Tagged RBC Scan
General
For active bleeding of mid to lower GI system
Tc-99m-RBC
Dose
Adult = 15-30 mCi
Children = 0.3 mCi/kg (minimum 2, max 20)
Detection of 0.1 ml/min
Images typically obtained for 60-90 min
Image rate not to exceed 1 min (too slow)
Bilateral photopenic areas with central hazy area of increased uptake = ascites with centrally located bowel
Bleeds
Angiodysplasia
Typically in cecum/right colon
Typically should see cluster of small vessels at the bleeding site on angio
Diverticular bleed
Typically in sigmoid/left colon
Management
If patient is stable —> endoscopy/colonoscopy
If patient is unstable or management cannot be done with endoscopy —> Angio
In Angio typically will use coils
Want coils to be placed as far distally as possible because
Prevent collateral vessels from also supplying the bleed
If you go to proximal the area of ischemic bowel will be large and you’ll kill all the bowel
Particulate embolization is typically contraindicated in lower GI bleeds due to risk of bowel ischemia
Diverticular Bleed
Notice extravasated blood in left colon

Technical Points
Look at the first pictures and follow normal course, do not just skip to the end. If you skip to the end and there is a bleed you will definitely see blood but you will think the bleed is in the distal colon because that is what the last pictures are taken of. However you can have a bleed in the more proximal bowel which will be seen on the earlier studies and because of normal bowel peristalsis it will carry blood to the distal bowel and you will be fooled into thinking the bleed is more distal than it actually is.
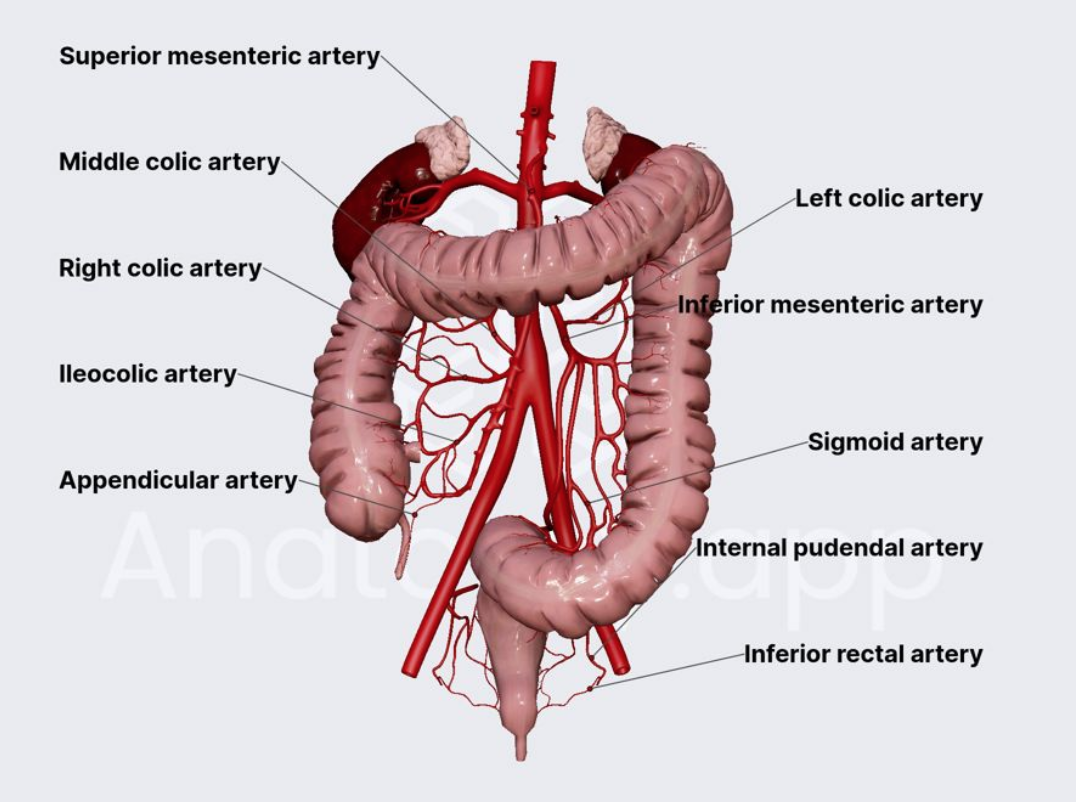
Need to be able to identify the vascular distribution and what portion of bowel the bleed is from
References: