Ovary
General
If a pelvic ass is T2 hypo, it is typically fibrous, the most common of which is a fibroid

O-RADS
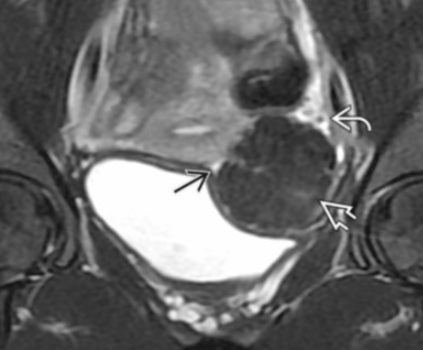
Endometrioma
T2 dark
T1 bright
T1FS-bright
Has internal T1 hyperintensity from old blood
On US
No color on doppler

Dermoid/Teratoma
T2 bright
T1 dark
T1FS dark
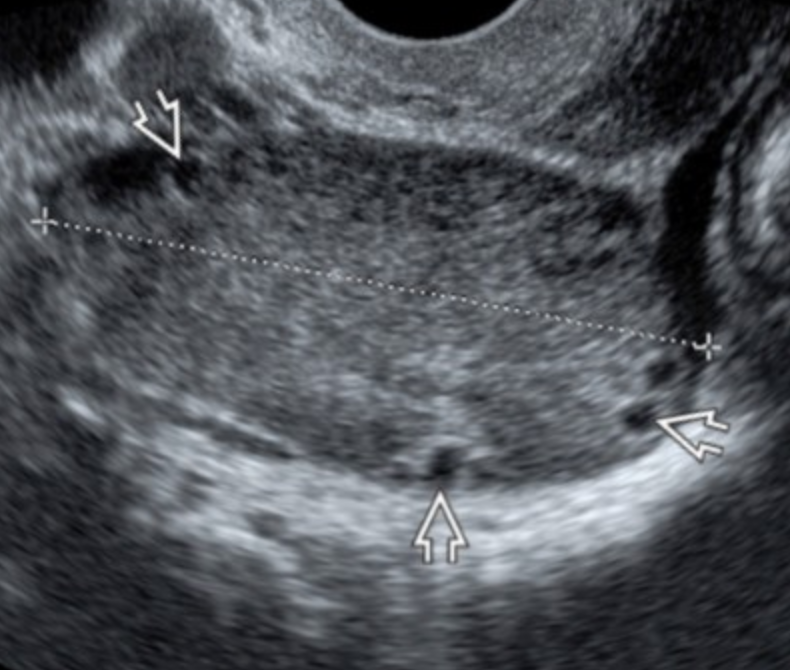
On Us
Tip of the iceberg (bottom)
Broad area of deep hypoechogenicity with iso or hyperechogenic area superficially
Fluid-fluid level
High echogenic substance is in anti-dependent portion and fluid is on bottom
Chemical shift artifact at border of fat and fluid in the frequency encoding direction
Dot-dash sign
Fat ball sign (top)
No color on doppler
Rokitansky nodule = dermoid plug
If enhances, question malignant transformation
Risk of rupture <5%
Risk of torsion = 15%
Risk of malignant transformation = 1%
Peritoneal Inclusion Cyst
Basically cyst in the pelvis
Very commonly arises next to/surrounds the ovary
Seen in women of reproductive age
May have septation
Not your typically well circumscribed cyst, its basically if there is inflammation and scarring or whatever and it walls off a fluid collection that is sterile (not an abscess)
Looks like a non circular cyst around ovary usually
Serous Cystadenoma
Unilocular
Thin walled
Simple fluid
On US have papillary projections
Basically what you think of when you think of a simple cyst
Note - may get bigger and likely persists over time, a follicular cyst will go away after 2-3 menstrual cycles
Granulosa Cell tumor
Solid and Cystic mass
Unilateral
Most common ovarian neoplasm
Typically post-menopausal women
Estrogen secreting tumor
Look for endometrial hyperplasia/endometrial thickening
Brenner Tumor
Mixed solid and cystic mass
Benign
Low T2 signal secondary to high fibrous content
References:
Cystic Adnexal Masses
Hemorrhagic Cyst
T2 bright
T1 dark
T1-FS bright
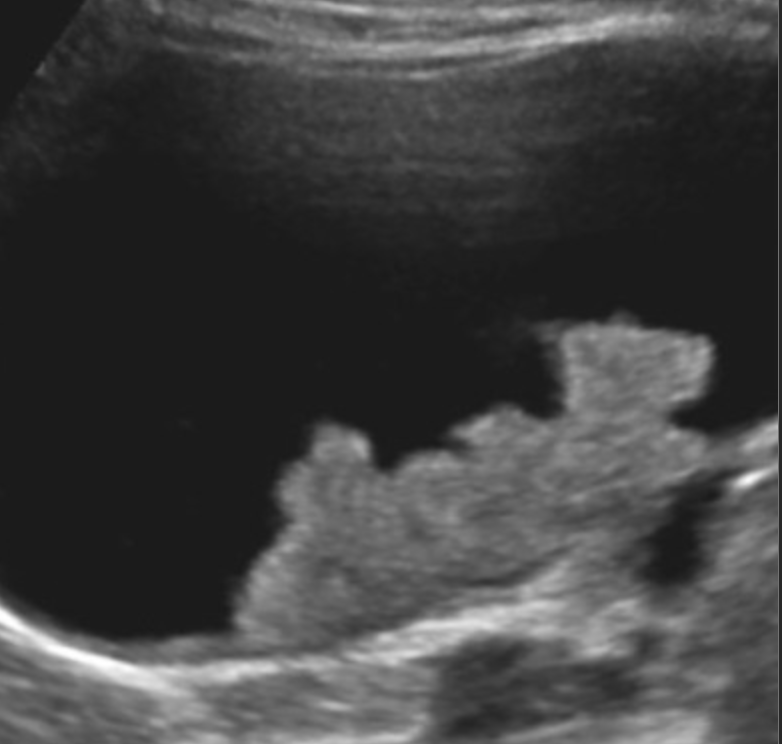
On US
Fluid-fluid level
High echogenic substance is in dependent portion and fluid is on top
Fibrin threads
Linear increased echogenic lines
Has a cobweb appearance - US below
Retractable clot (left thick arrow in US below)
No color on doppler
Mature Teratoma
Large clusters of fat
Usually more well defined
Large tooth-like clusters of calcifications
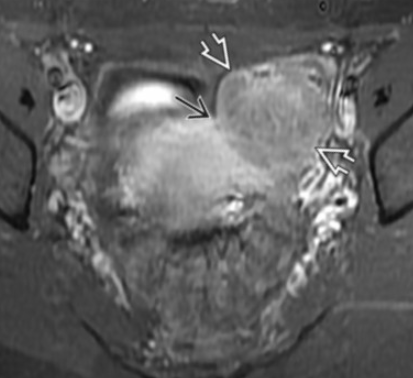
Ovarian Fibroma/Fibrothecoma
T1 hypo
T2 very hypo
Mild diffuse enhancement
Note: endometriomas will have internal T1 hyper signal from old blood
Struma Ovari
Multiloculated cystic lesion with strongly enhancing solid nodule
Simple Cyst
T2 bright
T1 dark
T1-FS dark
On Us
No color on doppler
Hydatid Cysts of Morgagni (Paratubal cyst)
Simple cyst near end of the fallopian tube in close proximity to the fimbriae
Asymptomatic
Honestly just looks like a random pelvic cyst, just not next to the ovary itself I guess, closer to the tube
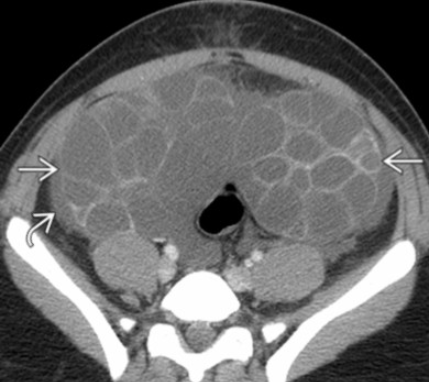
Mucinous Cystadenoma
Multiloculated
Thin walled with septa
Simple and/or complex fluid
Non Cystic Ovarian Masses
Dysgerminoma
Typically a purely solid mass
May have hemorrhage and necrosis making it look heterogenous
Lymphoma
Burkitt lymphoma
Unilateral or bilateral mixed solid and cystic lesions
Look for concurrent ileal disease
Immature Teratoma
Scattered small areas of fat interspersed between soft tissue mass
Typically larger and less defined vs mature teratoma
Irregular and amorphic calcifications

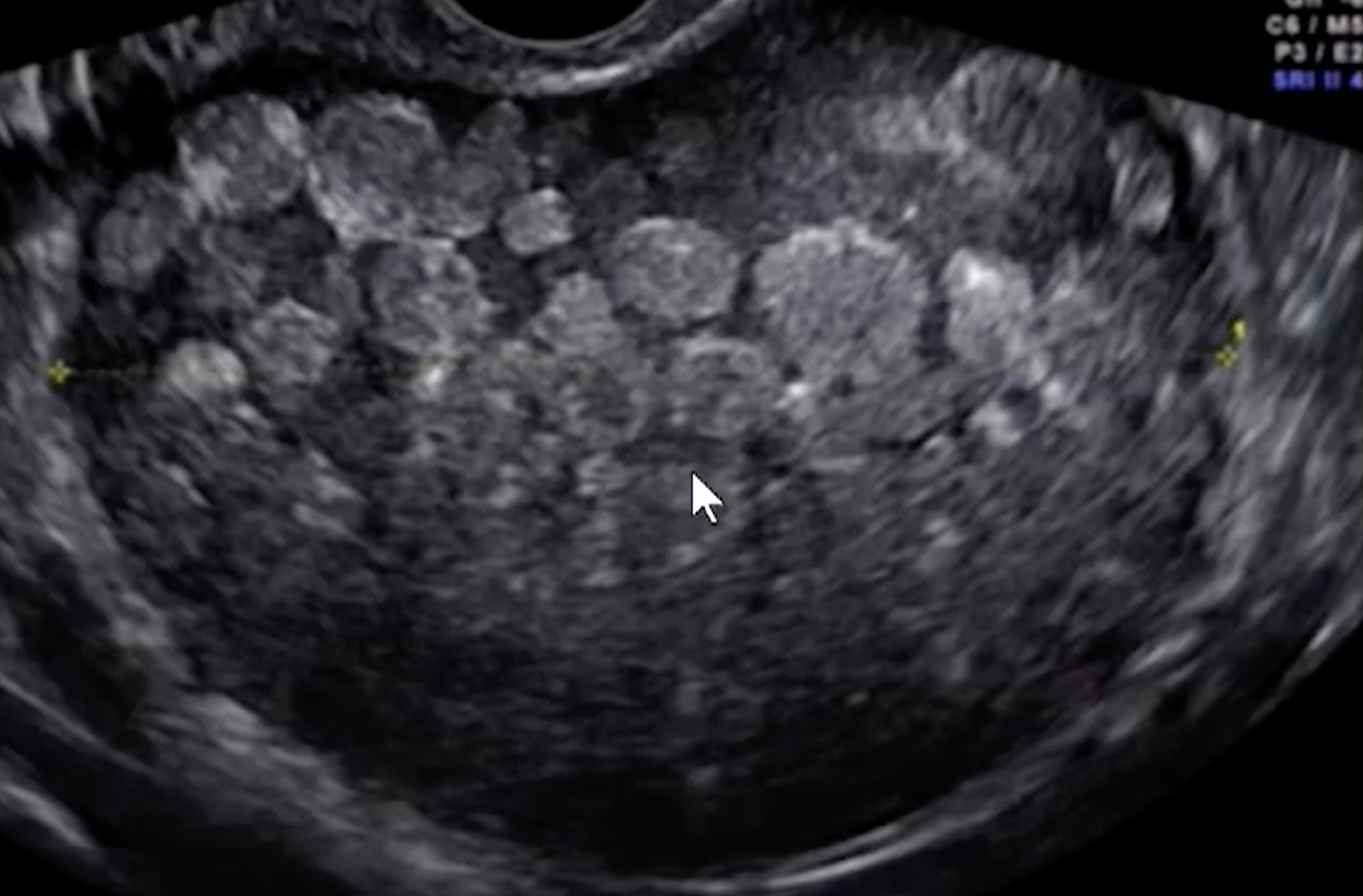
Hyperreactio Luteinalis
Very similar to ovarian hyperstimulation syndrome
Bilateral enlarged multicystic ovaries
WILL HAVE ELEVATD HCG
Associated with molar pregnancy
Benign and will resolve with delivery of normal pregnancy or removal of the molar pregnancy in cases of molar pregnancy
Meigs Syndrome
Triad of
Ascites
Pleural Effusion
Benign ovarian mass
8-& are fibromas (fibrothecoma)
Syndromes
Ovarian hyperstimulation syndrome
Range of mild to severe
Severe will have ascites and hemodynamic instability, renal failure, ARDS
Bilateral ovary enlargement
Associated with IVF
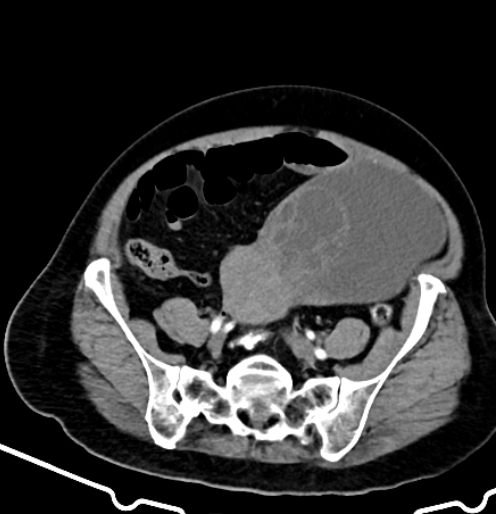
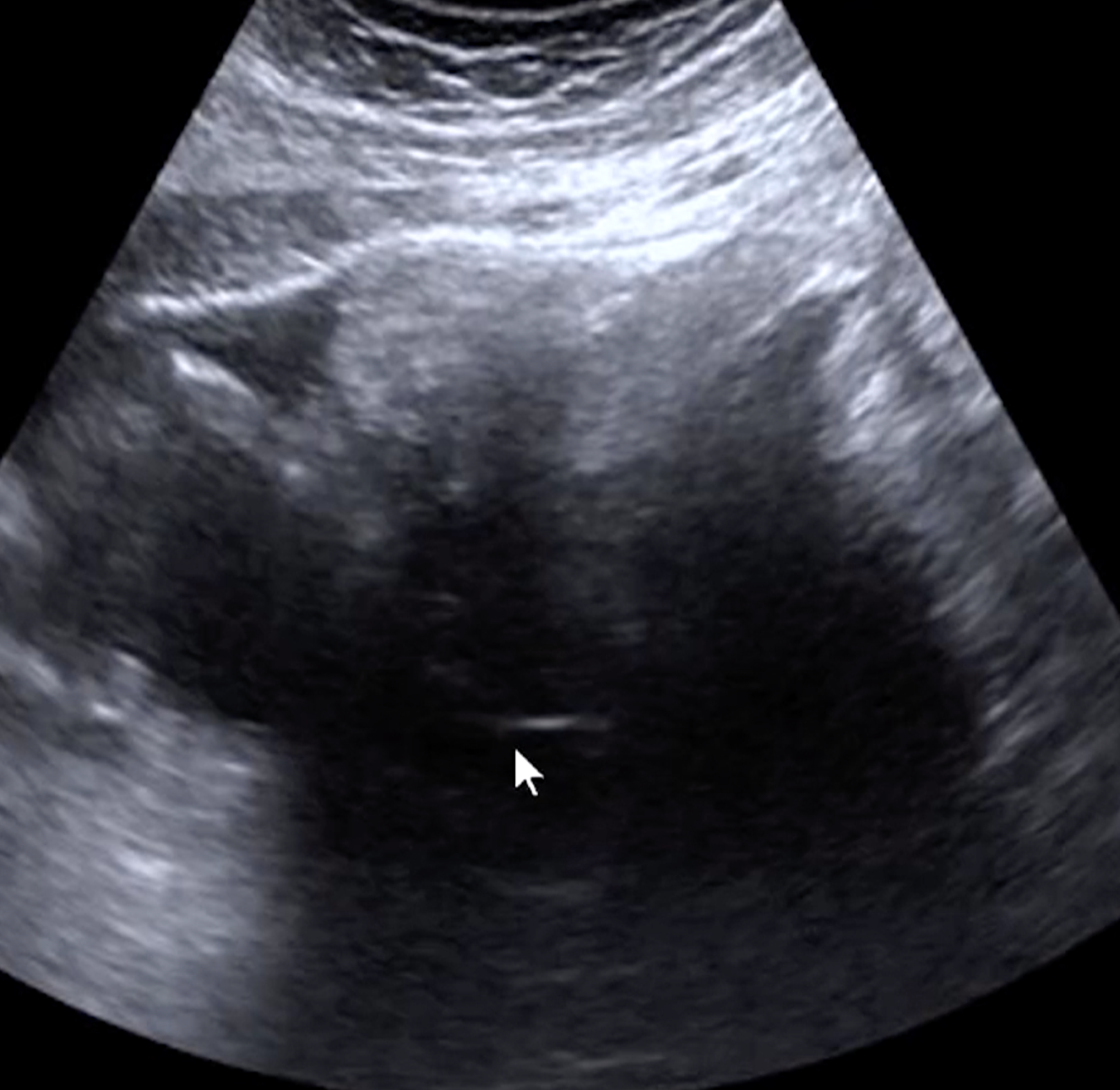
Massive Ovarian Edema
Unilateral
Makes it look like the ovary is solid without focal mass
Peripheralization of the follicles with normal blood flow
Enlarged ovary
Ovarian fibromatosis basically presents the same but due to fibrous tissue rather than edema