Hepatobiliary nuclear medicine
HIDA
Used to evaluate for cholecystitis typically
Bilirubin is transported in the blood bound to albumin
Then removed from albumin by hepatocytes
Secreted into bile canaliculi and cleared by biliary tree into the bowel
The IDA compounds will follow a similar pathway
HIDA
DISIDA
Technique
No food for 4-12 hour
Narcotics must be stopped 6-12 hours before test
IV inject 5-10 mCi Tc-99m IDA
Take 1-5 min frames for 60 minutes
If at the end of 60 minutes the gallbladder is not filled
Do delayed imaging up to 4 hours after the original hour
Give morphine IV (0.04 mg/kg over 1 min)
If you need GB ejection raction
Give CCK IV (0.02 ug/kg over 10-30 minutes) then take dynamic images over the next 30 minutes
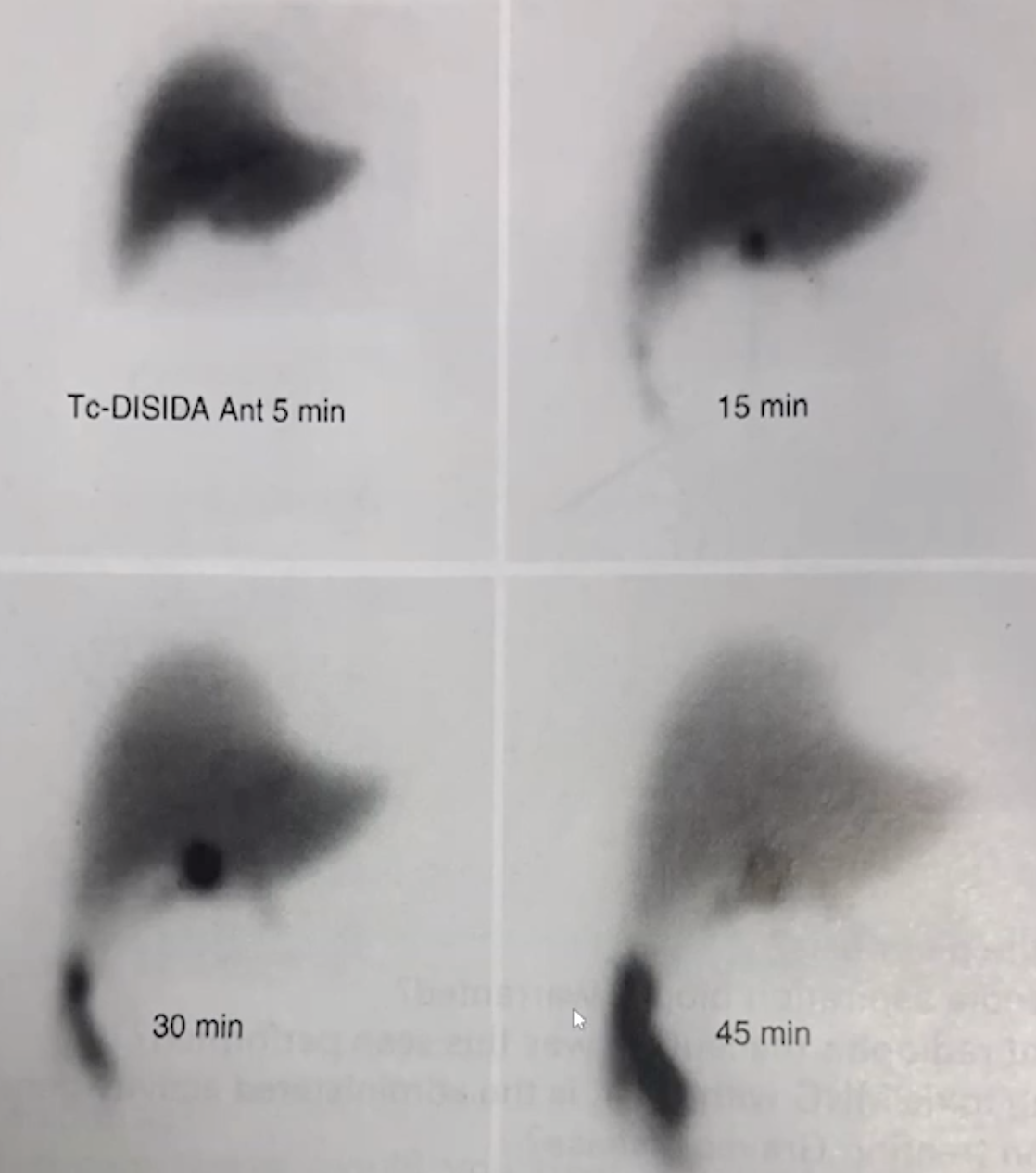
Normal scan
Liver is well visualized by 5 minute
Heart disappears after 10 minutes (earlier is ok)
IDA will then begin to be excreted from the liver into the bile ducts and the liver will begin to decrease in visualization and the bile ducts will begin to be visualized
GB will be visualized within 60 minutes
Note that 2/3 of biliary flow will by pass the GB and go straight t to duodenum
Normal GB EF is >35%
Abnormal study
Typical cause of acute cholecystitis is going to be an obstructive stone
Causes inflammation of GB which then cannot take in the radiotracer
If GB not seen after 1 hour —> get delayed images or use morphine
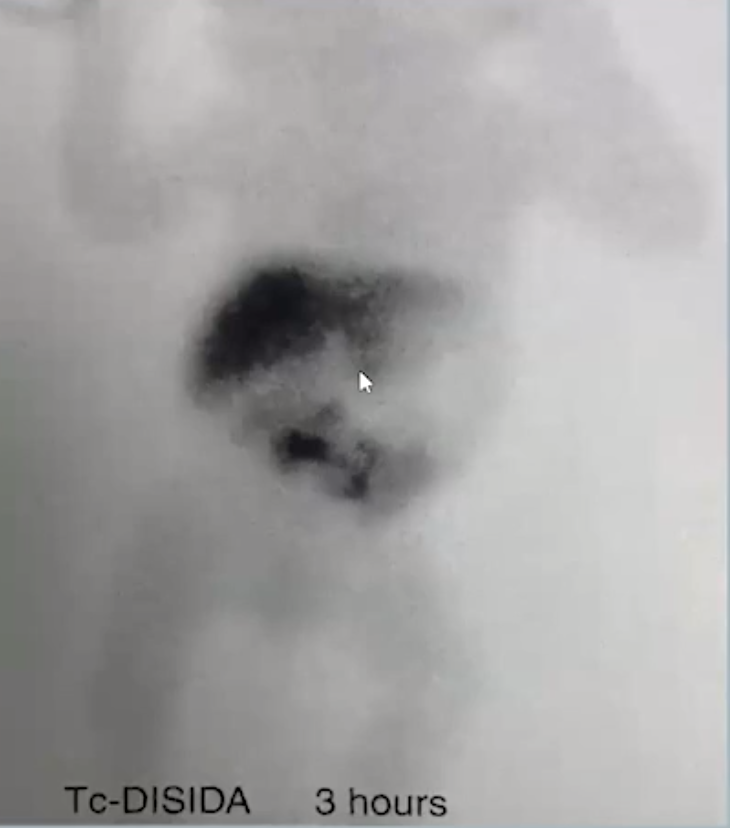
Acute cholecystitis
GB fails to fill (GB not visualized) after 4 hours
GB not visualized within 30 minutes after morphine is given
NOTE: You can still see the tracer in the CBD and in duodenum, just will not see the GB
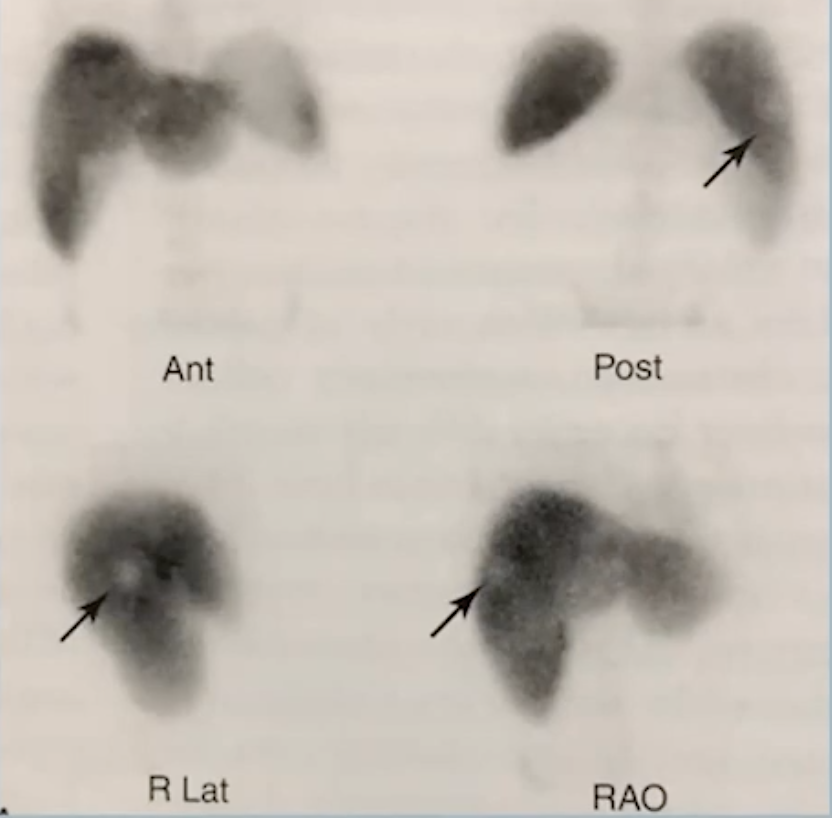
Rim sign - increased radiotracer activity in the areas of liver surrounding the GB fossa
A positive rim sign is associated with a 40% chance of perforated or gangrenous gallbladder
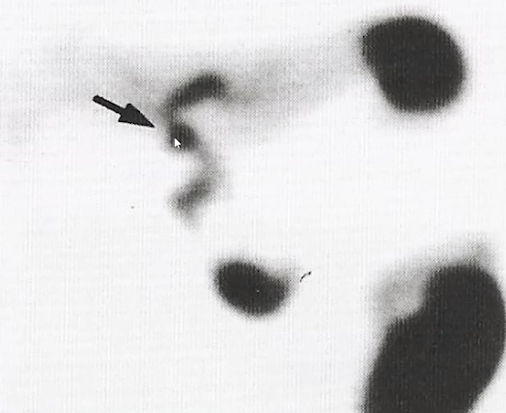
Cystic Duct sign
Focus of increased tracer uptake in the cystic duct proximal to the site of the obstruction
Shit just gets backed up I guess and accumulates making this pronounced focus of uptake
Chronic cholecystitis & Biliary Dyskinesia
Findings below are characteristic but ultimately nonspecific
Normal routine scan
GB EF < 35%
Delayed GB visualization beyond 1 hour
Acute Cholecystitis
GB fails to fill (GB not visualized) after 4 hours
GB not visualized within 30 minutes after morphine is given
NOTE: You can still see the tracer in the CBD and in duodenum, just will not see the GB
Cystic duct sign (top pic)
Focus of increased tracer uptake in the cystic duct proximal to the site of the obstruction
Shit just gets backed up I guess and accumulates making this pronounced focus of uptake
Rim sign (bottom pic)
Increased radiotracer activity in the areas of liver surrounding the GB fossa
A positive rim sign is associated with a 40% chance of perforated or gangrenous gallbladder
Chronic Cholecytitis & Biliary Dyskinesia
Findings below are characteristic but ultimately nonspecific
Normal routine scan
GB EF < 35%
Delayed GB visualization beyond 1 hour
Pediatric HB NM
Typically done in kids with jaundice to differentiate between biliary atresia and neonatal hepatitis
5-7 days of phenobarbital may be used to help diagnosed because it stimulates biliary excretion from the liver
Biliary Atresia
Increased tracer uptake in liver but none in bile ducts or small bowel
Image is garbage but basically shows uptake in liver and none in bowel
Imaging should be performed for 24 hours
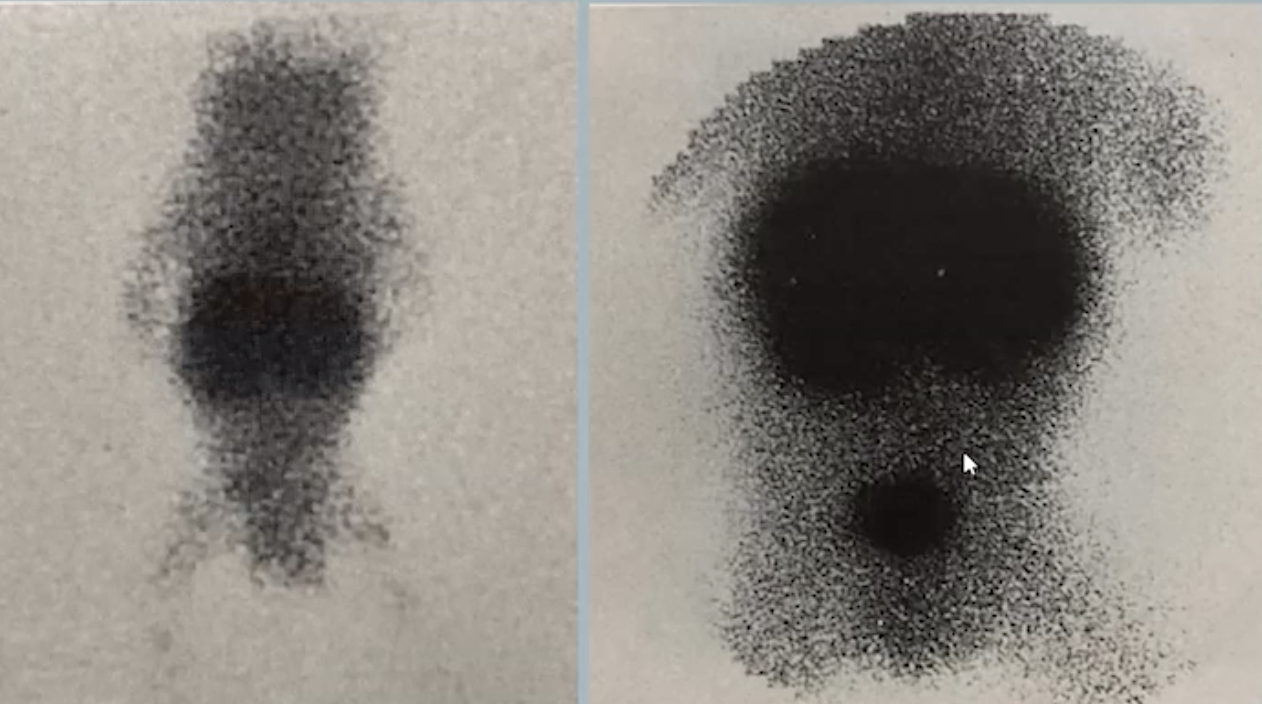
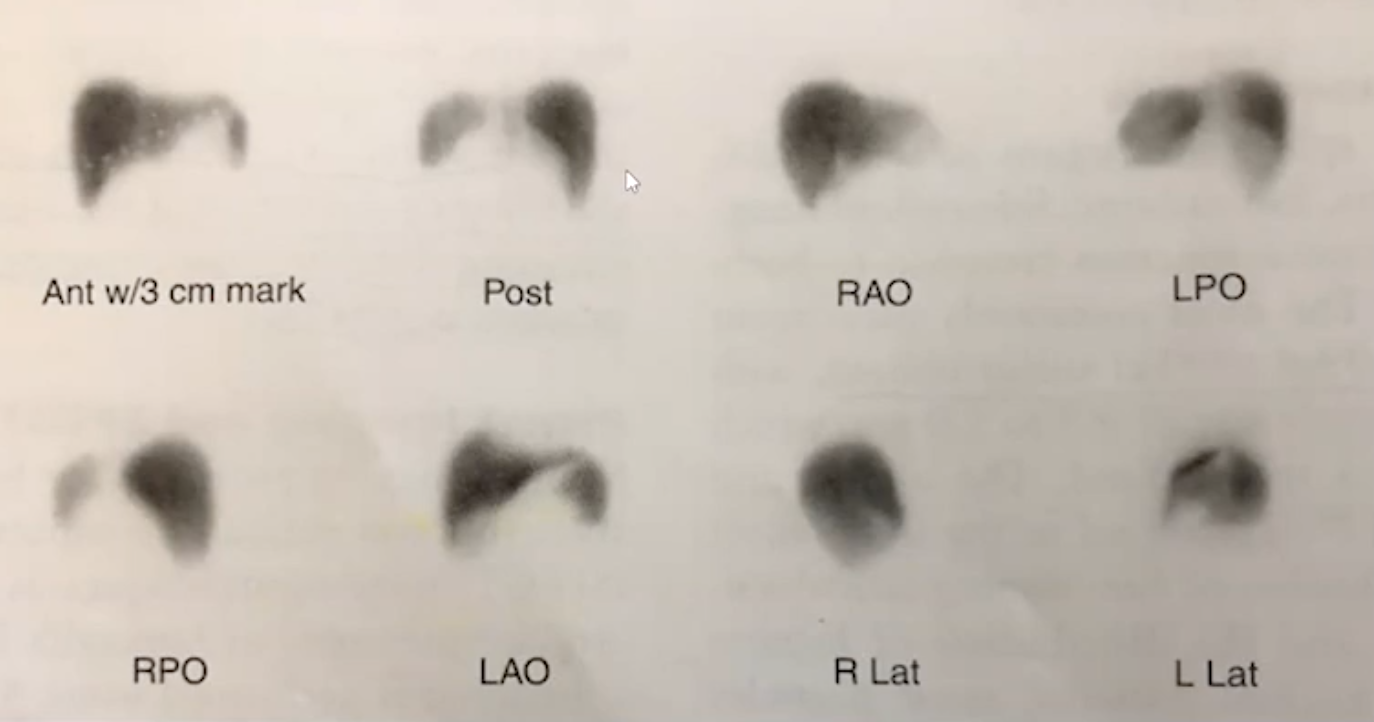
Liver & Spleen Nuc med imaging
Typically evaluated with CT first because better but some instances nuc med can be used
Tc-colloid is tracer
Normal study in pic to right
Indications
Focal nodular hyperplasia
Splenomegaly/splenosis
Colloid shift (cirrhosis)
Hepatic parenchymal lesions, whatever that means
Focal Hepatic Lesions on Tc99-colloid scan
Increased and decreased is relative to background of liver parenchyma
Increased uptake
FNH (top pic)
Regenerative nodule
Decreased uptake
Cyst
Hematoma
Hemangioma
Abscess
Mets, specifically colon cancer mets
Cirrhosis (hepatoma?)
References:
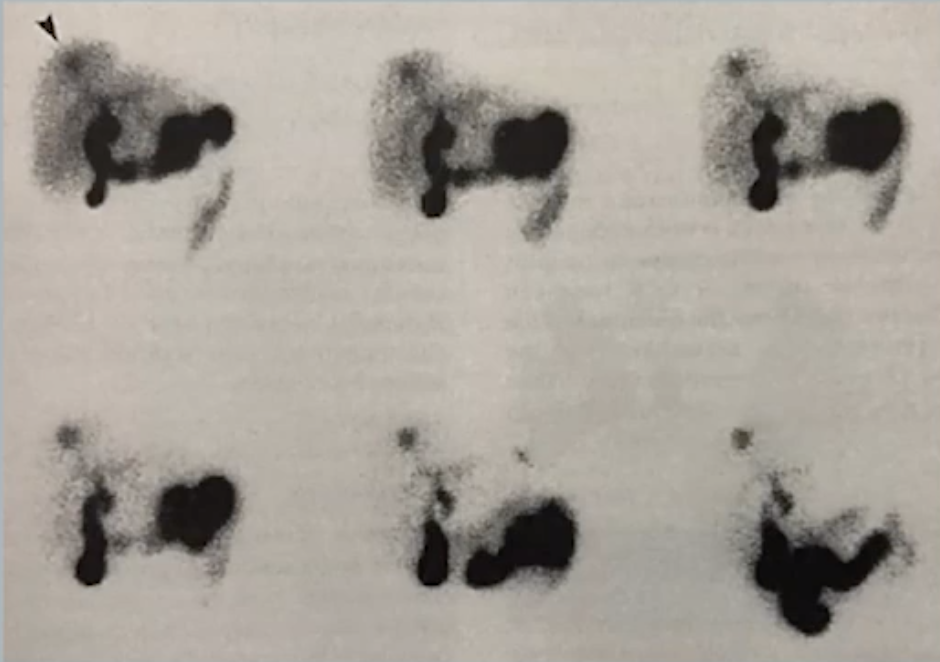
Complete Bile duct obstruction
Basically complete block of flow of the radiotracer into the biliary system so it stays in the liver for the whole exam
No tracer uptake in bile ducts or small intestine
Hot liver sign - strong tracer uptake in liver because it cannot go to bile ducts

Pediatric Hepatobiliary Nuclear Medicine
Liver & Spleen Imaging
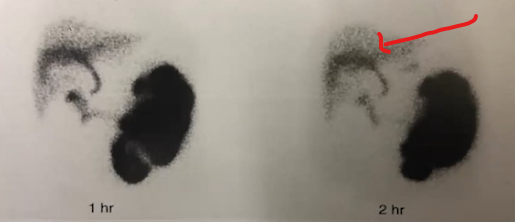
Bile Leak
Seen as increased uptake in dome of liver, GB fossa (after removal I assume, otherwise would be a normal finding), and paracolic gutters
Curvilinear area at bottom is paracolic gutter accumulation
Neonatal Hepatitis
Basically looks like a normal exam with uptake in liver and in small bowel