Neuro Nuclear Medicine
General Neuro Nuclear Med
Brain
3 Major types of imaging
Planar
Uses perfusion agents
Really only brain death studies fall under this category
2 phases
Dynamic/Angiographic phase —>many rapidly acquired of the arrival of the tracer —> shows brain perfusion basically
Done 2-3 sec after administration
Delyaed static phase —> show distribution of tracer and can make note of place it is (and should not be) or should be (and is absent)
Done 15 min after administration
SPECT brain perfusion imaging
Uses lipophilic agents that can cross BBB —> can enter brain tissue in same proportion as normal blood supply to area would
PET
Brain Death Study
Form of planar imaging
Radiotracers used
Tc-99m - DTPA OR Tc-99m-pertechnetate —> Transient perfusion agent —> preferred agents to be used for brain death study
If you see some faint tracer over what looks like the brain, it is not actually uptake in the brain because it cannot cross the BBB, it is actually uptake in the scalp which is projected over the brain
Can put a rubber band around the scalp to pinch off blood supply to it is not mistaken for brain activity
Tc-99m pertechnetate only —> choroid plexus will normally have tracer uptake
Tc-99m - HMPAO —> Perfusion agent extracted by brain on first pass —> not typically used
Trident sign
Should see a 3 pronged structure shortly after administration of tracer —> Middle cerebral artery + both MCAs
Positive study
Tracer uptake in carotids up to skull base and then none after due to compression from cerebral edema
NOTE: Need to evaluate that there is tracer uptake in the common carotid to show that a good bolus was given
If there is not significant tracer uptake in the common carotids then the bolus was likely shit and study needs to be redone
Hot nose sign —> basically maxillary branch of external carotid artery is still patent and supplies the face which may be hot, can still be brain dead with this
Brain SPECT
Agents
Uses lipophilic agents that can readily cross the BBB and be retained by brain parenchyma in proportion to their cerebral blood flow
Tc-99m-HMPAO
Uptake and metabolism is highest in gray matter
Uptake is proportional to cerebral blood flow
Excretion through intestines & kidneys
Tc-99m- ECD
Technique
Tracer injected IV
Seizures
Seizure Studies
Ictal & Inter-ictal
Ictal studies
Done while having the seizure
Use Tc-99m-HMPAO or Tc-99m-ECD
Ictal is more sensitive that inter-ictal
CSF Leak Study
Intrathecal administration of In-111 DTPA
Nasal pledget placement
Serum blood draws are obtained at intervals determined by the radiologist
At the same time that the blood is drawn the nasal pledget counts are also obtained
Serum blood is counted so that you can get a ratio of the nasal pledget to serum pledget
CSF pledget to serum ration of 1.5+ = positive test
Imaging
Prep for SPECT in suspected dementia
Ensure patient is in a dimly lit and quiet room
Patient is not to speak or read
You are not to interact with the patient before, during or 5 min after the procedure
They can have eyes open tho…idk it was a question
3 types of PET that can be used in dementia evaluation
FDG
Hypometabolism in fucked up areas
Amyloid
Diffuse uptake in abnormal cases
Tau
Deposition where there is atrophy
FDG PET
1 = normal
2 = Bilateral parietal lobe decreased uptake
3 = Bilateral frontal and temporal lobe decreased uptake
4 = Alzheimer pattern + occipital lobe involvement
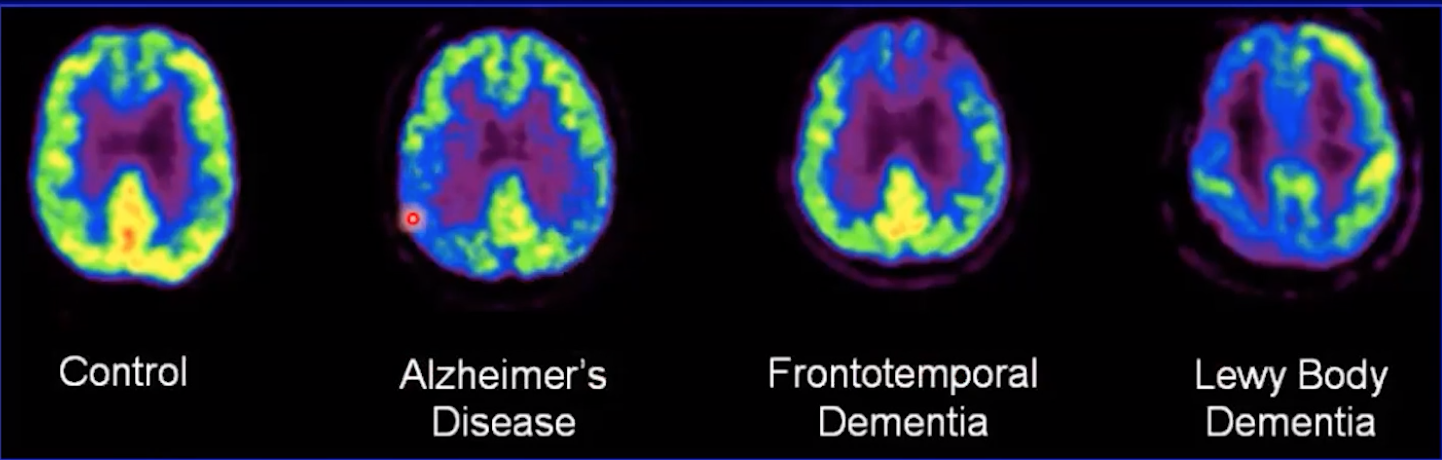
Fronto-temporal dementia
MRI will show atrophy of
Frontal lobe
Temporal lobes
Anterior cingulate gyrus
FDG PET Hypometabolic Areas
Same 3 as above
Negative amyloid PET
References:
Dementia
Alzheimers dementia
MRI will show atrophy of
Hippocampus
Parietal lobes
Posterior cingulate gyrus
FDG PET Hypometabolic Areas
Same 3 areas as above
Amyloid PET
w=Extracellular
Will be positive 20 years before symptom onset
Tau PET
Intracellular
Predicts the location of future atrophy
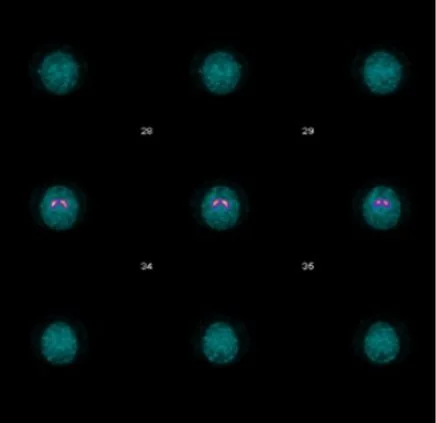
I-123 loflupane study
Used to assess for parkinson’s and adjacent shit which appears to almost walways be progressive supranuclear palsy and multiple system atrophy
Appears to be used when there is a tremor and want to see if from parkinson’s or some other shit
I-123
Decay by electron capture
T1/2 = 13 hours
159 keV
Dose = 5 mCi
Has high affinity for dopamine transporters (DAT), typically in striatum region
Normal study = bilateral comma shaped shit in putamen region (pic to right)
Parkinson’s Disease
I-123 loflupane study
Lewy Body dementia
MRI will show atrophy of
Occipital lobe MOST
Also some temporal, parietal, PCG (AD pattern)
FDG PET Hypometabolic Areas
Same 3 as above