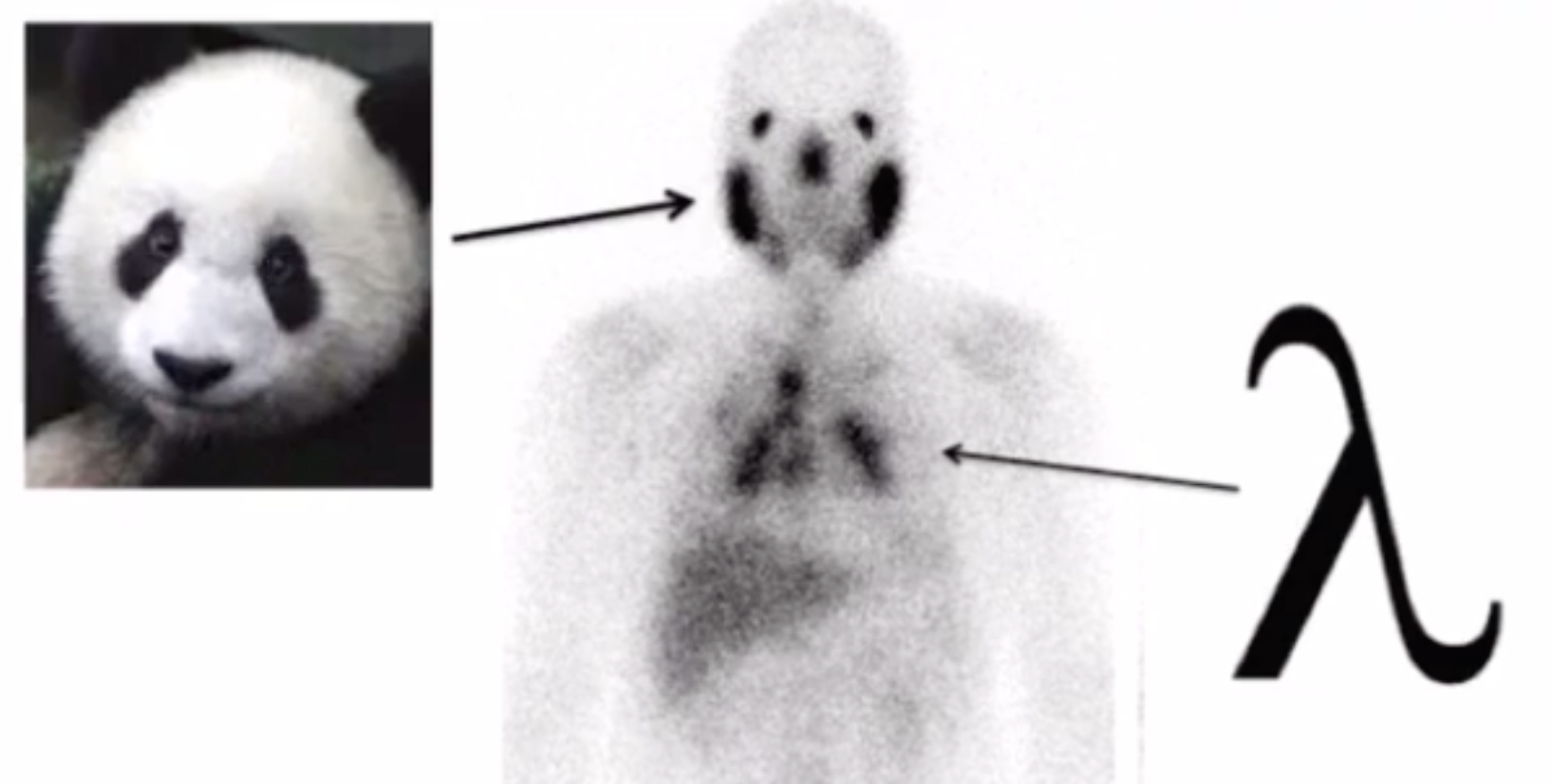
Sarcoidosis
Lambda sign
Hilar lymphadenopathy looks like greek letter lambda
Panda sign
Seen on Gallium-67-citrate studies
Uptake in parotid and lacrimal glands (abnormal) and nasopharyngeal tissue (normal) makes it look like face of a panda
Lymphoma and Sjogran also in differential
PSMA
Will see salivary glands are dark if PSMA is used
General
Appendicular skeleton = extremities, pelvis
Axial skeleton = skull, spine, thoracic girdle
Bome is essentially made up of calcium, phosphate and hydroxyl ions so the agents used will be related to these in some way
Most commonly used agent = methylene diphosphate labeled with Tc (Tc-MDP)
Complications
Administer 4+ hours after tracer is prepped —> gastric and thyroid visualization as a result of free Tc
Air injected during prep —>Tc becomes oxidized and poor phosphate tagging, idk shitty images i guess
Bone Scan
Tracer = Methylene Diphosphate (MDP), typically tagged with Tc
T1/2 = 6 hours
Energy = 140 keV
MDP only shows you osteoblastic activity, (if not remodeling then won’t be MDP pos)
Will be used in the osteoblastic phase where it basically gets included in the rebuilding process
Chemisorption = MOA
Basically chemical reaction between surface and the absorbed tissue, something like this
MDP has to be tagged with Tc to be able to actually see anything
In order to do this you mix the MDP + free Tc + stannous ions
If have contamination of this process with water or air (pull back on syringe) or not enough stannous ions (tin) you will have more free Tc than can bind and you will have uptake in the study in the salivary glands
Water contamination = liver will look hot = because you will form Tc-dioxide and Sn-colloid (tin colloid)
Air contamination = free Tc = hot salivary glands, gastric tissue, thyroid
Not enough stannous ions = same as air contamination = free Tc
Typically has 3 phases when done
Phase 1 = Flow phase
Images obtained every 5 sec for 1 min after administration
Shows the perfusion (blood flow) to the area
Phase 2 = Blood pool phase = soft tissue phase
5 min after administration
Basically how much fluid is in tissue, based on principle that inflammation causes capillary permeability and leak
Phase 3 = Delayed phase
Obtained 2-4 hours after administration
Uptake depends primarily on rate of new bone formation/remodeling
Fractures
After a fracture an osteoclast will come first and resorb the bone
Then you will get osteoblasts who put down new bone
There is increased vascularity in this process
Process requires
Vit D
Osteoblasts
Blood flow
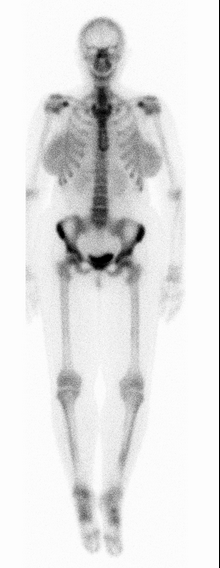
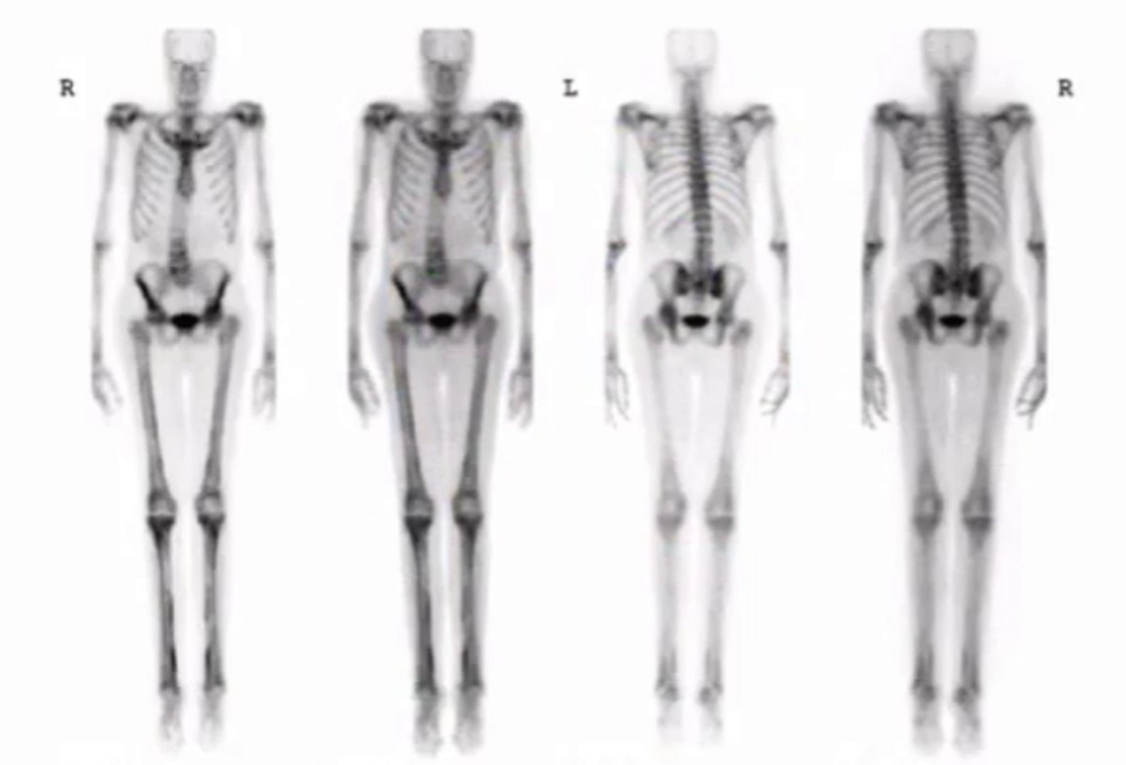
Normal bone scan
Increased uptake where there is trabecular (cortical) bone
Spine for example
Can faintly see kidneys
Some uptake in bladder
Mild symmetric uptake in breast
Low level in soft tissues
Epiphysis in kids
Osteomyelitis
Difficult to evaluate on bone scan because of overall poor perfusion to feet and small vessels
Use a 4th phase protocol
Gets you additional images at 24 hours —> gives you the most bone uptake after most has left the soft tissues so easier to see
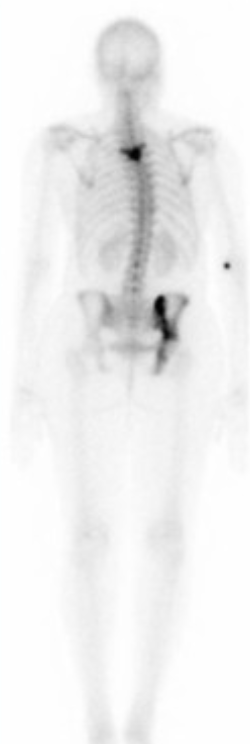
Metastatic disease
Focal area of increased radiotracer uptake
Typically multiple lesions, if a single lesion less likely but still possible to be a met with one exception
A single lesion in the sternum is highly suggestive of metastatic disease
Flare phenomenon
Within first 3 months of chemo there may be increased tracer uptake in osseous metastatic lesions which is a good thing and indicates healing bone but commonly mis-interpreted as progression
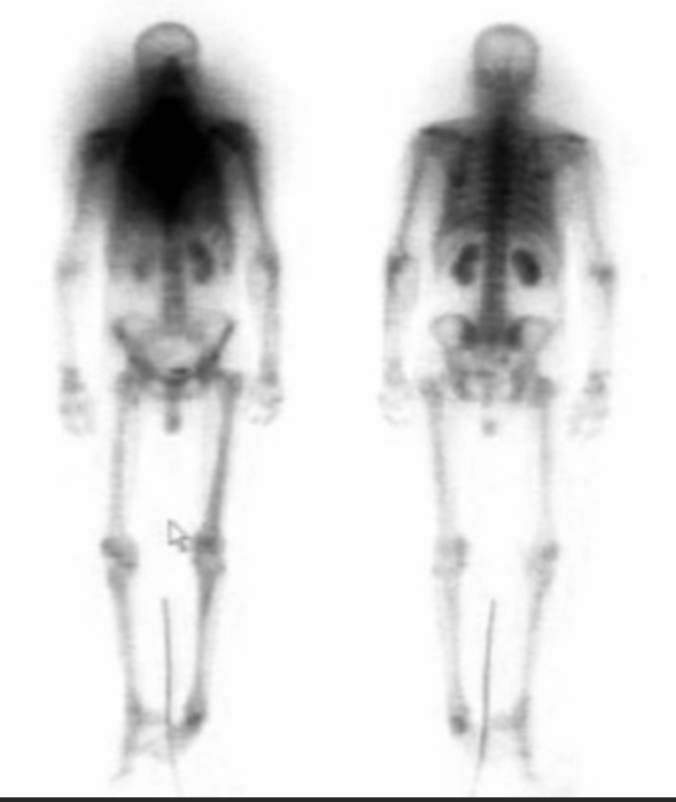
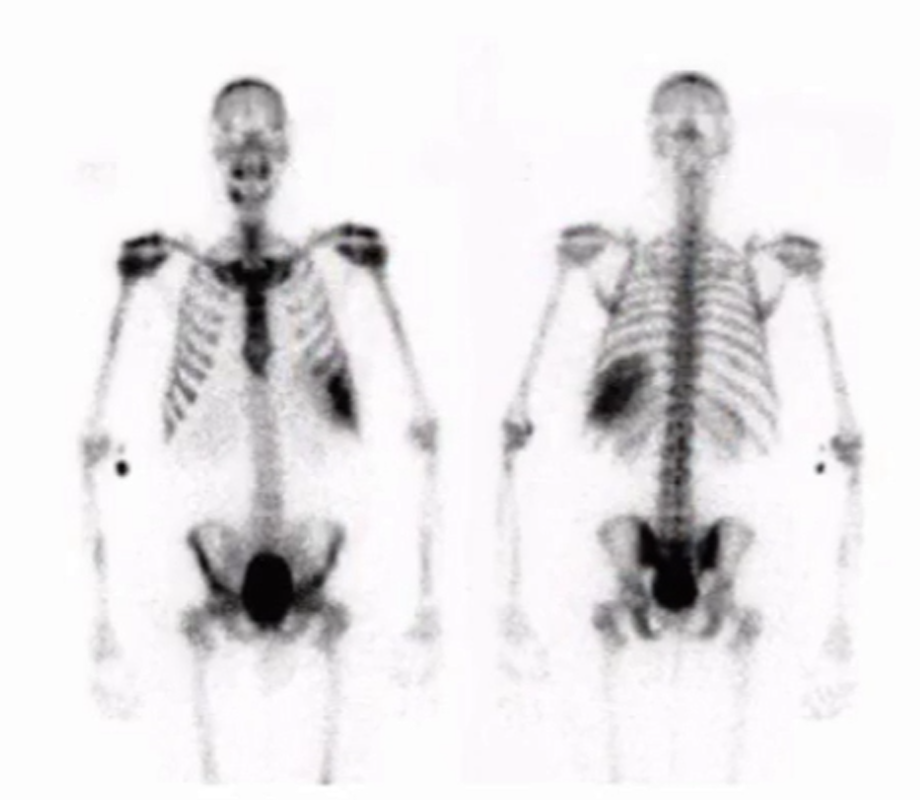
Superscan
Diffuse uniform tracer uptake throughout the skeleton
Will see concurrent decreased renal activity
Most commonly due to prostate carcinoma
Other things looking similar if no cancer —> hyperparathyroidism
Benign bone lesions with intense uptake
Osteoid osteoma - classic case
Fibrous dysplasia
Giant cell tumor
Osteoblastoma
ABC (likely centrally cold with hot rim)
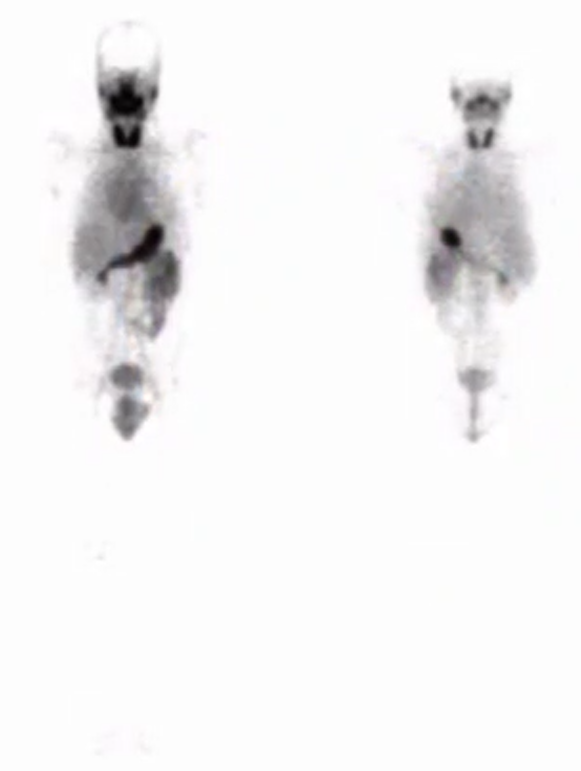
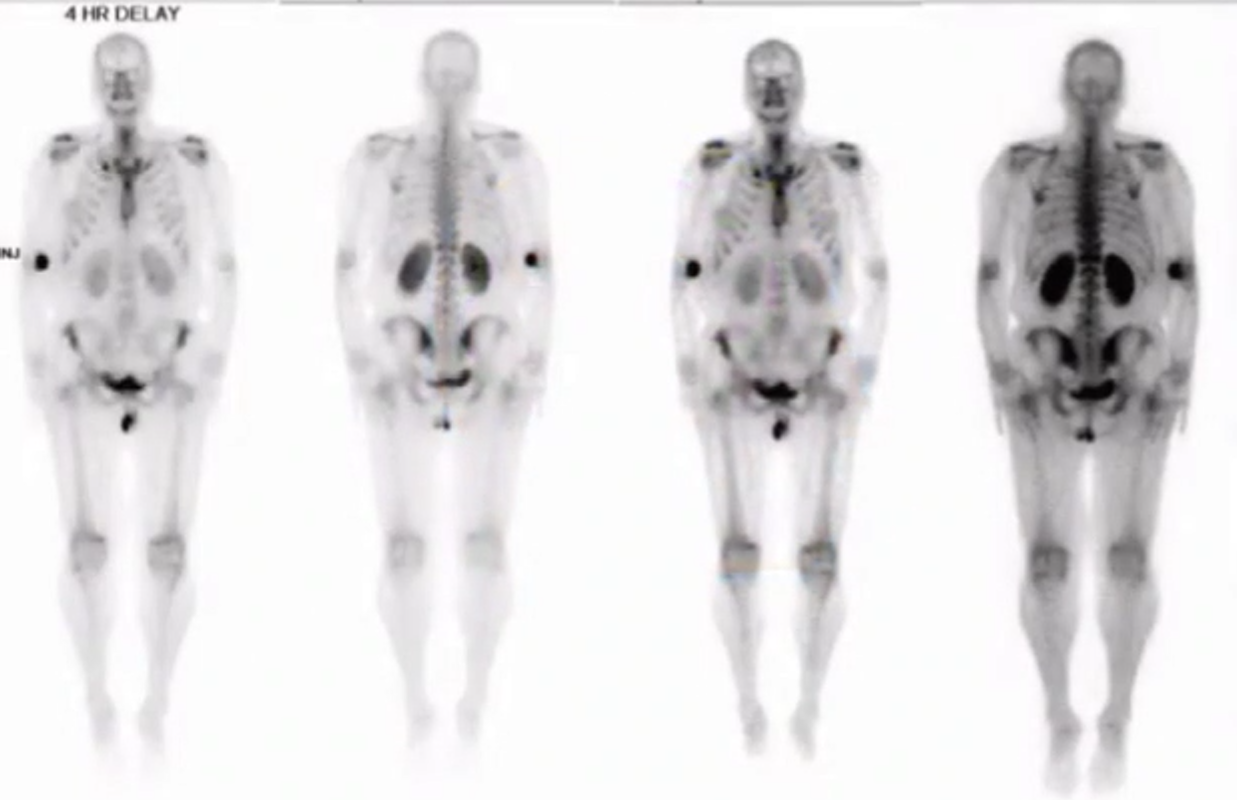
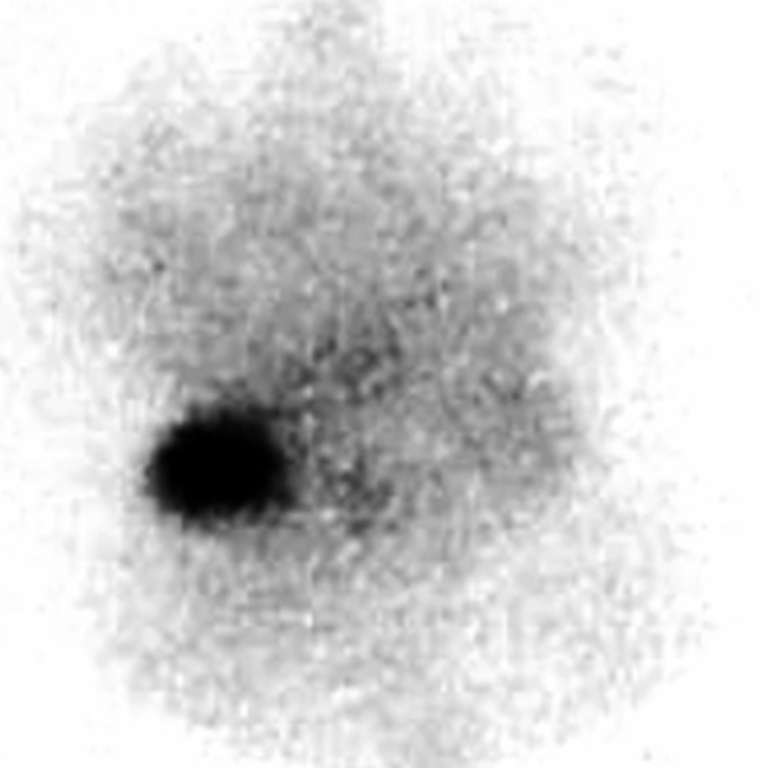
Free Tc
Hardly see bones (no bone uptake)
Uptake in stomach
Uptake in salivary glands
Uptake in thyroid
Arterial Intravasation
Hot glove sign
Radiotracer goes into artery and goes distally (cause arteries push blood distally)
Obviously can have some in vein too

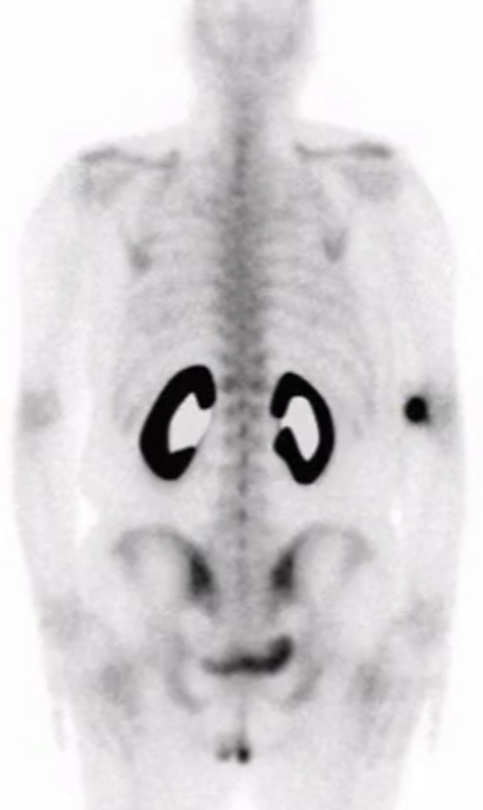
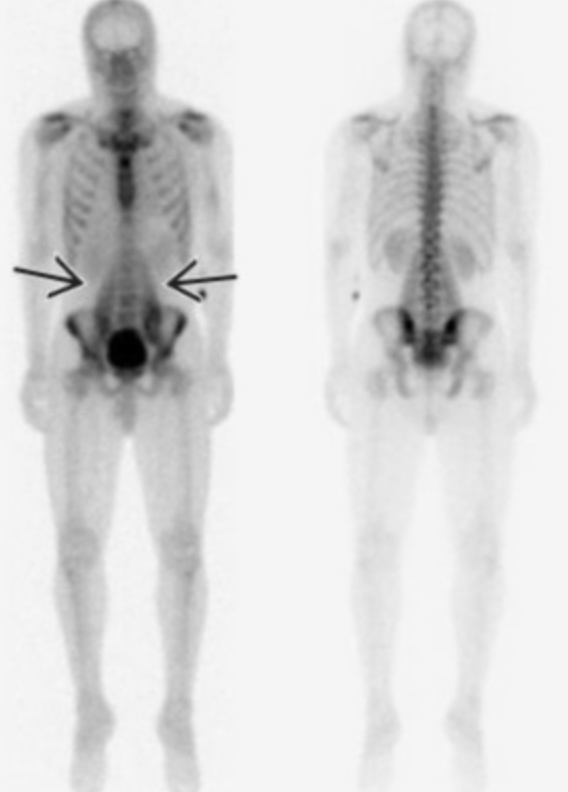
Hot kidneys
Bone scan with very hot kidneys AND whole kidneys are hot not only part of it
Ddx:
Chemo therapy
Urinary tract obstruction
Bone scan and kidneys are hot but only the cortex is hot, not the whole kidney
Hemochromatosis
Note: looks like octreotide study but here you see bones and do not see spleen
Enchondroma
Focal area of uptake in the right humeral neck (inferior and lateral most spot)
The other two areas are degenerative
Get a radiograph and shows rings and arcs

Paget’s Disease
Excessive bone remodeling
Mickey mouse sign
Increased tracer uptake in spine and posterior elements making mickey mouse head type look
Black beard sign
Increased uptake in mandible making it look like a black beard
Fibrous Dysplasia
Enlarged and deformed bone with strong uptake
Plain film will show expansile, lytic lesion with ground glass
MSK Nuclear Medicine
Scaphoid Fracture
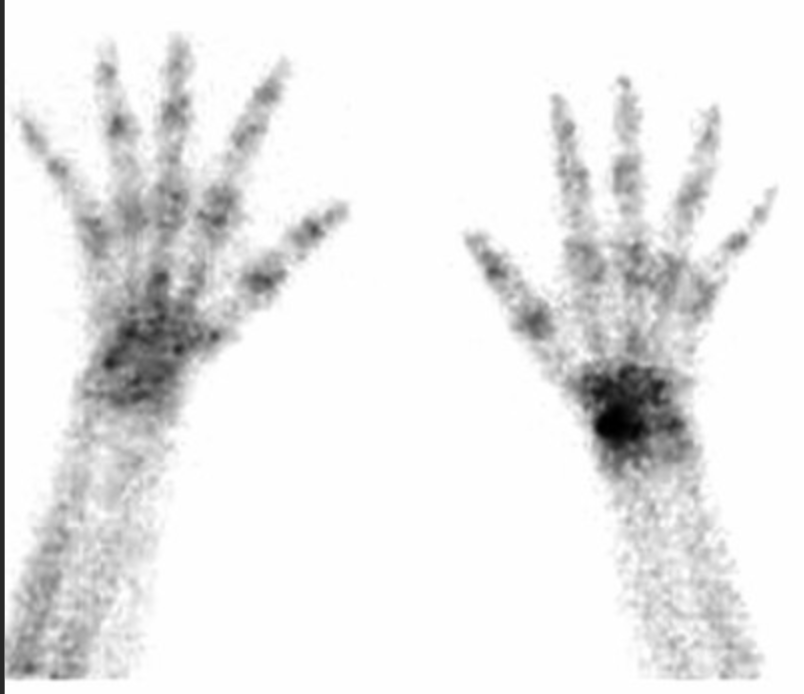

Wrong Window applies
Windows are used to look at and separate true photons and scattered photons
These photons will exclude low energy photons
Here the energy window was set too low so you only get the scatter photons and not the good ones

Myositis Ossificans
Small focal area of uptake in the right lower extremity
Next step - get a CT and you will likely see calcified shit
Bright because MDP gets laid down because of calcification depositing I believe is the MOA

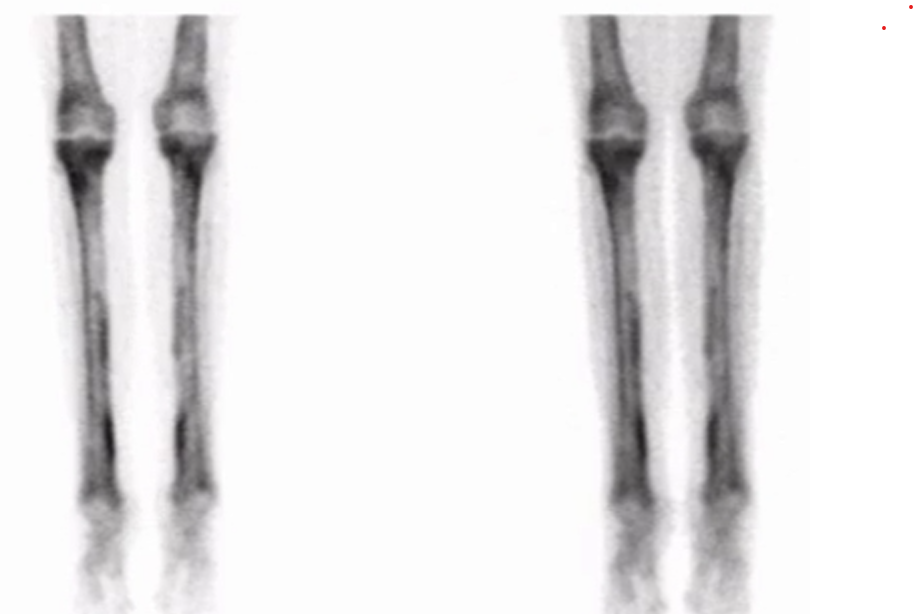
Shin Splints (Medial tibial stress syndrome)
Seen as diffuse uptake in the posterior-medial tibial cortex
Best visualized on the delayed static images
Note: stress fracture will typically have early uptake
Arterial and blood pool images are normal
Recent radioactive tracer adminsitration
In this case for thyroid
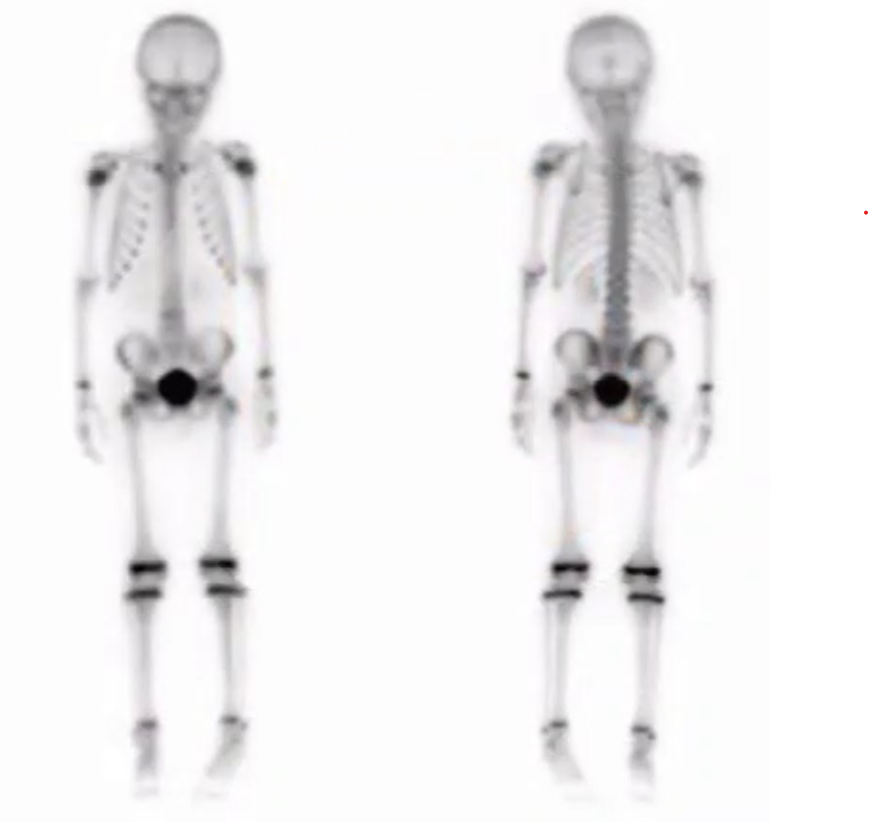
Hardware Loosening
Bone scan is positive in all 3 phases (left)
In-111 WBC scan shows no increased uptake (right)

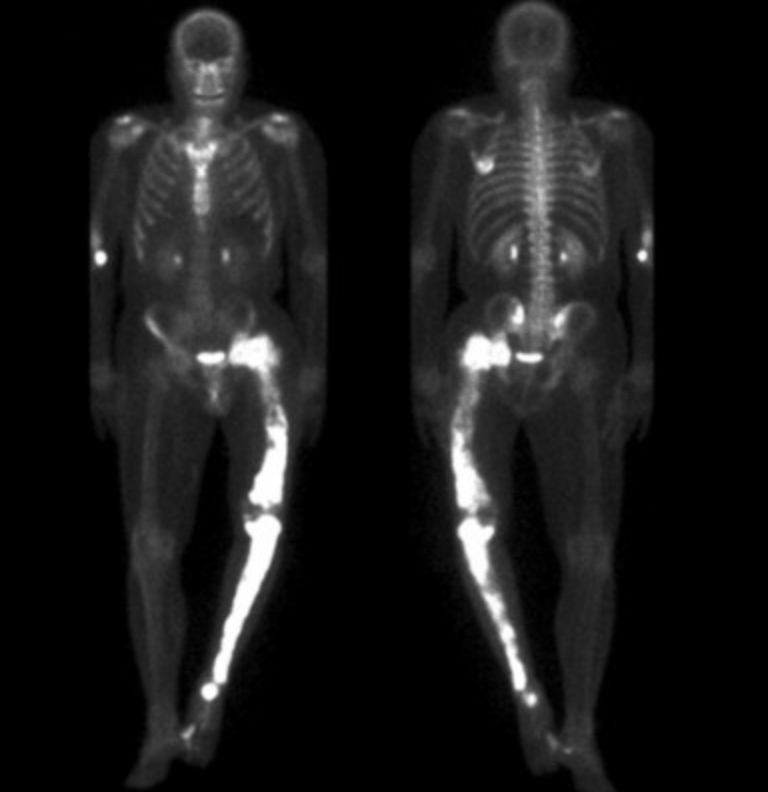
Hypertrophic Osteoathropathy
Look at shins and you will see linear areas of high uptake along periosteum
Called tram tracking
Next step - likely CT chest for lung cancer eval
Other DDx:
Hypoxia, cyanotic heart disease, pulmonary pathology
Sickle Cell
Infarcted spleen
Rhabdomyolysis
Uptake within the soft tisues
Here it is seen with the psoas muscles
Normal kid
Uptake in epiphysis in kids - normal
Osteoid Osteoma
Focal area of uptake in lumbar spine of kid with scoliosis
Double density sign ( basically centrally very hot and slightly less hot surrounding it)
Pain better with NSAIDs, typically pain at night

Osteosarcoma
Focal are of uptake at metaphysis of long bone
Kid - we know because growth plates light up

Multiple Myeloma
Will be hot on PET and normal on MDP
This is because MDP only shows osteoblastic activity which is not present in MM only the destructive part
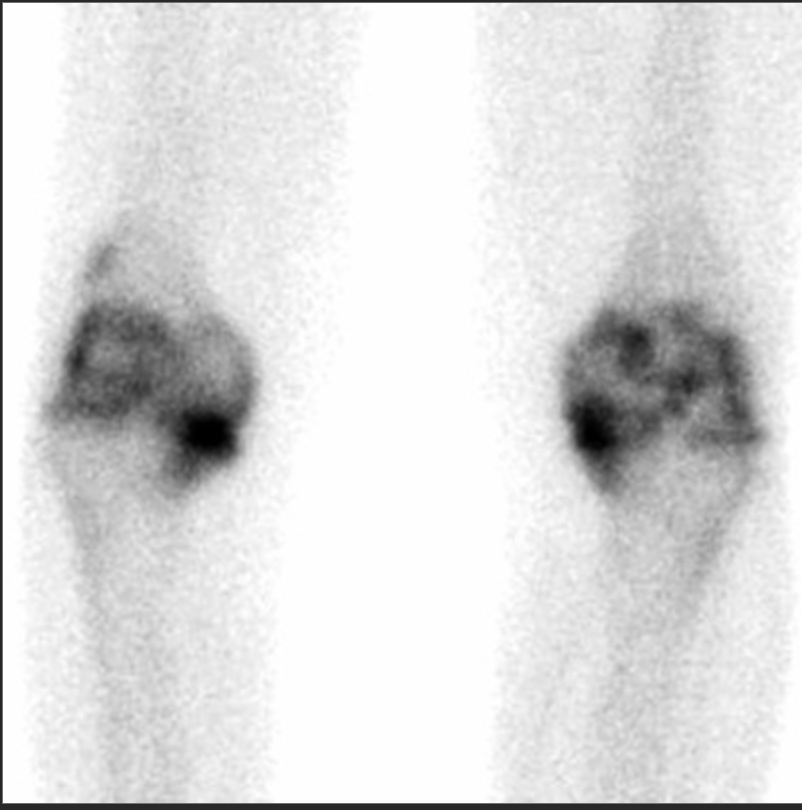
Degenerative Changes
Joint centered uptake, more pronounced medially
Superscan
Diffuse uniform tracer uptake throughout the skeleton
Will see concurrent decreased renal activity
Most commonly due to prostate carcinoma
Other things looking similar if no cancer —> hyperparathyroidism
Resources: