PET/CT
Standardized Uptake Value (SUV)
How much radiotracer has been taken up by the tissue
SUV activity concentration in tissue / injective activity aka body size
SUV max
Highest value in the voxel regardless of size
more susceptible to noise
SUV mean
Averages value from multiple voxels of the region of interest
Less sensitive to noise
Factors Affecting Quantification of Tracer Uptake
Weight & Body size
Blood glucose
Post-injection uptake time
Respiratory motion
Technical factors associated with obtaining the image itself (FOV, use of contrast, etc.)
Protocols
All PET/CTs should include these
Non-attenuation corrected
Regular body CT
Attenuation corrected PET series
Protocols
Skull base to mid-thigh
Vertex of skull to mid-thigh
Whole body
Mechanism of Action
FDG-glucose will not undergo glycolysis
The amount of glucose in cell is regulated by two items
Number of GLUT transporters
Level of hexokinase in the cell
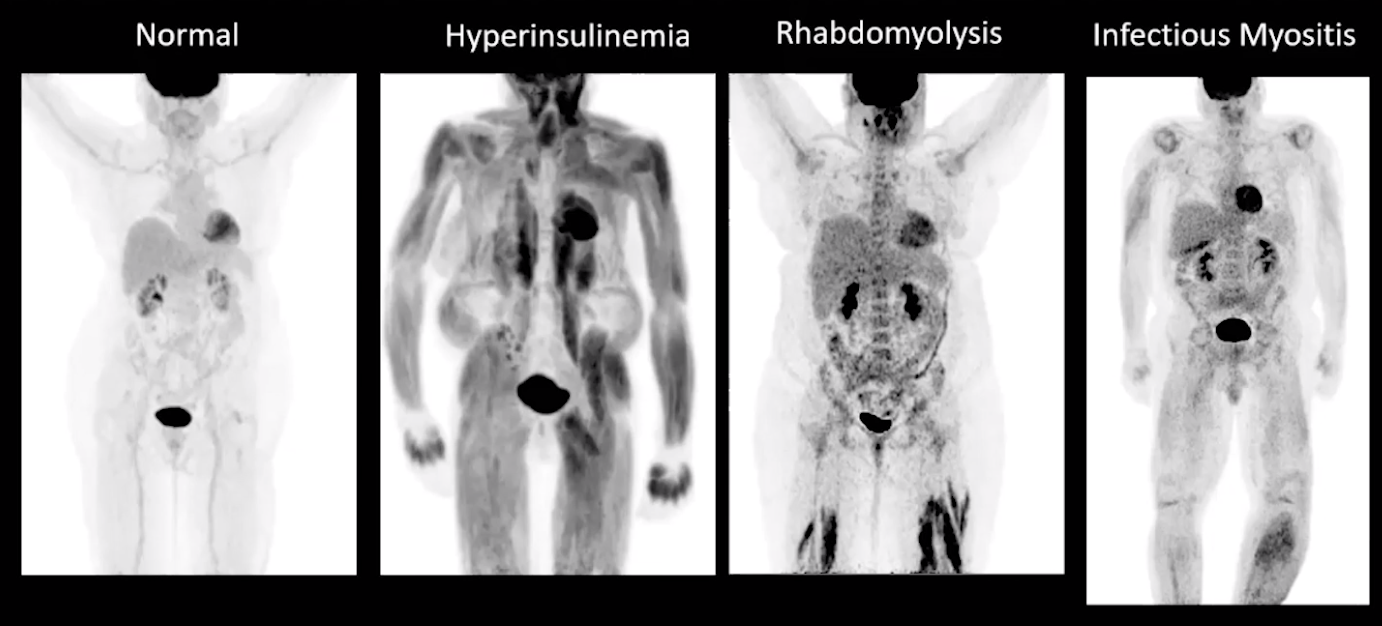
Insulin causes increased muscle uptake of glucose
Need to time the insulin use in diabetics before PET is obtained
Note you can have hyperinsulinemia with a normal glucose level, classically if a person recently ate a few hours before the exam the glucose will likely be normal but insulin will be high
Ideally want glucose between 70-200
When insulin is high then the glucose will be diverted to other areas and falsely dilute its transport to the cancer so even if the cancer is hot it is likely not as hot as it should be because the glucose tracer is being diverted to muscle and other areas
Avoid exercise at least a day before scan —> causes increase glucose uptake by muscles
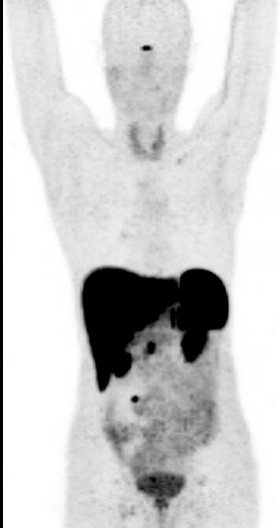
Normal Distribution of FDG-PET
Highest uptake in brain
Higher in gray matter
White matter only has axons so no glucose transporters present and therefore lower uptake
Low levels of uptake
Blood vessels
Salivary glands
Lymph nodes
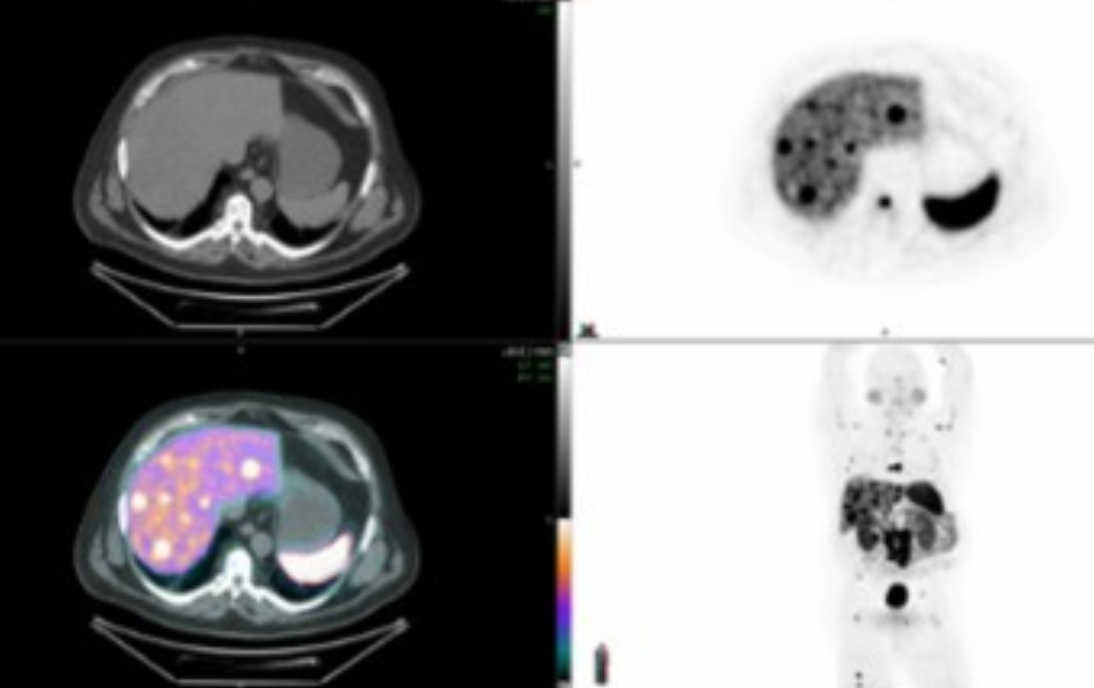
Uptake in liver used as the background level of metabolism
Spleen should be equal to or lower in level of uptake compared to the liver
Kidney
Will have high levels in collecting system
If have kidney disease may not have any in collecting system
FDG Patterns of Bone
Diffuse, homogenous uptake in bone
Look for G-CSF use —> stimulate bone marrow
Spleen will also typically have diffuse uptake as it is stimulated by these drugs too
Size of spleen is typically normal if the diffuse uptake is caused by the drugs
If diffuse uptake and enlarged consider lymphoma
Diffuse, heterogenous, multifocal in bone
Look for lymphoma
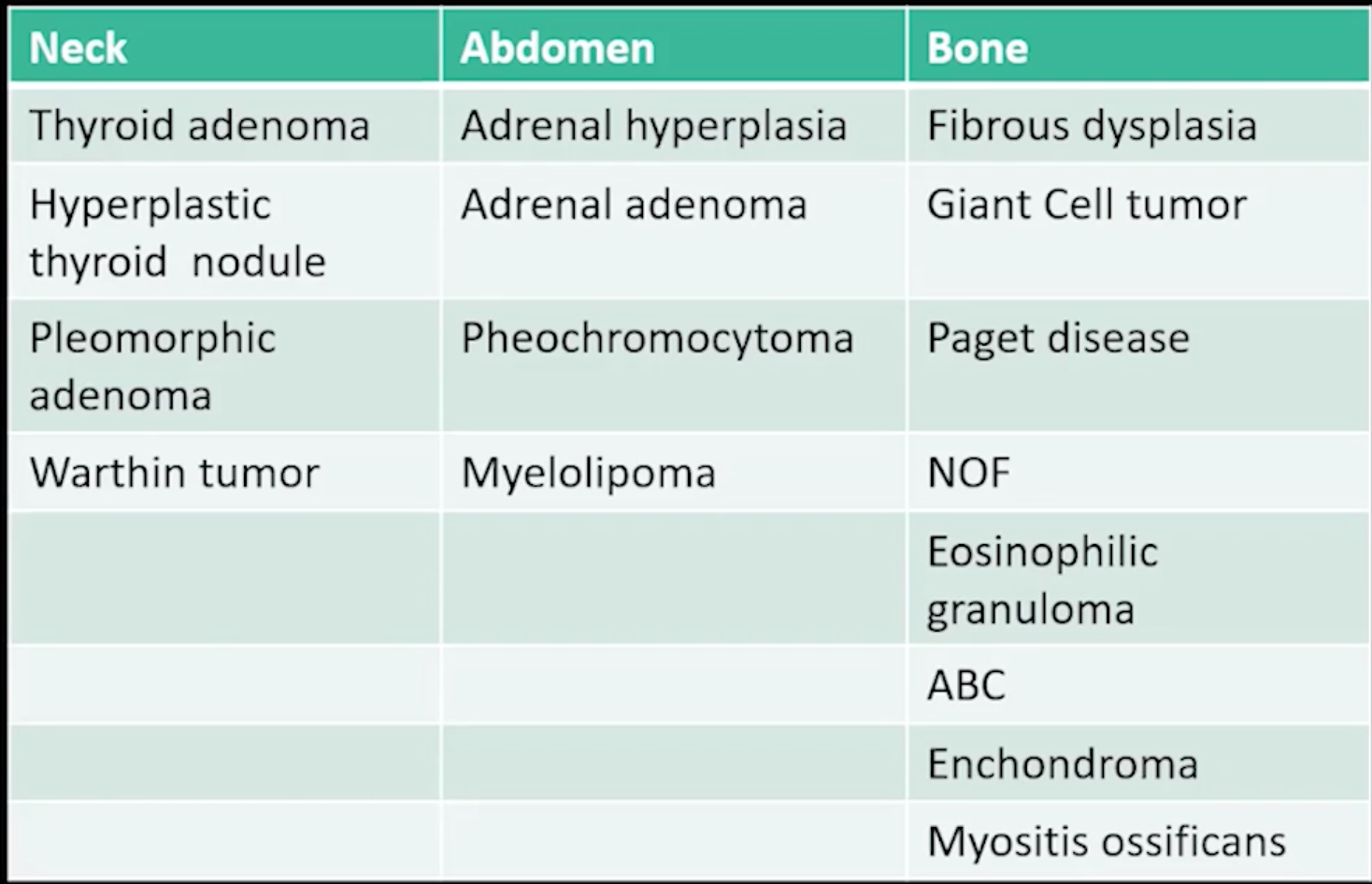
Benign Findings & Pitfalls
Benign Lesions which may have increase tracer uptake
Lipomatous hypertrophy of the interatrial septum
Increased radiotracer uptake between the right and left atrium
This is a focal area of brown fat
Nothing to do about this, no follow up
Can be hot on one study and not hot on another, doesn’t matter its fine, leave it alone
Pleurodesis
Will be FDG-avid basically from chronic inflammation
Will see associated density on the non-con
Mesothelioma may look similar but should be more nodular and throughout the pleura, and should also typically be bilateral
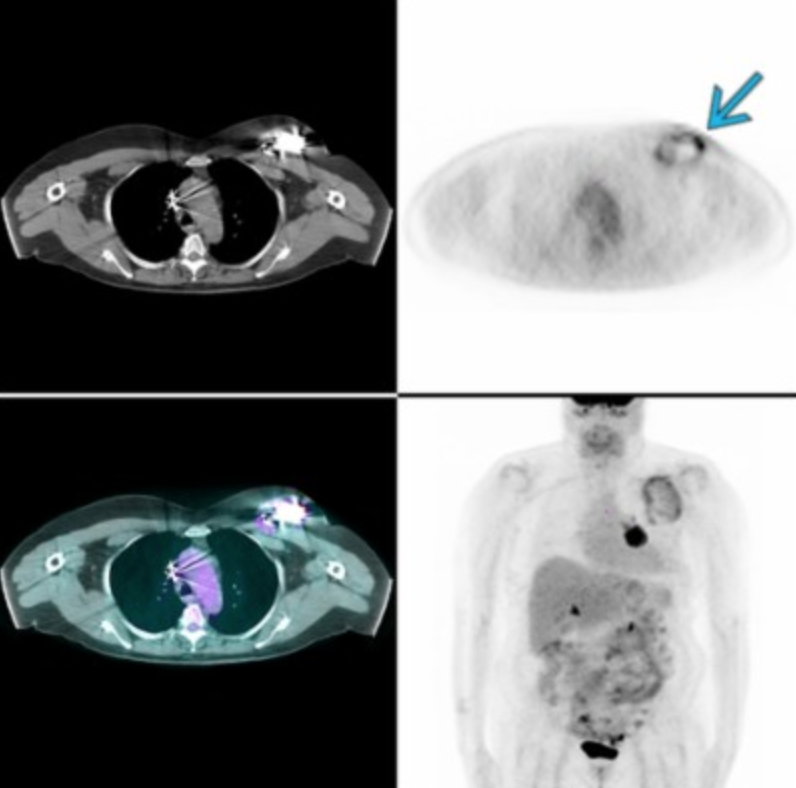
Thymic uptake/Thymic Rebound
Looks like bright shit over the heart
Normal in kids and young adults
DDx:
Lymphoma - should be very hot, thymic uptake should be luke warm
Vocal Fold/Cord
Focal unilateral uptake within the vocal fold/cord is likely secondary to entrapment of the recurrent laryngeal nerve caused the contralateral side to work harder and therefore have increased tracer uptake
Same phenomenon can be seen with radiation changes to the chest/mediastinum/neck region
Lung
GGO + hot on PET —> infection/inflammatory
GGO + cold on PET —-> Broncheoalveolar carcinoma
Infected ICD
Post-treatment
Don’t want to early after treatment —> stunning
Don’t want to late after treatment
Chemo
Need to wait 2-3 weeks after last chemo to get PET
Radiation
Need to wait 8-12 weeks after last radiation to get PET
Note that when looking at mass vs radiation necrosis in CNS, if the PET is hot then it is mass recocurance even if the mass is not well seen on the MR or if there is a bunch of FLAIR signal or other shit making it hard to see
Radiation necrosis will show no uptake on PET BUT, in the immediate 2-3 weeks following radiation therapy there will likely be increased uptake due to inflammatory hypermetabolism
Brown Fat
Mostly seen in the neck, cervicothoracic paraspinal soft tissues, clavicular region and mediastinum
Can also see in peri-renal area (looks like adrenal gland but obv is not the adrenal gland)
When determining if brown fat or abnormal look for
Symmetry
Look for no lesions and just fat on the regular non-con CT
Look for no surrounding abnormal LN
How to reduce this
Keep room warm
Give benzodiazepines - shuts down pathway
Key Notes:
For non FDG PETs (Dotatae and PSMA), the SUV has nothing to do with actual tracer uptake it has to do with cell surface receptor level
So the worse the cancer gets, the more amorphous and fucked up the cells become so they no longer look like the normal organ tissue and therefore SUV will decrease
For stating disease progression
Needs to be >20% increase in size and > 5mm increased —> BOTH
What is PET good at vs MR and Contrasted CT
Solid organ mets —> PET is best
Vascular invasion and peritoneal carcinomatosis —> CECT is best
Shit in brain —> brain is best
Tumors that are PET cold
Broncheoalveolar carcinoma
Carcinoid
Islet cell tumors
RCC
HCC (varies)
Has enzyme that removes phosphate which makes FDG not bright or some shit
Prostate
Anything mucinous
Thyroid Uptake
Diffuse uptake —> Hashimoto
Focal uptake —> anything (cancer or anything)
Need to get US
References:
Brown fat
Lipomatous hypertrophy of the interatrial septum
Chronic inflammation
Pleurodesis
Osteoarthritis
Metallic artifact
Fractures
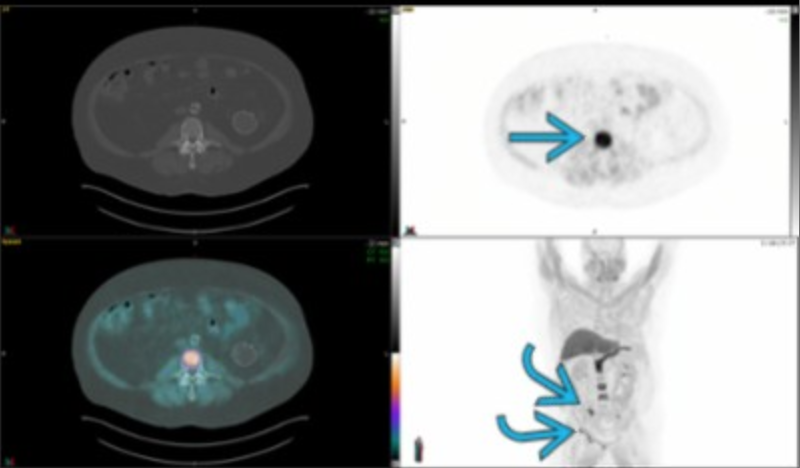
Metformin use
Causes uptake of glucose within the bowl
Will be see as intense FDG avidity throughout the bowel
Doesn’t have to be seen in all parts of the bowel but will be relatively dense for a significant portion
Affects both small and large bowel
DDx:
Colitis - not as continuous
Growing Nodes
Obviously follow the Recist study
Key note: If you see a node that has grown and has increased or new radiotracer uptake in a short period of time and the patient has a history of lymphoma there should be concern for transformation of type of lymphoma (SLL —> DLBL for example)
Kidney Uptake
Mostly normal
Abnormal lesion that is hot
Most likely oncocytoma
Abnormal lesion that is cold
RCC
Opposite of above can also be seen but this is most common finding
Testicles
Mass that is hot —> seminoma
Mass that is cold —> non-seminoma
Cases

Carcinomatosis
Ga 68-Dotatate PET
General
Basically a somatostatin analog
Used to evaluate for
Neuroendocrine tumors
Meningiomas
Sarcoid
Compared to FDG PET
No brain uptake
+ uptake in pituitary gland (looks like Indian bindi)
Spleen also hot
Physiologic uptake in adrenal glands, liver, pancreas, spleen
Note that in pancreas it is in uncinate process, so looks somewhat focal normally - question asking what part of pancreas so need to know
Axumin (F-18-Fluciclovine) PET
General
Special PET used in patients with prostate cancer who have previously had radiation therapy or prostatectomy to look for recurrence
Lytic lesions tend to have strong uptake and sclerotic lesions tend to have little to no uptake
If there is a sclerotic lesion with no uptake then you need bone specific evaluation with skeletal scintigraphy
Homogenous and diffuse uptake in the pancreas is a normal finding, do not be tricked into picking pancreatitis
Spine and pelvic mets
Ovaries
Pre-menopause ovaries —> ok to be hot
Post-menopause ovaries —> should be cold
If hot, question cancer
Carcinomatosis