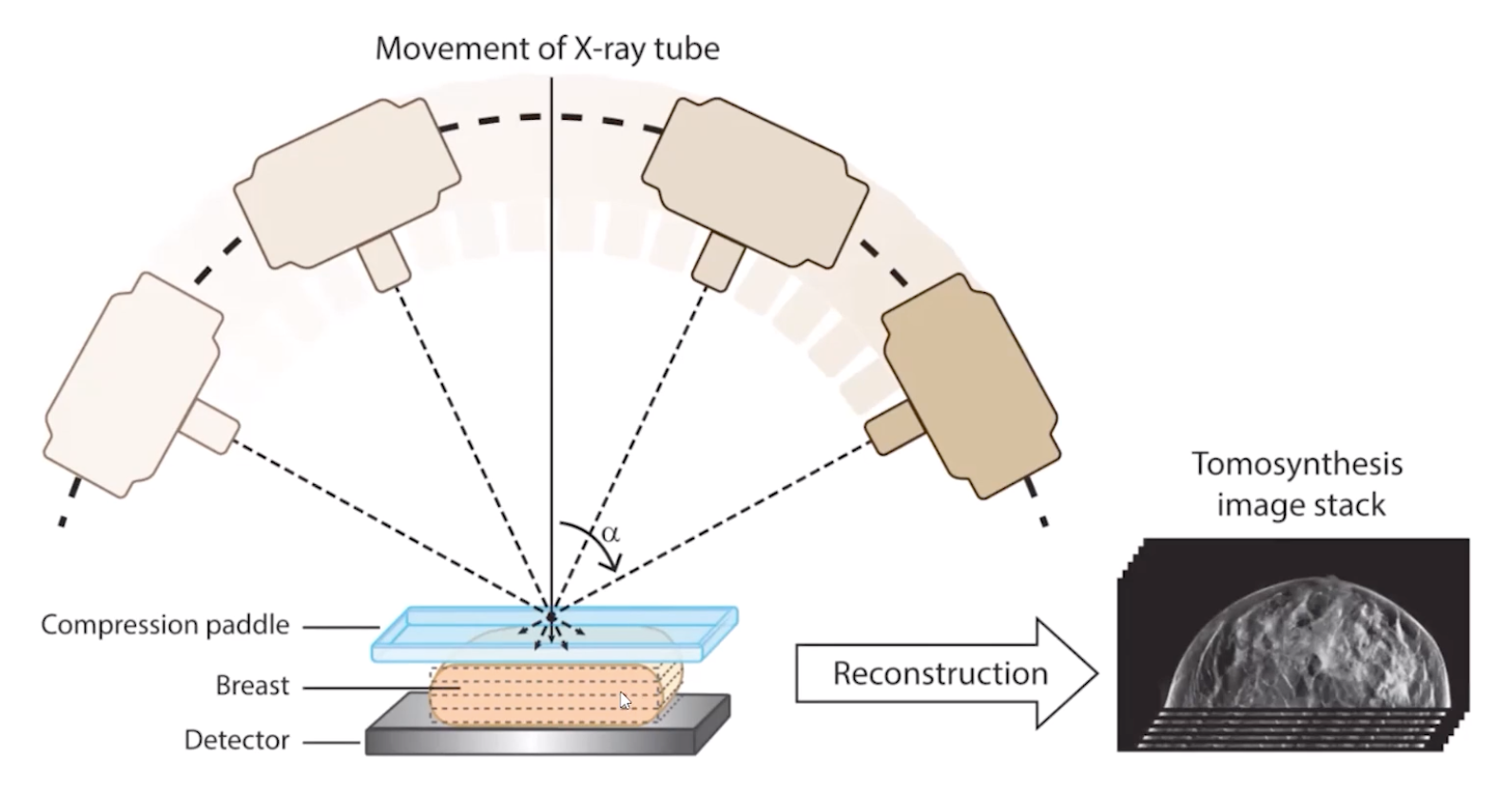
Tomosynthesis
Multiple low dose exposures obtained in an arc and then fused together in 1 mm slices
3 images actually used
Raw images of the actual exposure
The fused raw images in 1 mm slices
Traditional Digital Mammogram or Synthesized Mammogram (these are basically post-processing images it seems)
CAD = Computer Aided Detection - 2 types
CADe = D = Detection = Identifies Abnormalities
CADx = D = Diagnosis = Classifies Abnormalities
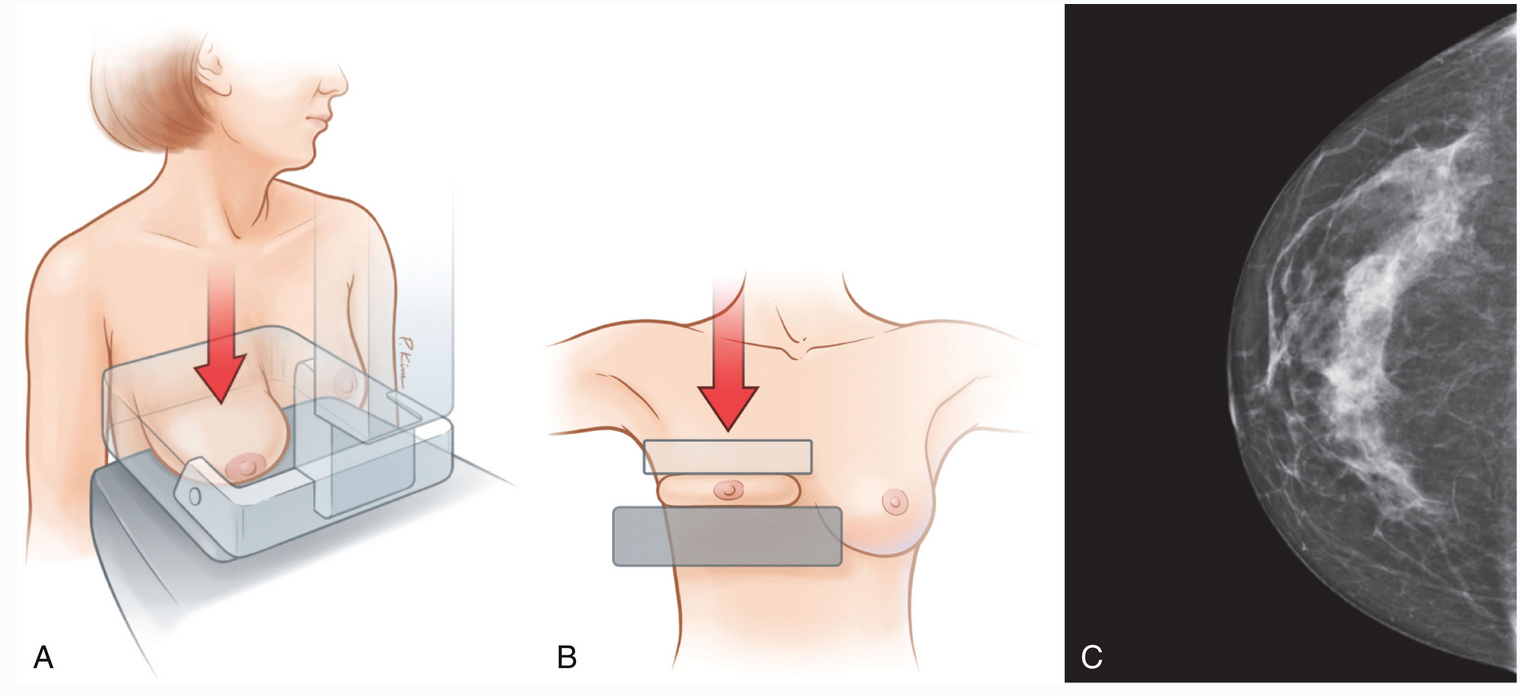
Compression of breast during mammogram
Decreased radiation dose
Decreases blur by reducing exposure time and less time for pt motion
Reduces scatter = better image contrast
Views
Views
View describes the direction of the XR beam
Typical default included views include MLO and CC
Other possible views include
Cleavage view
Exaggerated medial and lateral CC views
Others
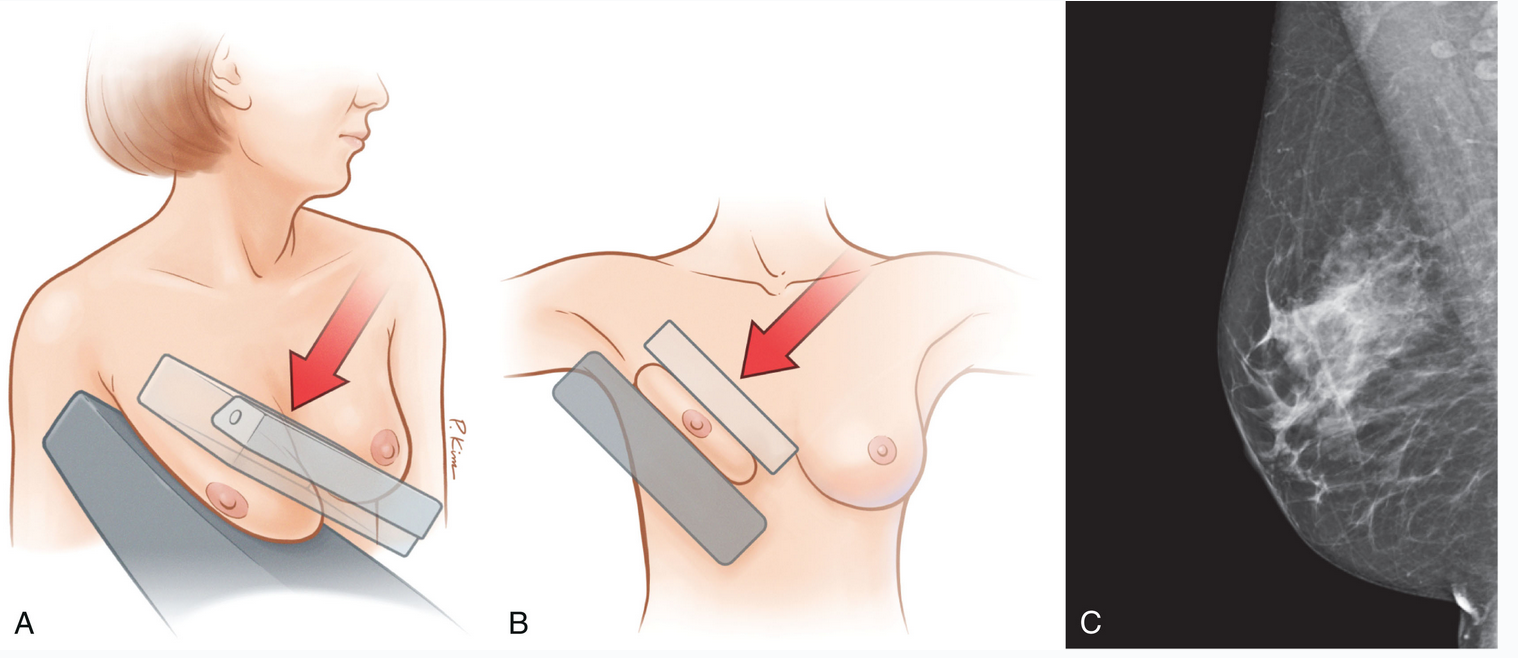
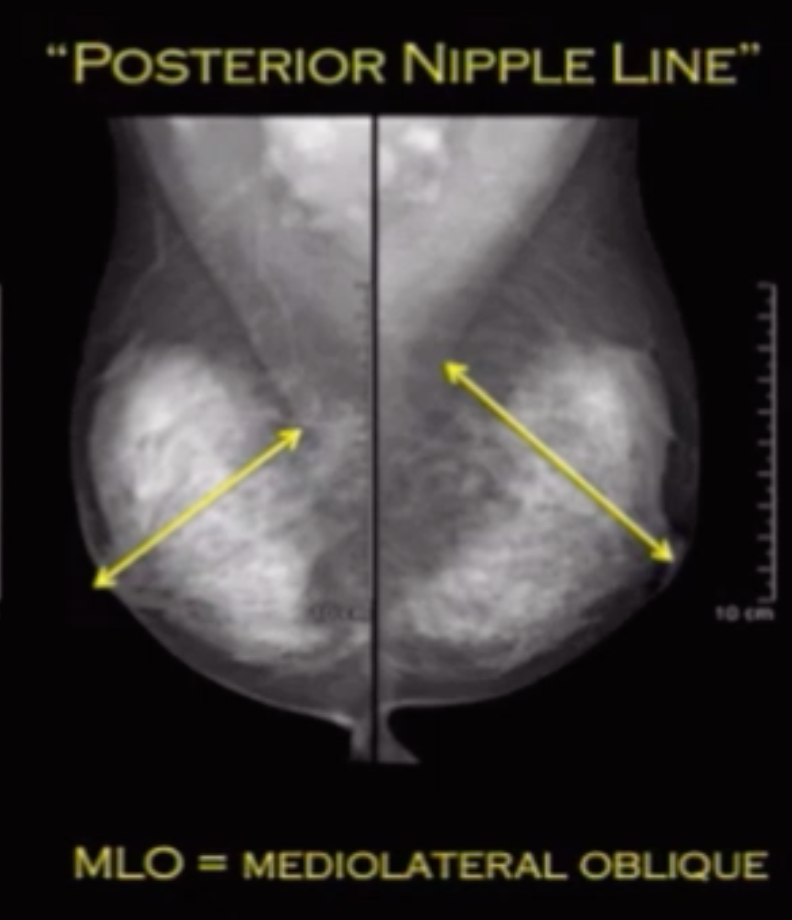
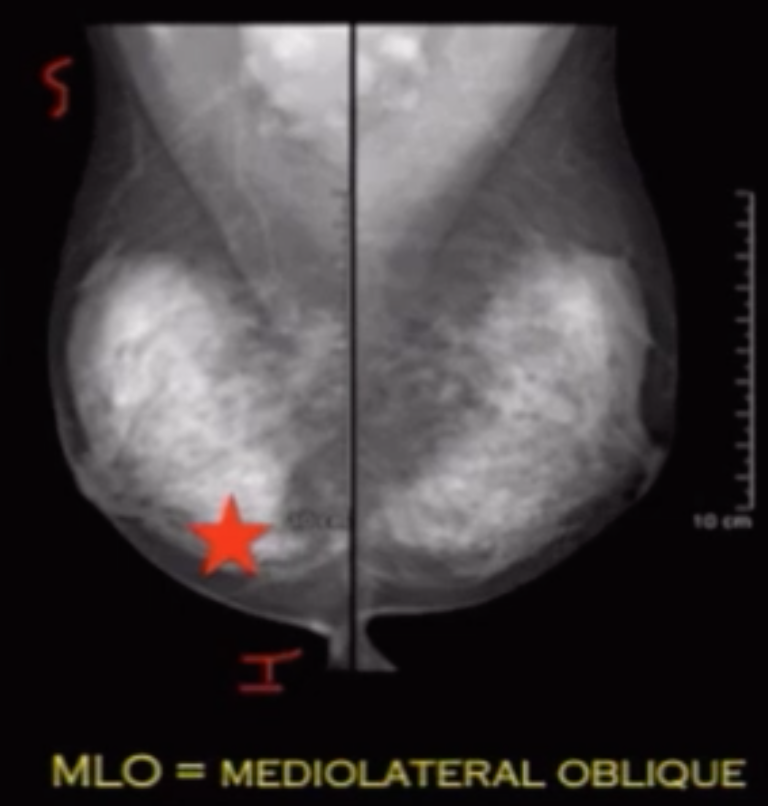
Mediolateral Oblique (MLO)
Beam travels from superior-medial to inferior-lateral
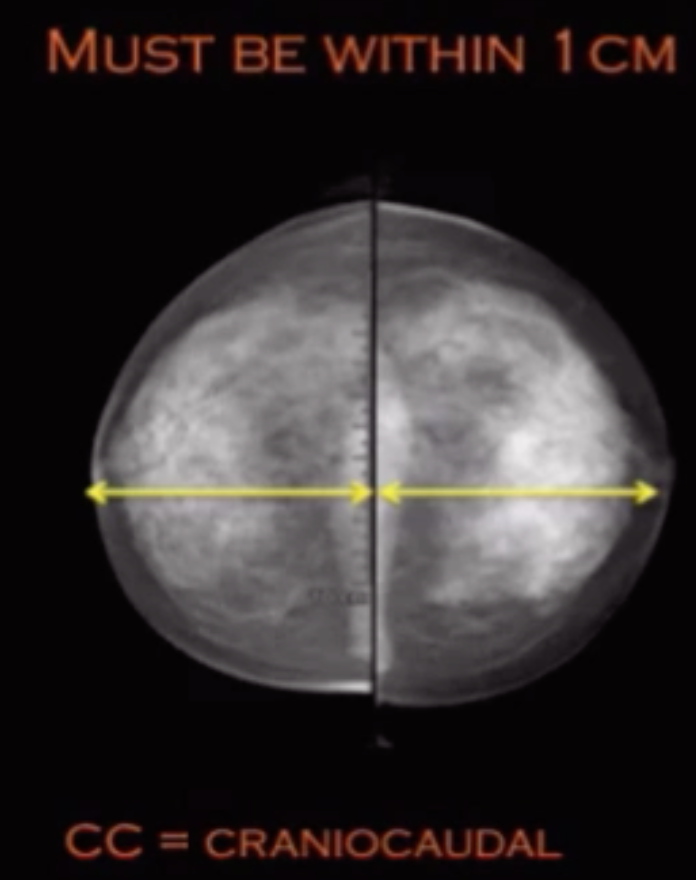
Draw line from nipple to border of pectus muscle = posterior muscle line
This line needs to be within 1 cm of a line drawn from nipple posteriorly on the CC view
Terminology & Basics
Multifocal = 2+ lesions in same quadrant or within 5cm of each other
Multicentric = 2+ lesions in different quadrants or greater than 5 cm of each other
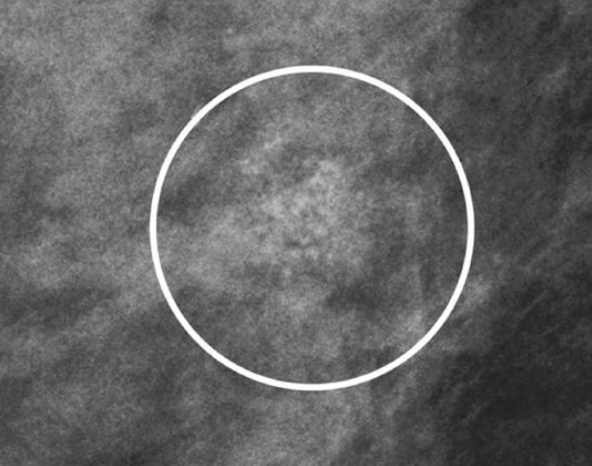
Asymmetry
Regular Asymmetry = density seen only in one view that may or may not be a mass
Global Asymmetry = basically more breast tissue on one side relative to the other
“More” means at least one quadrants amount of asymmetry
If initial visit needs to be called back for another look to establish a baseline
Focal Asymmetry = lesion seen in 2 views but not further characterized by compression or mag views
Developing asymmetry = new lesion is there that wasn’t seen before basically
Plain Film Mammogram
Lesions are described by shape, density and margin
Shape
Oval
Round
Irregular
Density (relative to background breast parenchyma, not fat)
Low
Equal
High
Fat (Classic ddx)
Lymph node
Hamartoma
Galactocele (if lactating)
Oil cyst
Fat encrosis
Lipoma
Margin
Circumscribed
Obscured
Microlobulated
Indistinct
Spiculated
General Tips
Danger Zones
Medial Zone of the breast
Should only contain fat, if you see something in medial zone should raise concern for bad shit
Exception is the sternalis muscle which is normal on the CC view and should not really be seen on MLO
Retroglandular fat
Fat between the normal glandular tissue anteriorly and the chest wall posteriorly
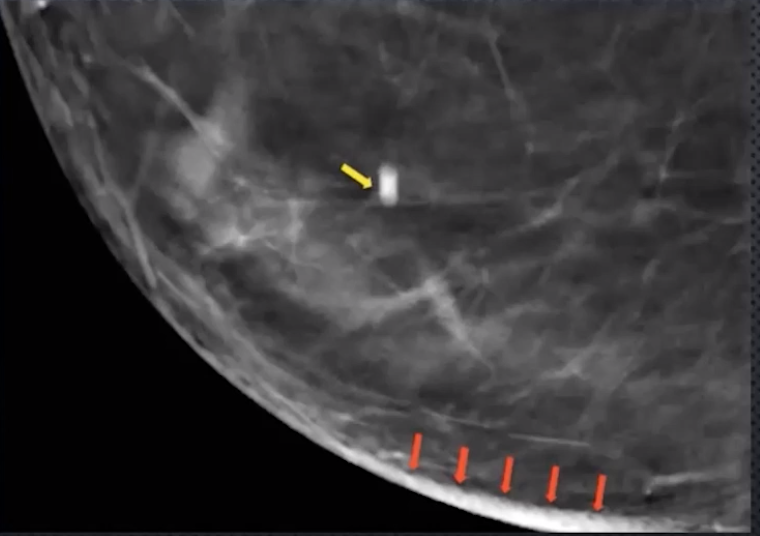
Blurring/Ripple Artifact
Caused by limited # of acquired projections
Occurs perpendicular to XR tube sweep direction
Look for falsely thickened appearance of skin
Coarse calcs and biopsy clips will have elongated slinky appearance
Fix via post image processing
Motion
Idk man
Makes seeing calcs much harder
Look for linear line of calcs, its really just one that is like dragged out
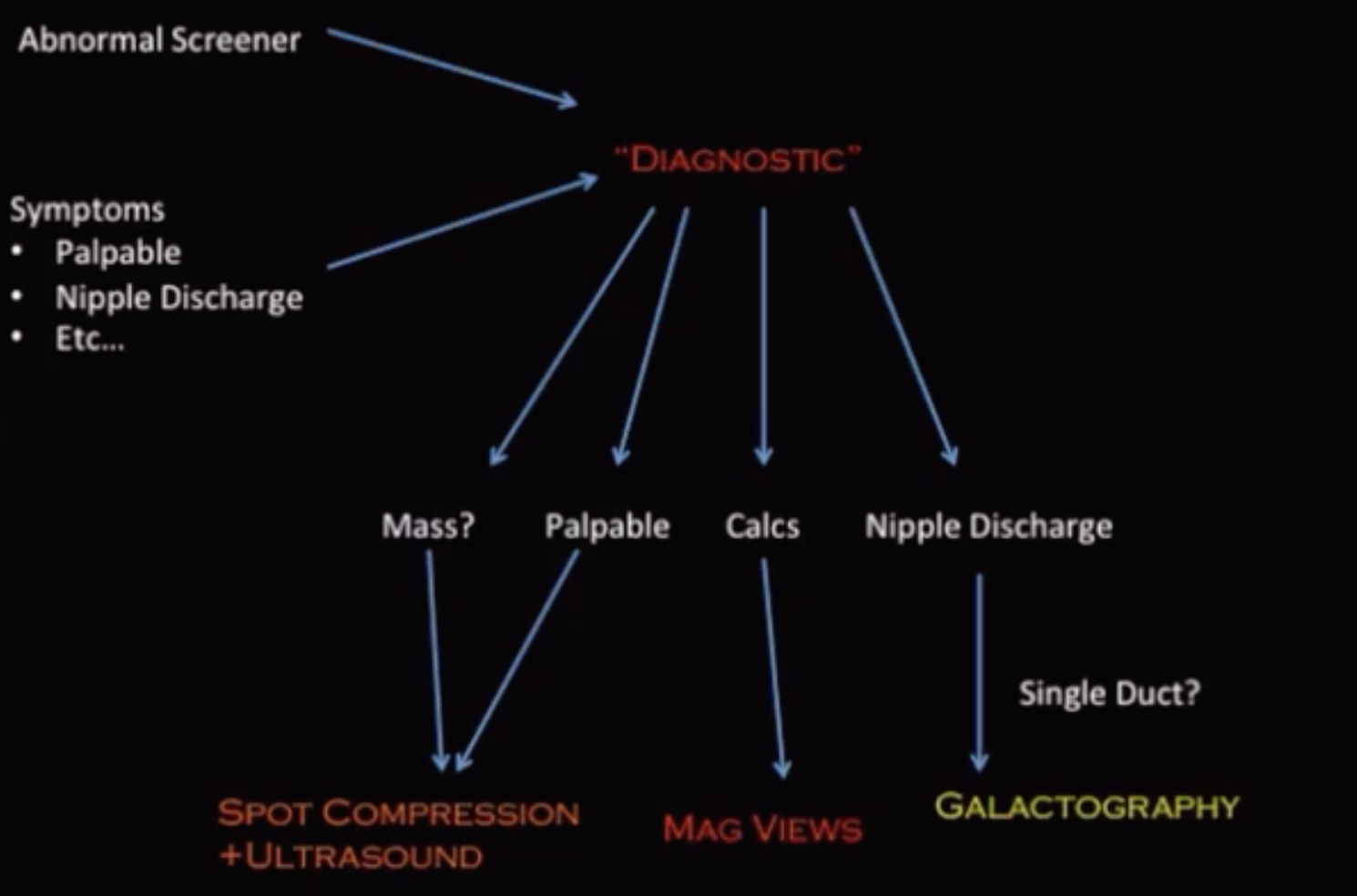
Special workflow in Pregnant and Lactating women
If pregnant or lactating and feel a lump
Want to start with an US and if you see something then get a mammogram
If pregnant or lactating and need their routine screening mammogram
Wait 2-3 months after breastfeeding has been completed to perform mammogram
BR-3
Things that can get a BR-3 on baseline exam
Grouped or clustered round calcifications
Asymmetry with interdispersed fat
Fibroadenoma appearing lesion
US Descriptors
Typically bs like echogenicity, shadowing
Mammo-specific = orientation
Orientation
Parallel (to chest wall) =typically more benign
Anti-parallel (to chest wall) = bad
TOMO Artifacts
Workflow
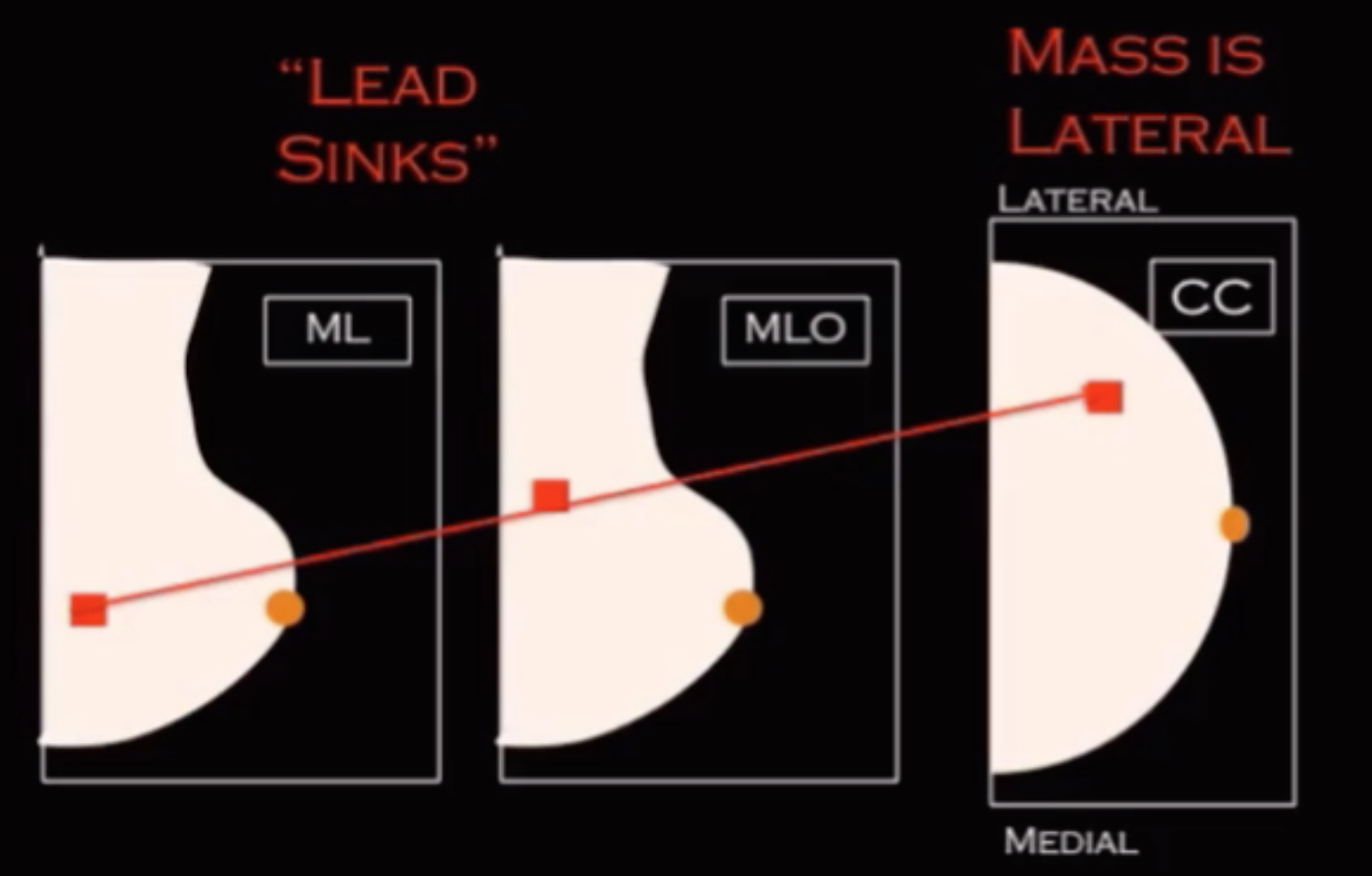
Lesion only seen on MLO?
Get a true lateral
You will evaluate whether the lesion is superior or inferior relative to the loction it was seen on the MLO
Use the nipple as your landmark on each
If lesion is inferior on true lateral relative to the MLO then it is located in the lateral aspect of the breast (re-look at lateral on CC to see if you see anything)
Lead sinks = L = lateral
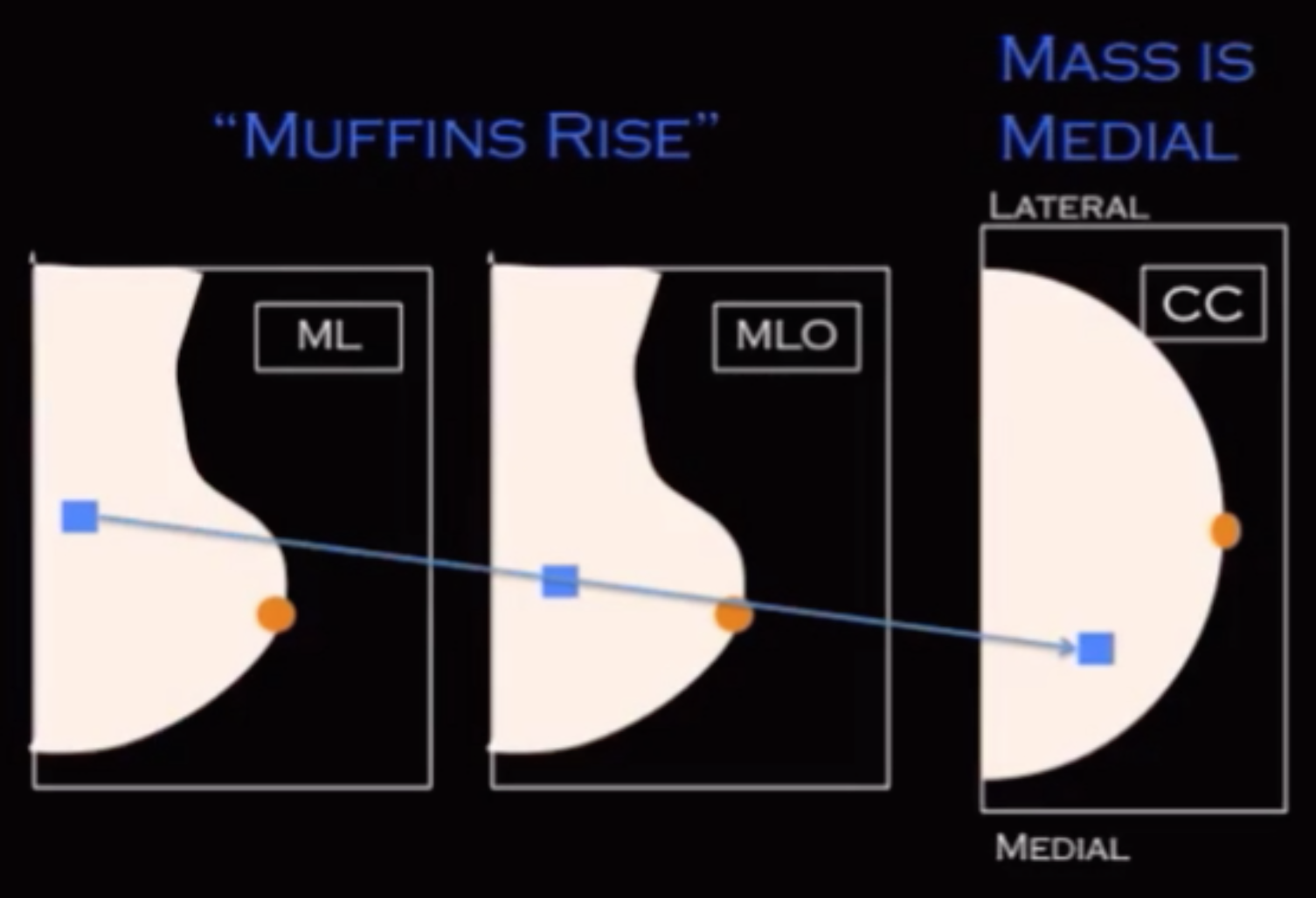
If lesion is seen superior on lateral relative to MLO then the lesion is located in the medial aspect of the breast
Muffins rise = M = medial
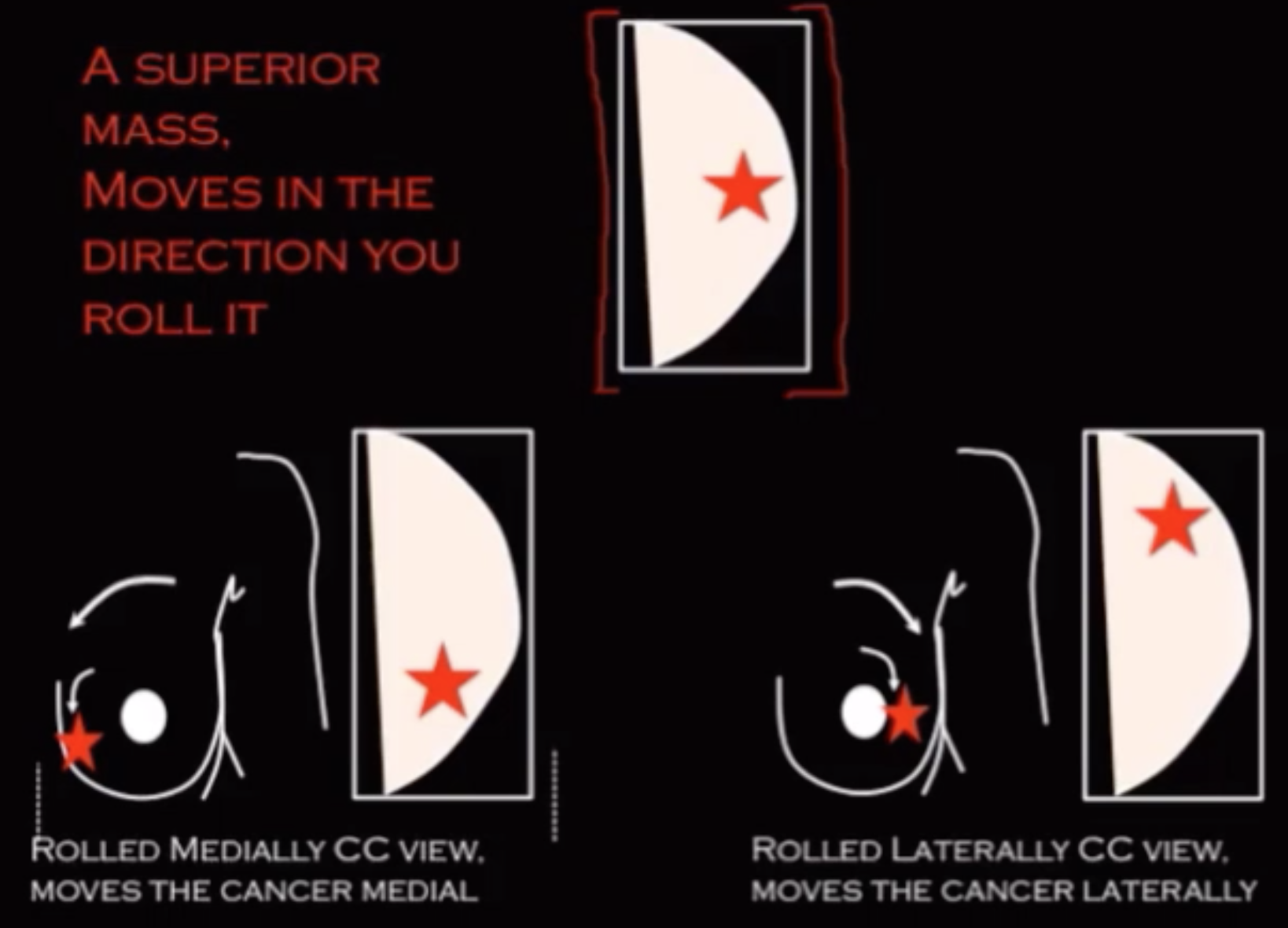
Mass only seen on CC?
Basically means you see how deep the mass is but not if it is in the superior or inferior breast
Get a rolled CC view
Mass is in superior compartment
Mass will move the same way you move the breast
Roll breast medially, mass will move medially
Roll breast laterally, mass will move laterally
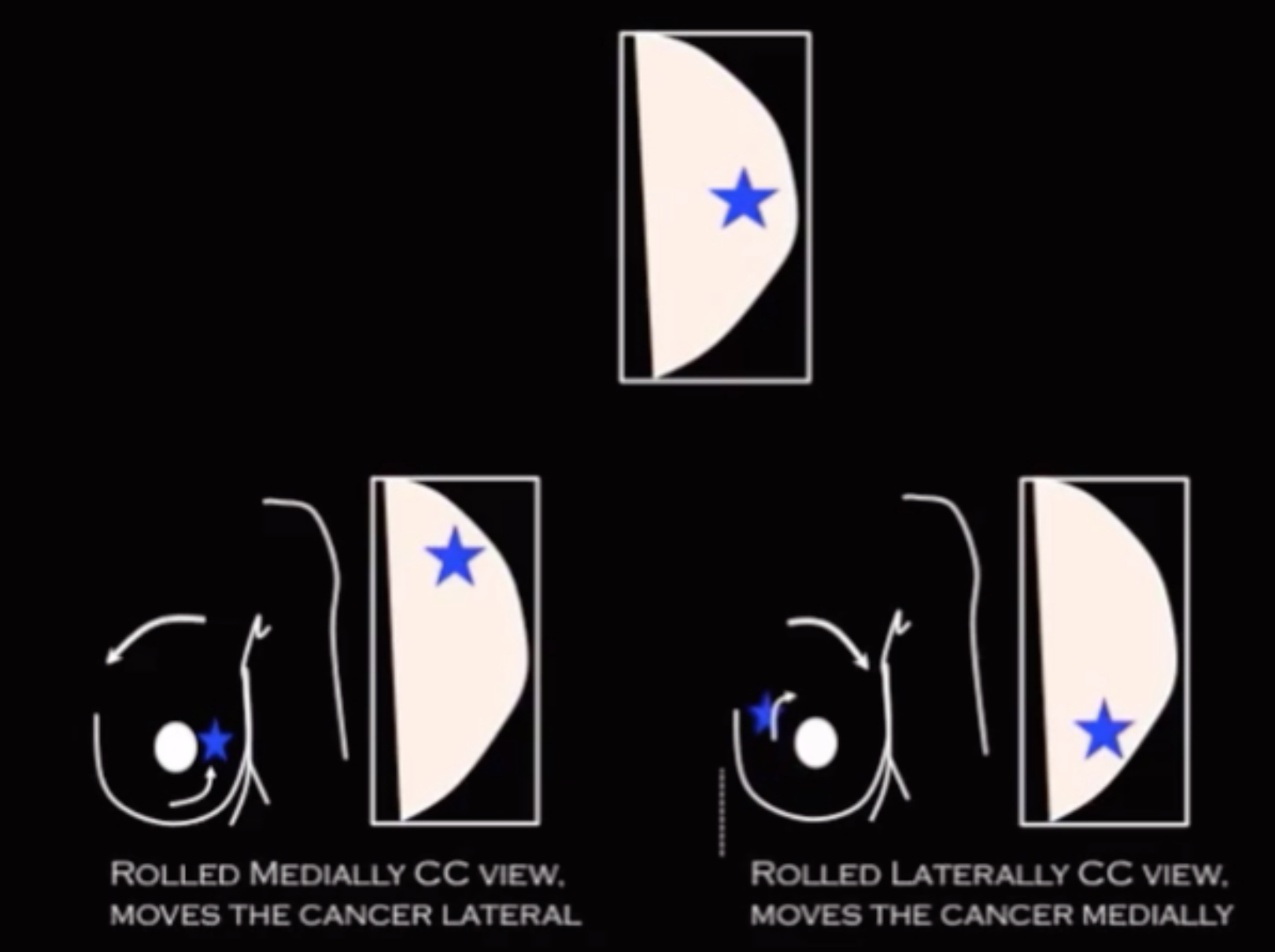
Mass in inferior compartment
Mass will move the opposite way you move the breast
Roll breast medially, mass will move laterally
Roll breast laterally, mass will move medially
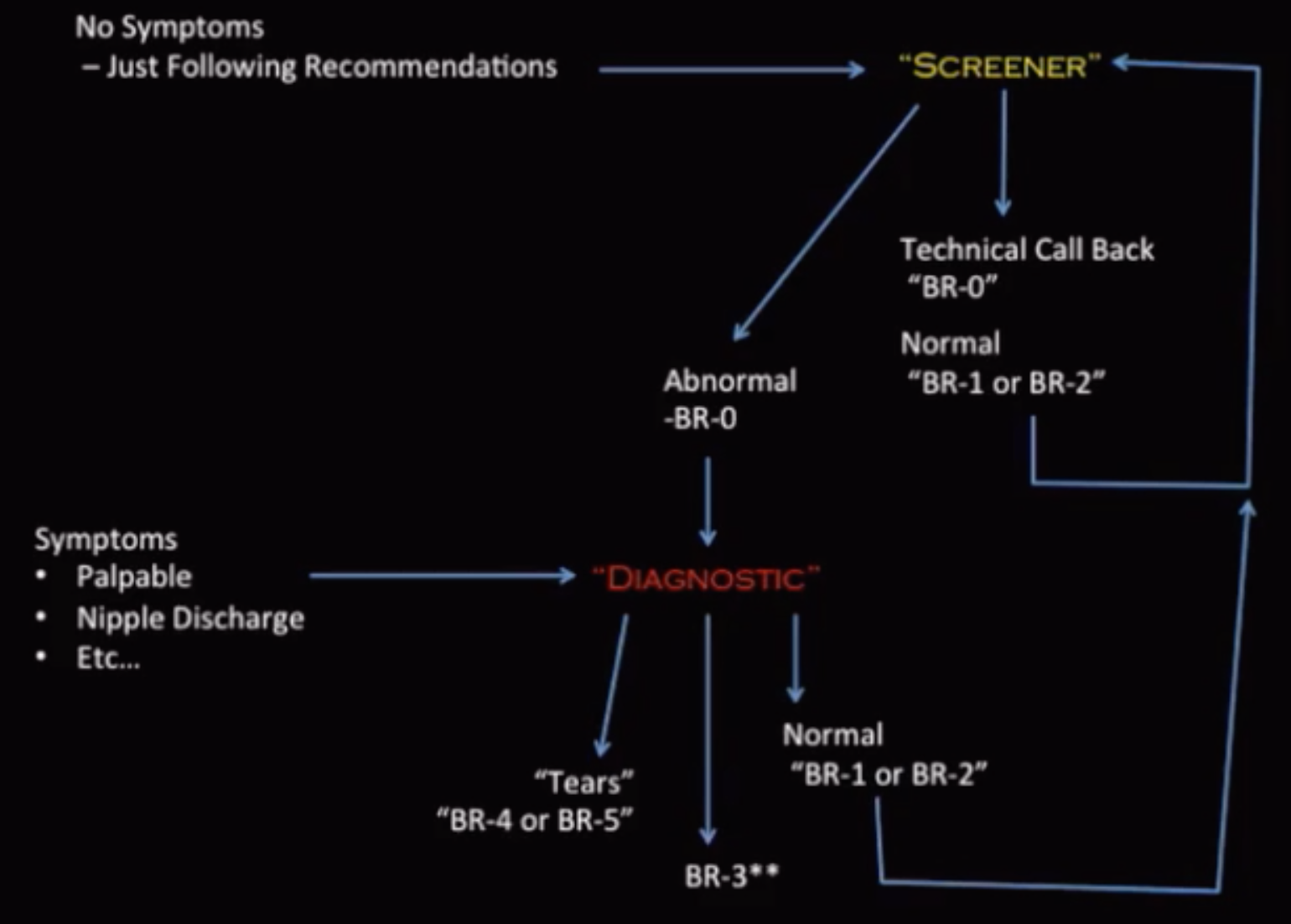
BI-RADS
BI-RADS Classification
BI-RADS 0 = Incomplete assessment
BI-RADS 1 = Negative
BI-RADS 2 = Benign finding
To call BI-RADS 2 on a baseline need at least 3 masses with at least 1 in each breast
BI-RADS 3 = Probably benign
Round calcs or lesions on baseline exam
2% chance of malignancy
BI-RADS 4 = Suspicious (2-95% chance of malignancy)
If you made it a BI-RADS 4 lesion, you have to biopsy it, if the biopsy comes back as benign you can leave it alone
BI-RADS 5 = Highly suspicious mass (>95% chance of malignancy)
If you make it BI-RADS 5 something, you have to biopsy it, if the biopsy comes back as benign then you HAVE to have a surgical excision of the lesion
BI-RADS 6 = path proven
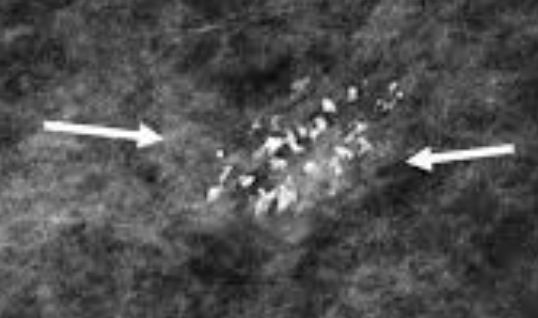
Calcifications
Ductal
Dash-dot-dash = no good
Concerning fro DCIS

Amorphous Calcifications
Basically multiple calcs but can’t actually make out how many, just a bunch
Hazy and indistinct
DDx
Fibrocystic change = most likely
Sclerosing adenosis
Columnar cell change
DCIS - low grade
Fine Linear Branching
Very bad
DDx
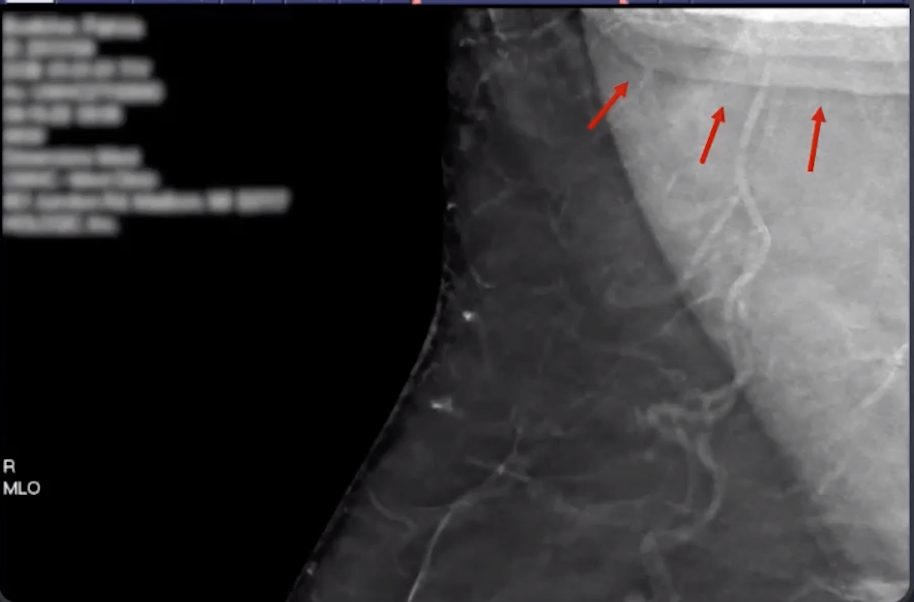
Atypical vascular or secretory calcs
DCIS
Coarse Heterogeneous Calcifications
Multiple calcs, and you can actually count how many
Borders are not sharp (would not prick you if you held them in your hand)
DDx
Fibroadenoma
Papilloma
Fibrocystic change
DCIS - low/intermediate grade
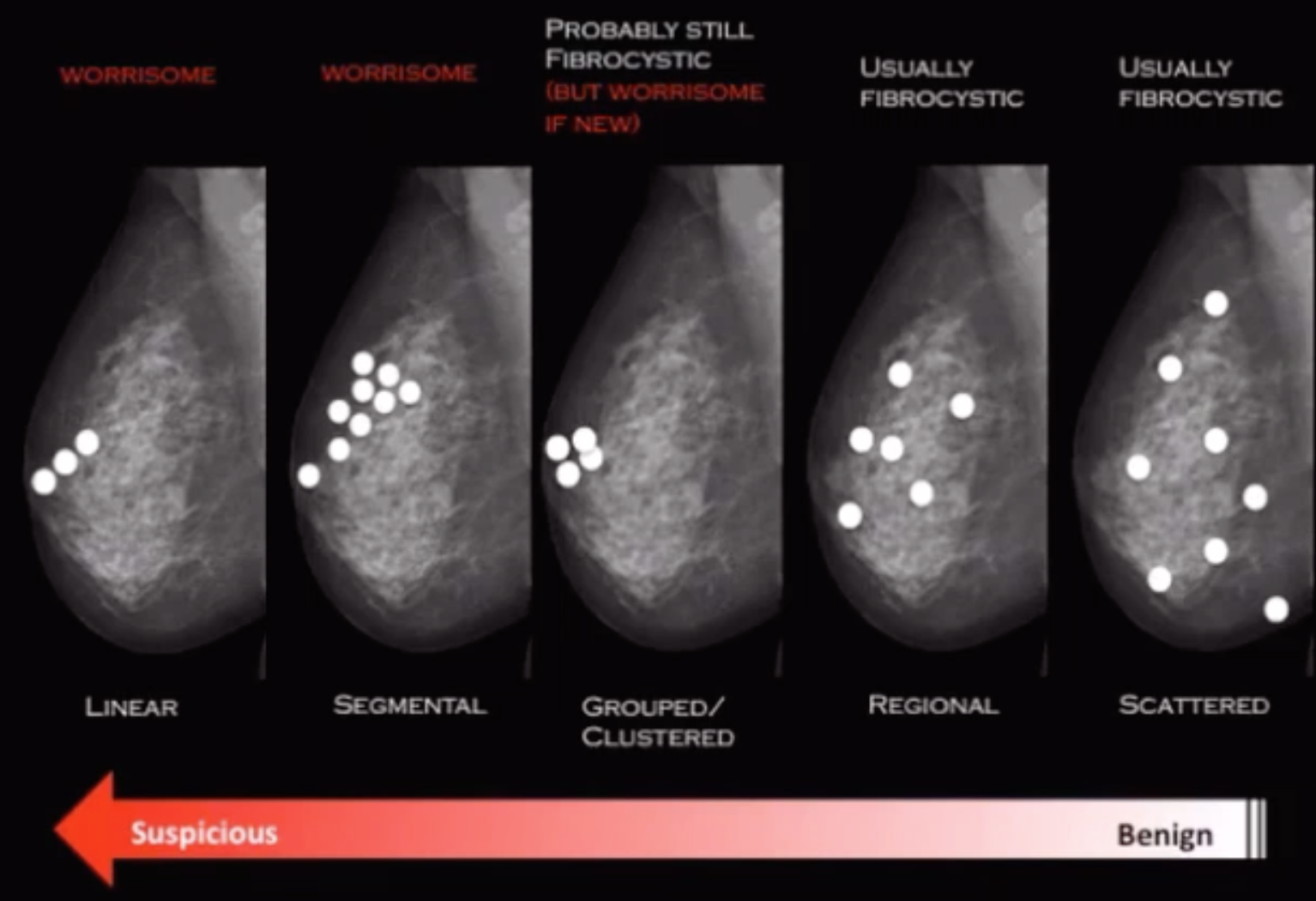
Distribution
References:
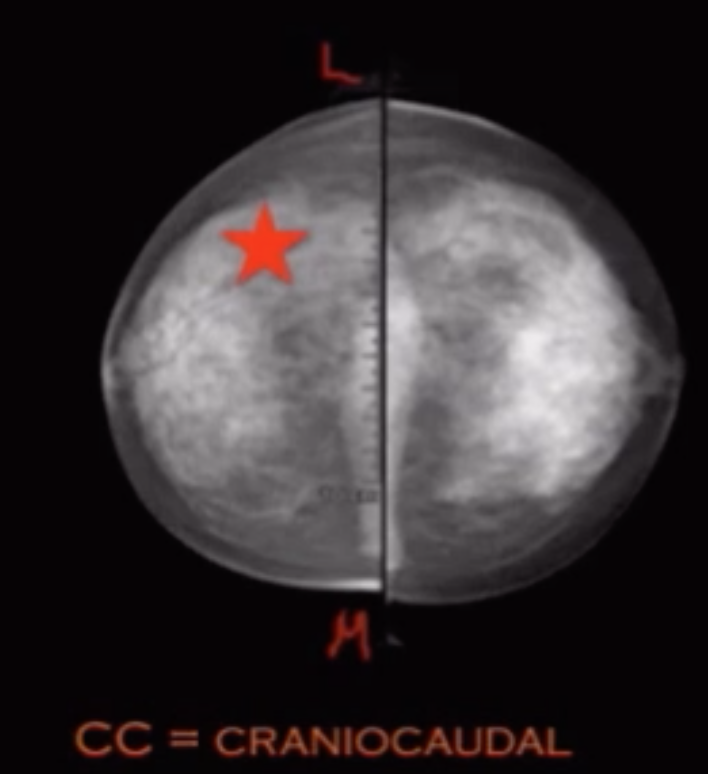
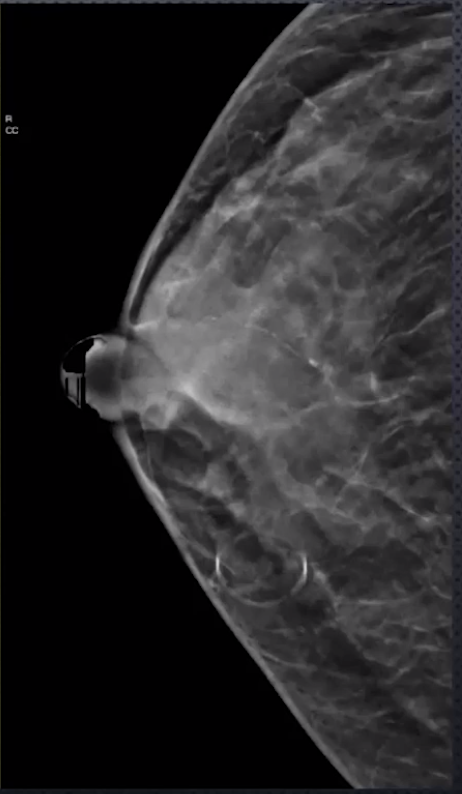
Craniocaudal (CC)
Patient faces machine
Images posterior and superior breast very well
Compressed in the axial plane
Stair-Step & Bright Line Artifacts
Type of truncation artifact
Stair step-Artifact
Tissue or object outside the margin of detector is captured by wide angle projections
Basically something is in the way of your boob and is seen in the picture when you don’t want it to it seems
Bright line artifact
When stair-step artifact is reconstructed into synthesized mammogram and appears as a bright line
Loss of Superficial Soft Tissue Resolution
Pts with big or dense breasts
Need higher XR beam energy
Lobular
Round, punctate calcifications = more benign
Due to calcification of debris, cellular material
Not specific but may be seen with
Fibrocystic changes
Milk of Calcium
Sclerosing adenosis
Intermediate to low grade DCIS
Fine Pleomorphic Calcifications
Multiple calcs, and you can actually count how many
Borders are sharp (would prick you if you held them in your hand)
DDx
Fibroadenoma (uncommonly)
Papilloma (uncommonly)
Fibrocystic change
DCIS - high grade
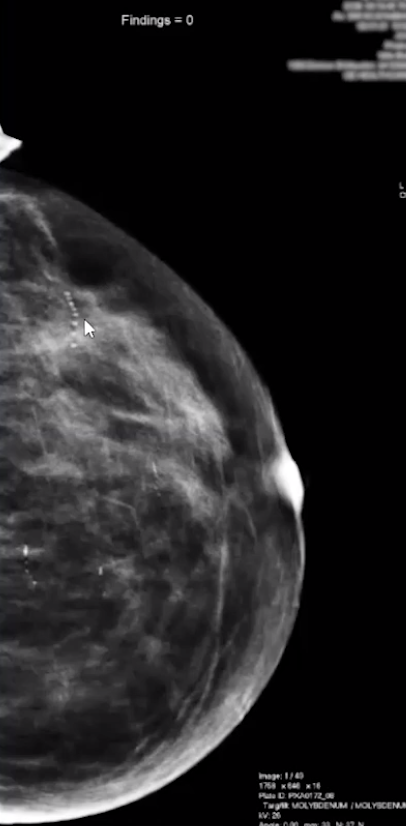
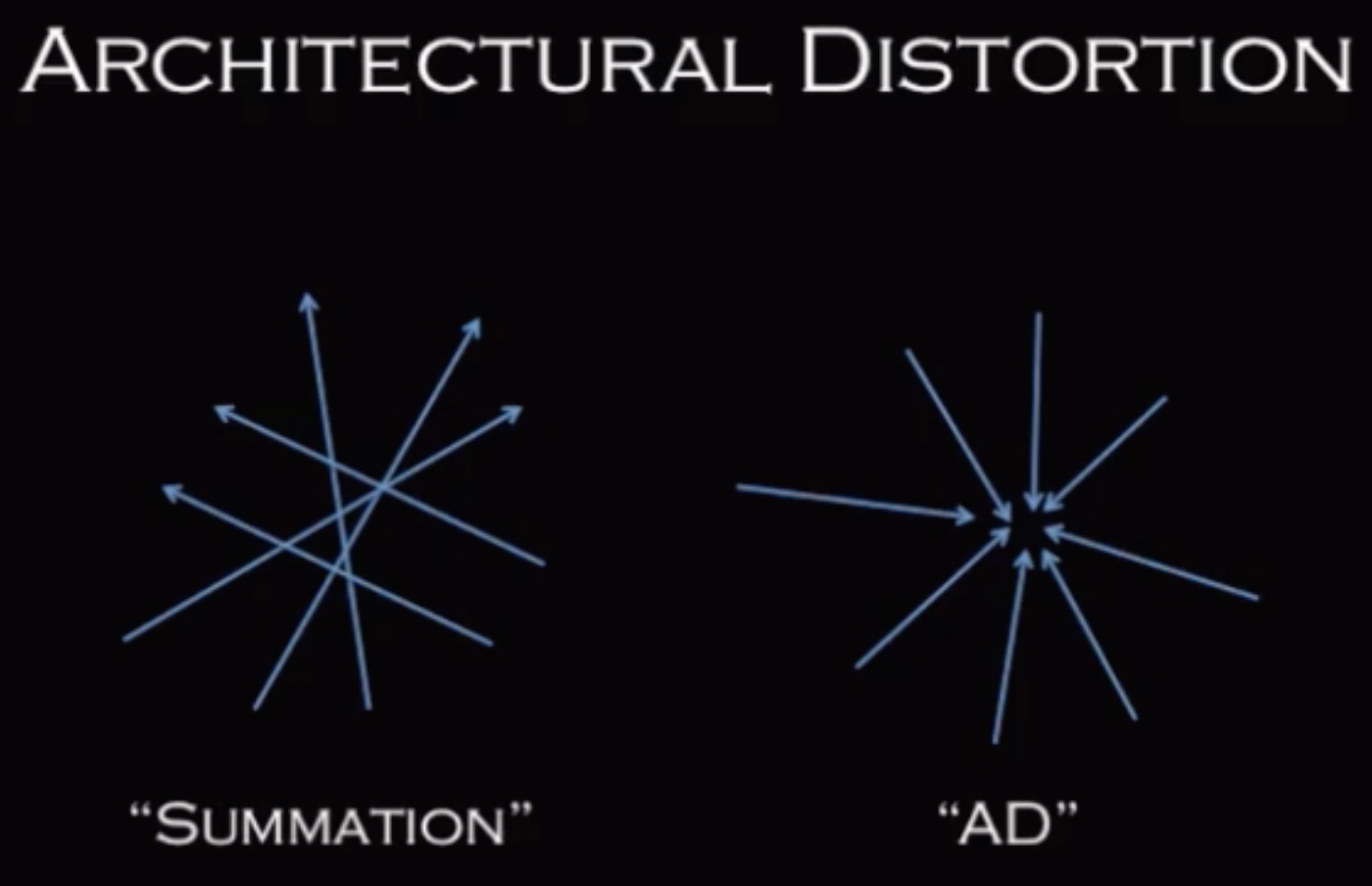
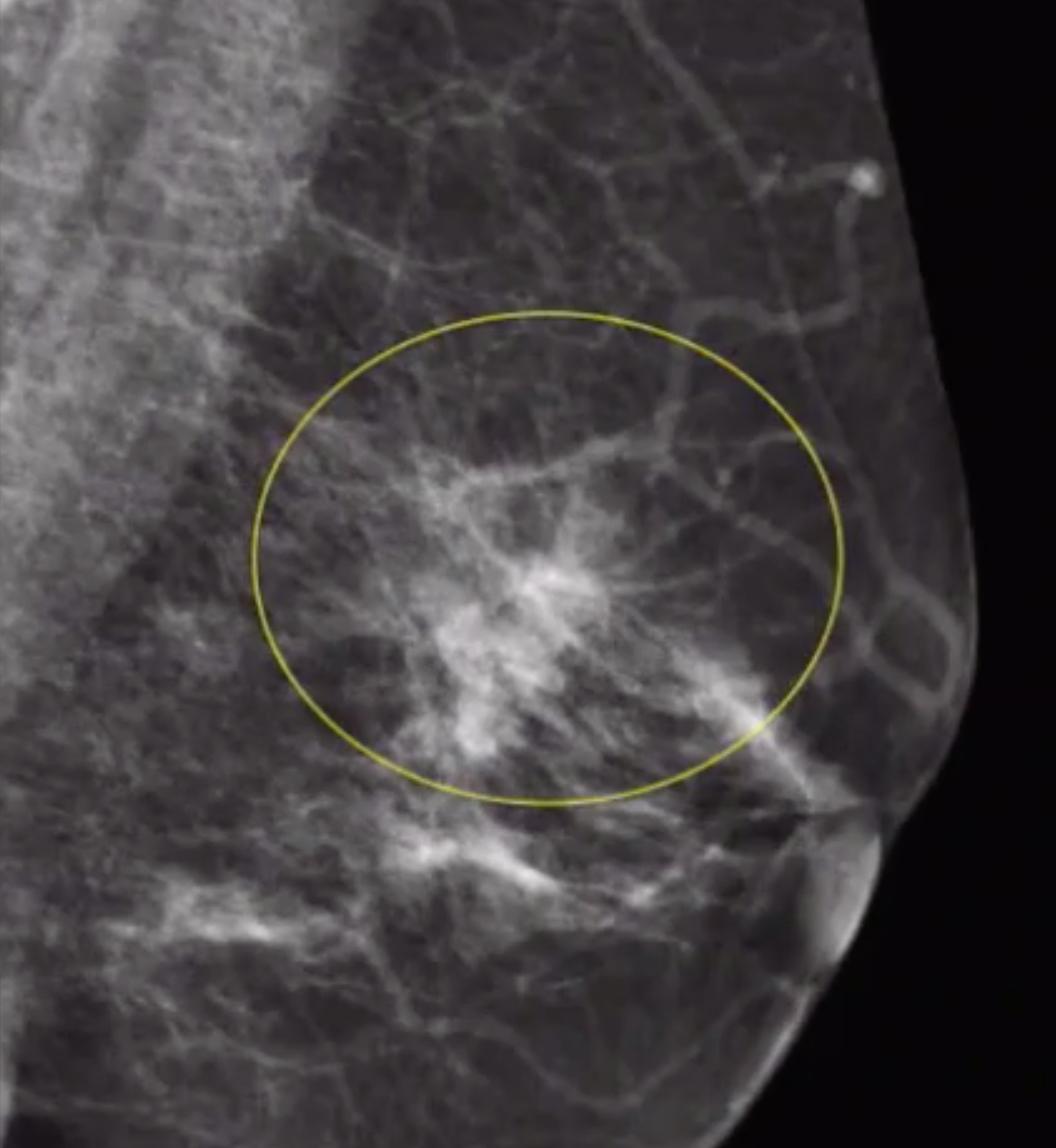
Architetcural Distrotion
DDx
Malignancy - IDC-NOS, ILC
Radial Scar
Post-surgical scar
Biopsies
3 types
US (core)
Stereotactic
MRI
90% of pathology can be diagnosed with a single first biopsy with a good tissue sample
With all biopsies but most relevant for US guided
Want the needle to be parallel to the chest wall (muscle below the breast tissue)
Want to biopsy the deeper portion first before the shallower portion
In complex masses (contain cystic and solid components), need to biopsy the solid part, not the cystic part
If biopsing a mass that is adjacent to a breast implant and you cannot safely biopsy it without the high risk of rupturing the implant, then try a stereotactic biopsy because you can do an implant displaced view and then biopsy it
Architectural Distortion