V/Q Scan
V/Q Scan
Tc-MAA (technetium tagged to albumin)
Inhaled radiotracer - shows ventilation
Xenon 133
Short half life - 30 s
Low energy ~80 keV
3 phase - wash in, equilibrium, wash out
Fat soluble
May see uptake in the liver if it is fatty
Tc-99m DTPA
Energy 140 keV
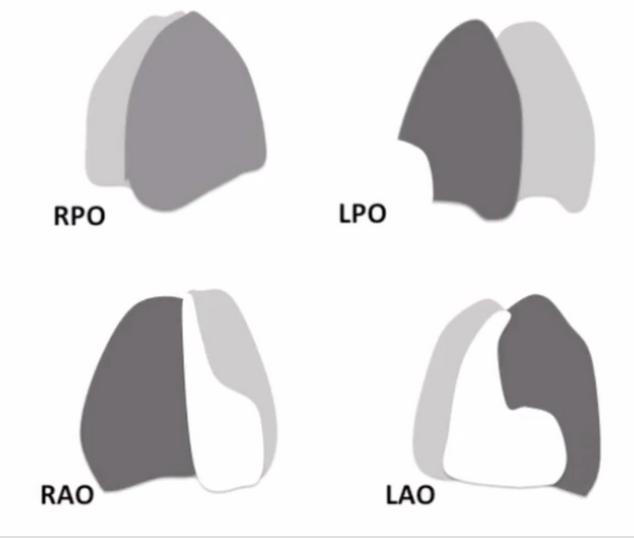
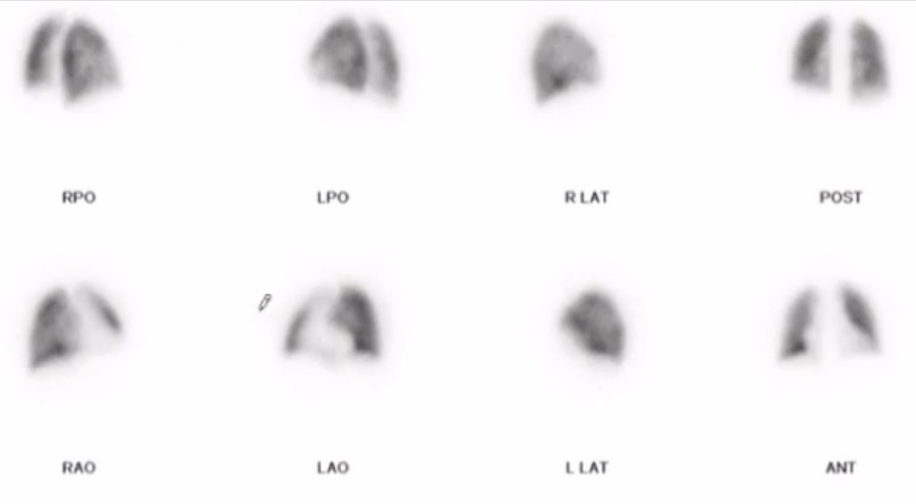
Allows for multiple projections
Tracheal clumping
IV radiotracer - shows perfusion
Tc-MAA (technetium tagged to albumin)
Should stay in lungs because it basically gets trapped into capillaries in lung
See radiotracer in brain
Look for shunt
Downscatter
Lower energy tracers have to be used first
This is because the one with the higher energy will basically decay into the values of the lower energy one and won’t know what the real shit is
So for this, the Xenon has to be used before the Tc (the inhaled before the blood portion)
When should radiotracer particle amount be decreased
Does not mean reduce the dose
Basically a more concentrated dose i guess
Basically the particles get stuck in and block off the capillaries and don’t want to block more than 0.1% of capillaries
So situations where there are less capillaries require less particles such as:
Kids
Lung resection
Pulmonary hypertension
Known shunt
Normal to have
Perfusion slightly less at top of lungs (hence hematogenous shit goes to base of lungs)
Ventilation slightly less at bottom of lungs (hence airborne shit goes to top of lungs)
PE
Normal ventilation
Wedge shaped area of perfusion decrease (typically in periphery)
Normal perfusion essentially excludes a PE regardless of findings on ventilation portion
PIOPED Criteria
Criteria for reporting liklihood of having a PE
Very low = <5 %
Low < 20%
Intermediate = <80%
High = > 80%
Must have a CXR before doing
Size
Described as a fraction of the segment
Small = <25% (do not add the smalls)
Moderate = <75%
2 moderate = 1 large
Large = > 75%
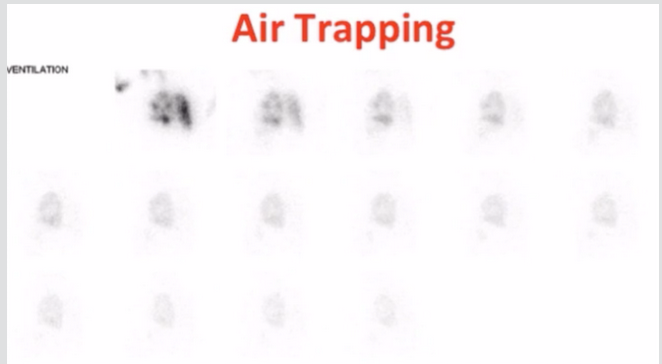
Air Trapping
Will see slightly increased radiotracer uptake in the base of the lungs rather than the apex (note should normally be slightly high inhaled radiotracer in the lung apex)
This is for the ventilation portion
Not super obvious
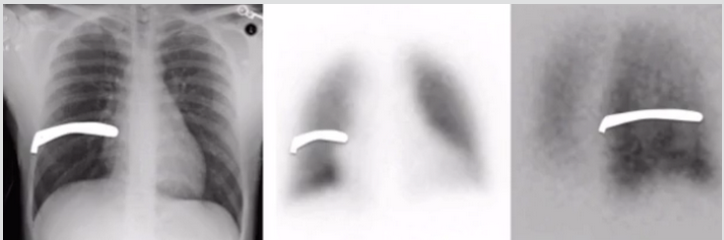
Complete lack of uptake in one lung
Complete lack of perfusion in one lung
DDx
Hilar mass
Hypoplastic pulmonary artery
Mediastinal fibrosis
If you see complete lack of perfusion in one lung and normal ventilation that is a cancer eating into the artery
Complete lack of ventilation in one lung
NOTE: Foreign body in mainstem bronchus will not cause whole lung mismatch
This is because there is hypoxic vasoconstriction leading to decrease in blood flow to the non-ventilated lung so the decrease in perfusion and ventilation is the same
Fissure Sign
Fluid in fissure causes defect
No PE present
References:
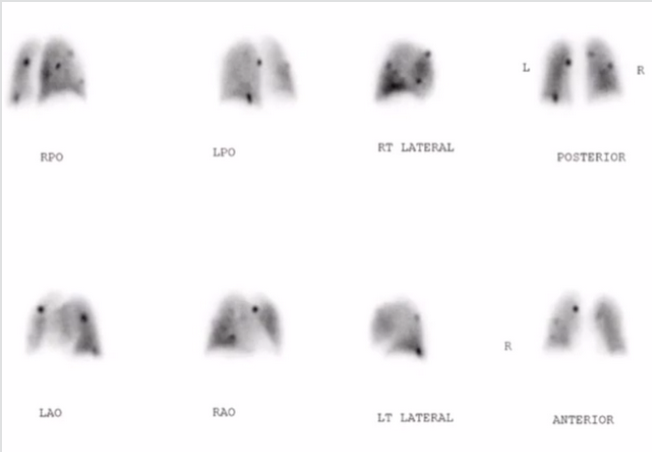
Clumping
Basically multi-focal hot spots throughout lungs
Seen when person injecting draws back on syringe and causes radiotracer to clump
No other cause
Triple Match
Defect seen on CXR, ventilation & perfusion scans
Triple match in lower lobe = Intermediate risk
Triple match in upper lobe = low risk