High Risk Breast Lesions
Breast Malignancy
DCIS (90% with IDC)
Cancer confined to the duct
Multiple filling defects in a duct (note that papilloma will present as a solitary filling defect)
Paget’s
Associated with high grade DCIS
Need to also biopsy the skin - wedge biopsy
Involvement of skin does not upgrade the cancer
Comedo form - more aggressive
Non-comedo form
10% = mass without calcs
MG
Fine linear branching, fine pleomorphic calcs
US
Microlobulated hypoechoic mass
Ductal extension
Normal acoustic transmission
MRI
Non-mass like enhancement
Galactography
Multiple intraductal masses/filling defects on galactogram
Invasive lobular carcinoma (8%)
Seen in older patients
Commonly only seen in one view (usually CC as there is better compression)
Mets to axilla = less common vs ductal carcinoma
Washout less common on MRI vs ductal carcinoma
Prognosis similar to ductal carcinoma
Exception = pleomorphic ILC = very bad
More often bilateral and multifocal vs ductal carcinoma
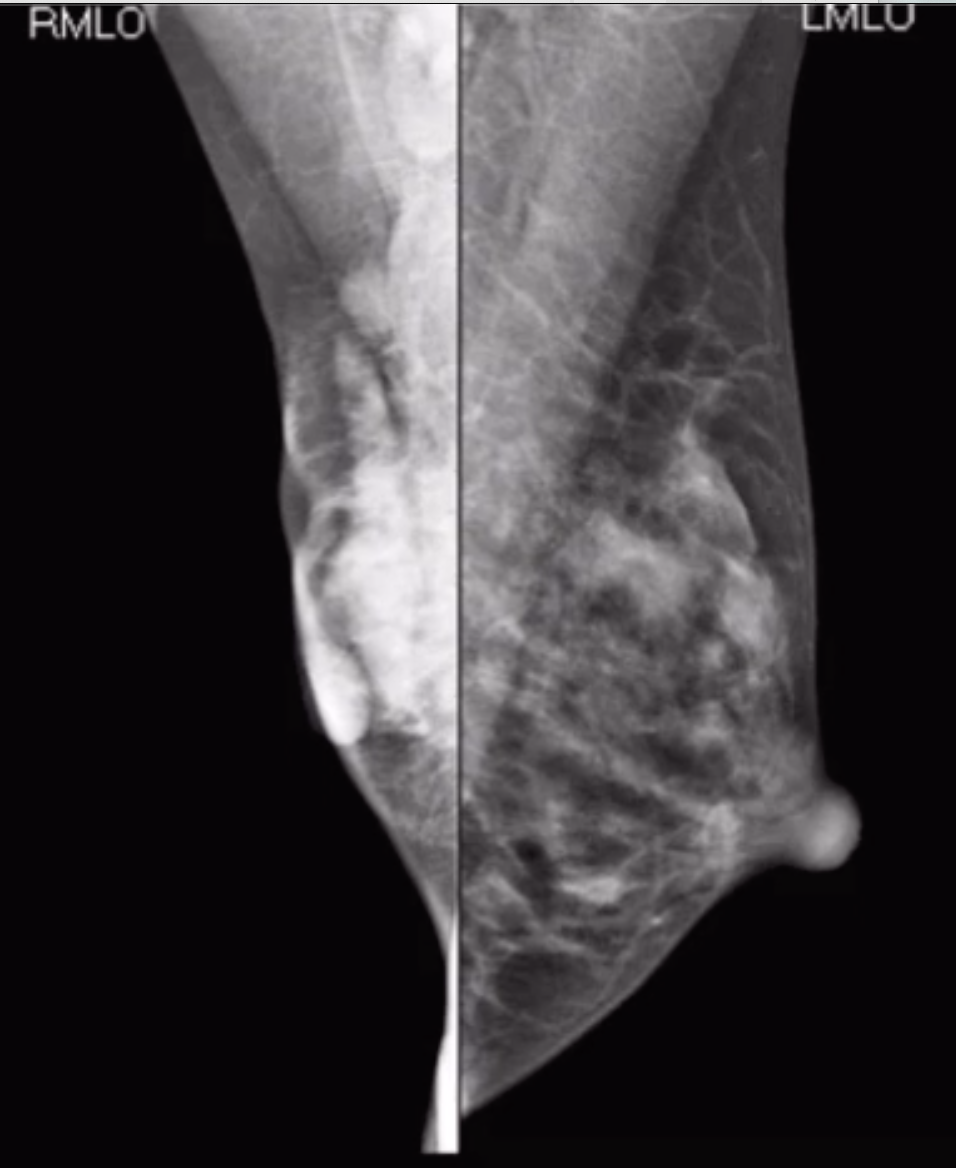
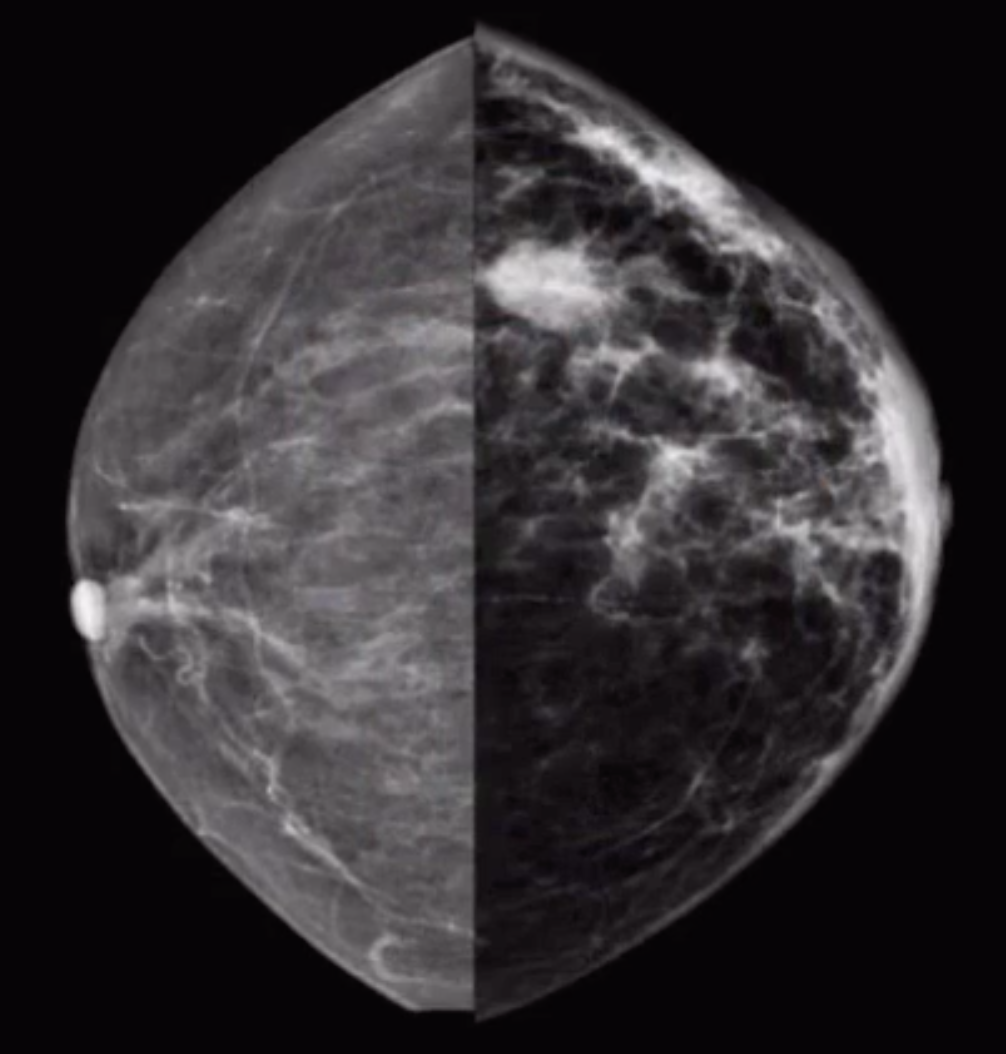
Shrinking breast appearance on mammogram
The affected breast looks asymmetrically small
But may look normal on physical exam
Breast wont compress because its infiltrated and fucked up
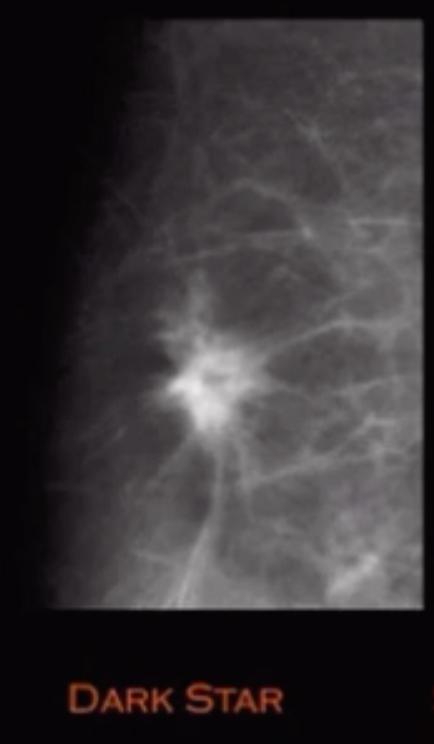
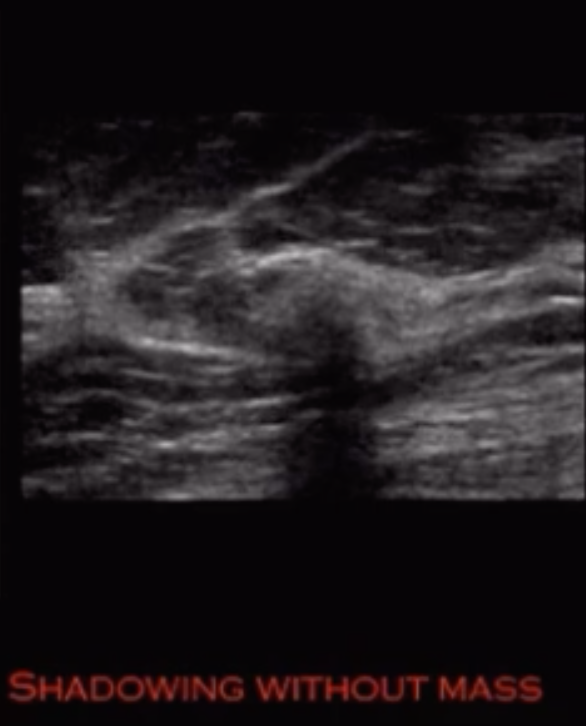
Dark star appearance
Architectural distortion without definitive central mass on MG
Shadowing on US without evidence of definitive mass
Invasion of the overlying skin is not uncommon
Note that you may get this confused with mastitis or inflammatory breast cancer because of the skin involvement but in mastitis or inflammatory breast cancer the breast should really be enlarged and will have lymphadenopathy, in invasive lobular carcinoma the breast is typically asymmetrically smaller and the nodes may be normal or not very impressive
Dark Star DDx
Architectural distortion without definitive mass
Invasive lobular carcinoma
Radial scar
Postsurgical scarring
IDC-NOS subtype
Paget disease of Breast
Carcinoma in situ of the nipple epidermis
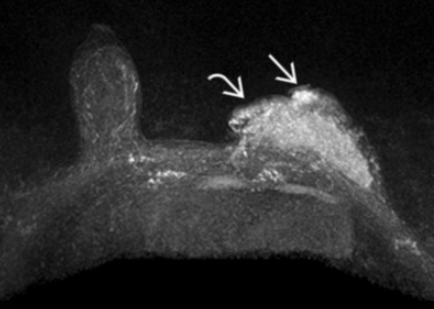
Inflammatory Breast Cancer
Skin thickening
Swollen red breast - think mastitis vs inflam breast cancer
Horrible prognosis
Treat with chemo then surgery
Note the inflammation may improved with Abx but will not RESOLVE
If does not go away completely = cancer
If cannot find a mass and you see this = get skin biopsy
Note skin thickening on left picture
Metastatic Disease to the Breast
Typically round, circumscribed and non-calcified (not typically spiculated)
Typically hematogenous spread from
Melanoma,
Lymphoma
Lung
Others
In males, prostate most common source (> lung)
General
Lesions that are associated with cancer and usually require an excision when they show up on biopsy
Atypical ductal hyperplasia (ADH)
ALD
LCIS
Radial scar
Papilloma
Breast Cancers
Ductal carcinoma in situ (DCIS)
Invasive ductal carcinoma
Invasive lobular carcinoma
Atypical Ductal Hyperpalsia
Basically the precursor to DCIS
By definition, partial involvement of <2 duct sites and measures < 2mm
Most commonly found from biopsy of calcifications
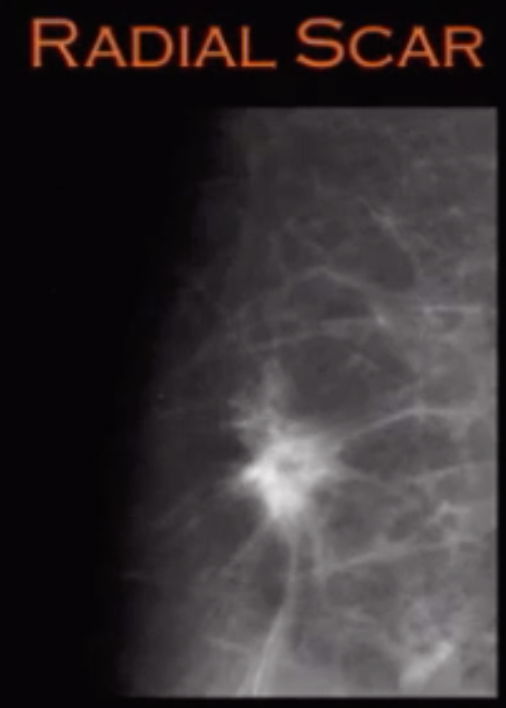
Radial Scar
Dense fibroelastic core with stellate entrapped ducts
Associated with tubular cancer
Dark star appearance
Biopsy recommended
Lymph nodes
Measure area of cortex to hilum in short axis of thickest part
If >2.5-3 mm = abnormal
Non-hilar blood flow is highly suspicious finding
References:
Pleomorphic LCIS
Basically precursor to invasive lobular carcinoma
Cells are more atypical with necrosis and calcifications
Lobular Neoplasia
General term for epithelial atypia of cells lining the lobular portion of the TLDU
Includes
Atypical lobular Hyperplasia (<50% of acini with atypia)
4% chance of becoming malignancy
Classic lobular carcinoma in situ (LCIS) (>50% of acini with atypia)
10% chance of becoming full on malignanct
Difference between this is for path not us
Most commonly found from biopsy of calcifications
Invasive Ductal Carcinoma
Histopath subtypes
Not otherwise specified
Most common
Worse prognosis of those listed here
Mucinous
Rare
High T2 signal 2/2 high mucin content (note ILC is T2 hypo)
Medullary
BRCA association
Seen in younger patients
Bulky lymphadenopathy
Tubular
Spiculated & Small masses
Good prognosis
Has a radial scar
Papillary
Complex cystic & solid
Older patients
Rare to have lymphadenopathy
Basically opposite of medullary
Notice not only the focal mass but how asymmetrically smaller the left breast is compared to the normal right breast
Bilateral Disease
Genetic disease - BRCA
Multicentric disease
Lobular malignancy
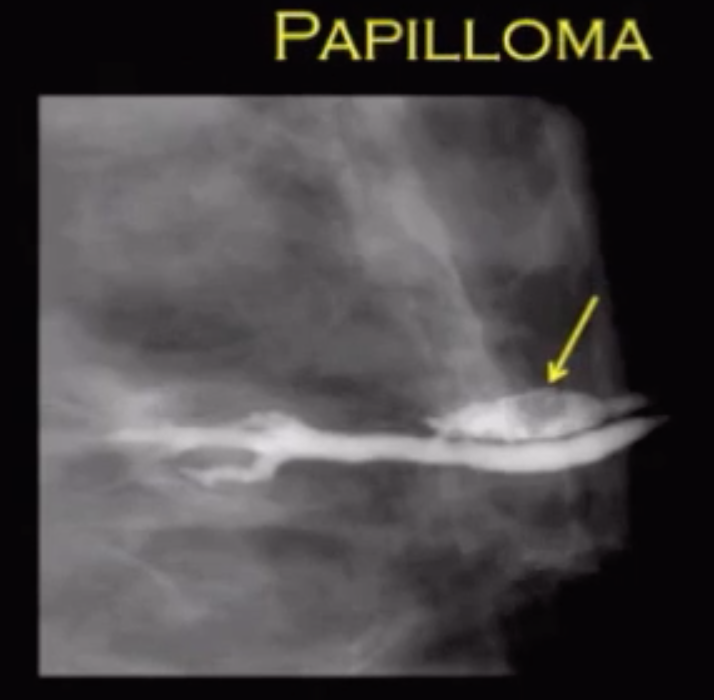
Papilloma
Most common intraductal mass
Most common cause of bloody nipple discharge
Solitary filling defect on galactography
Usually within 1 cm of nipple
Central papillomas more like to be benign than peripheral papillomas