Temporal Bone
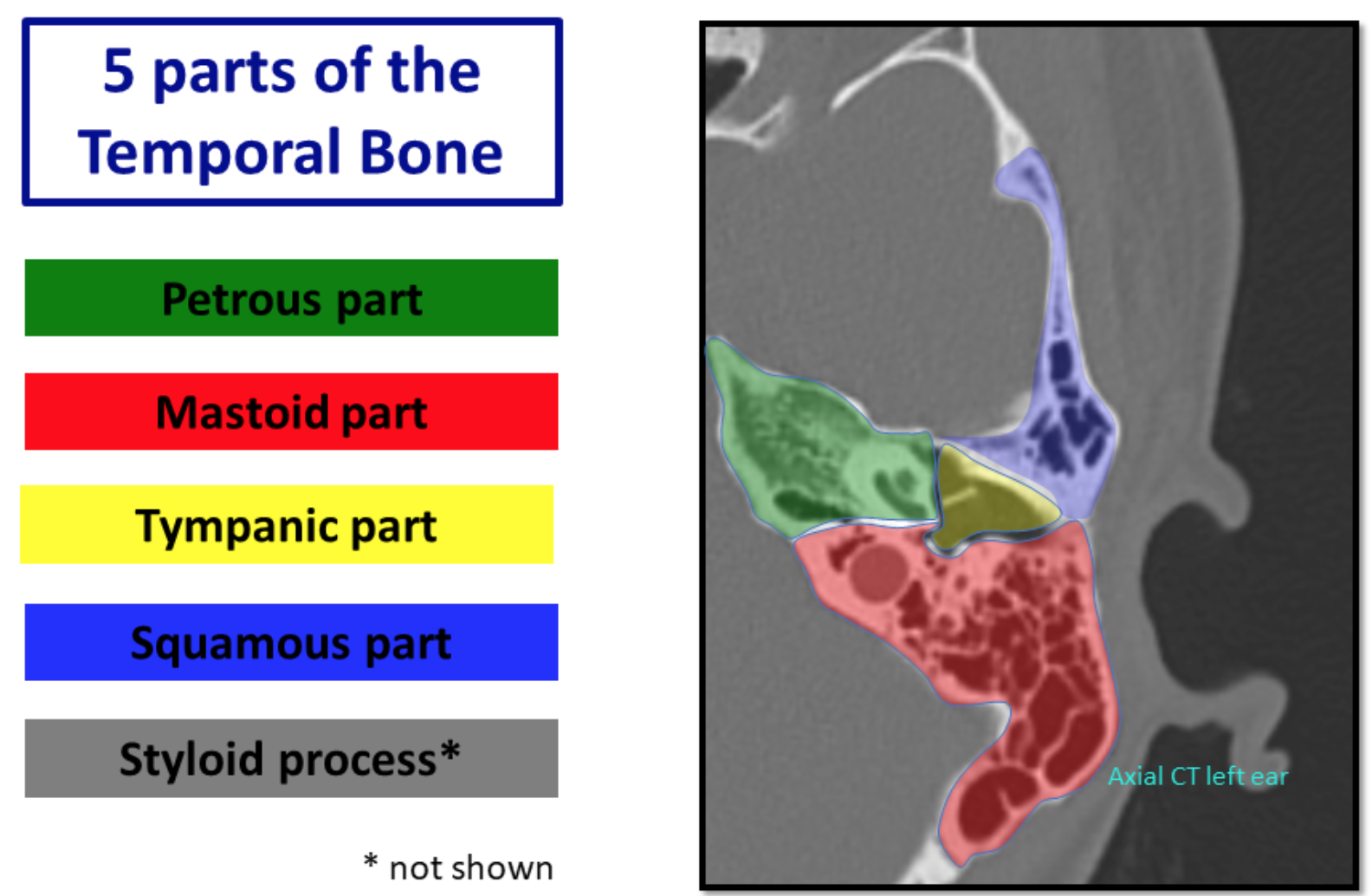
Temporal Bone Overview and Anatomy
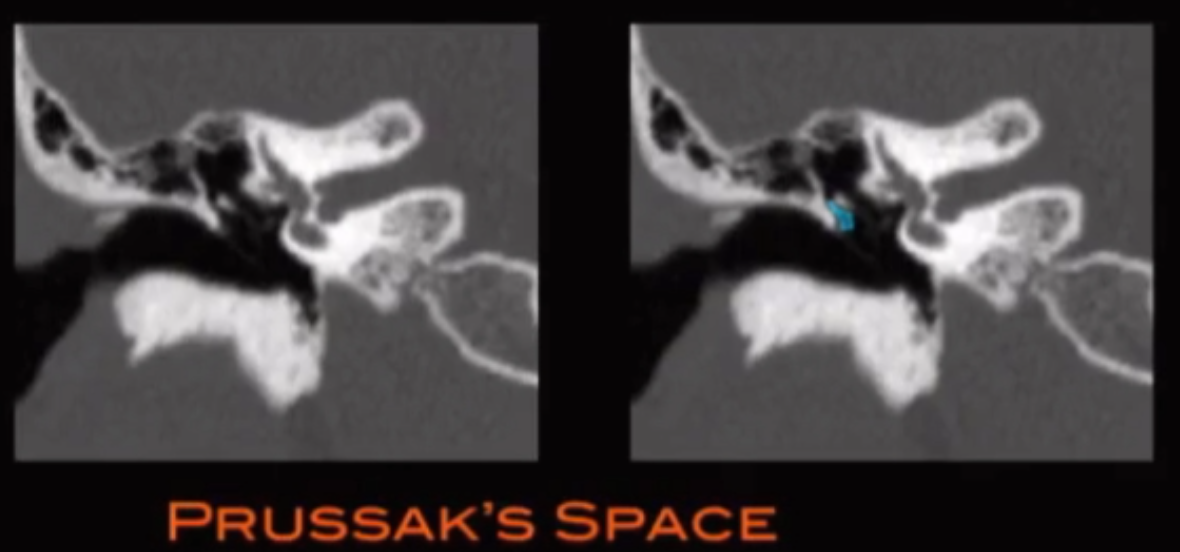
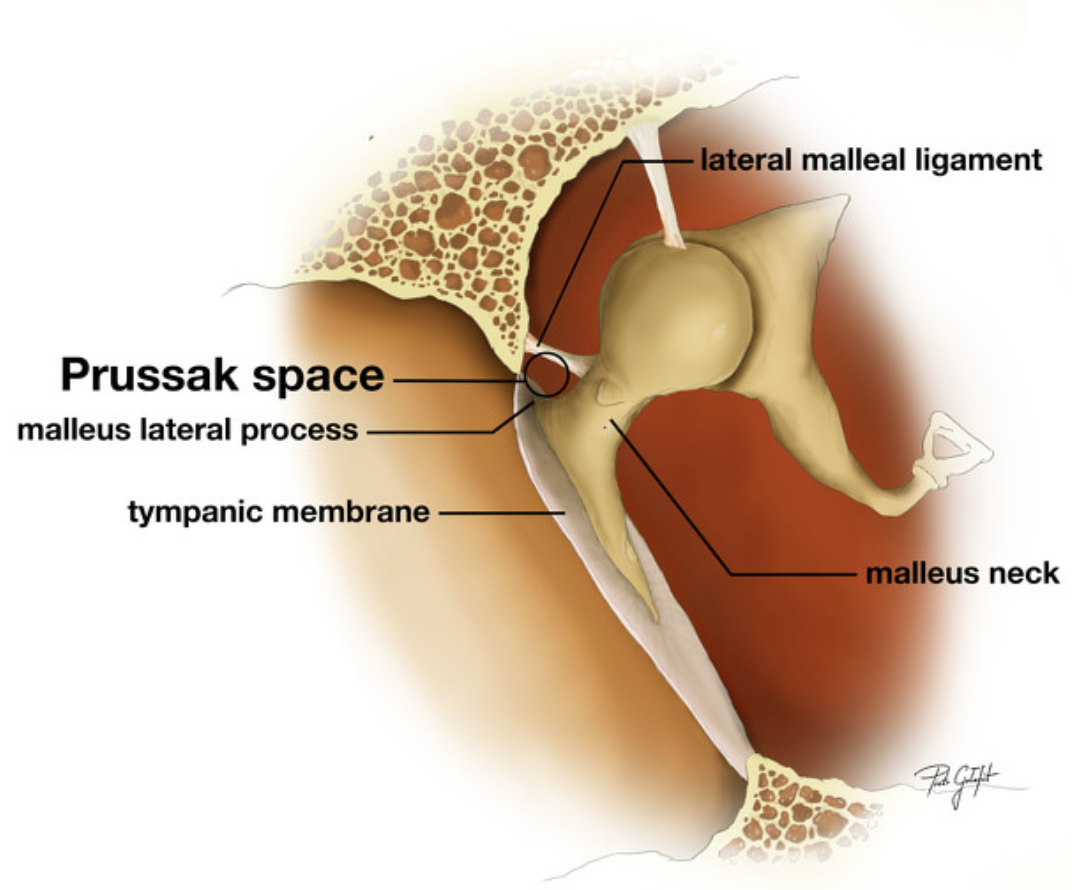
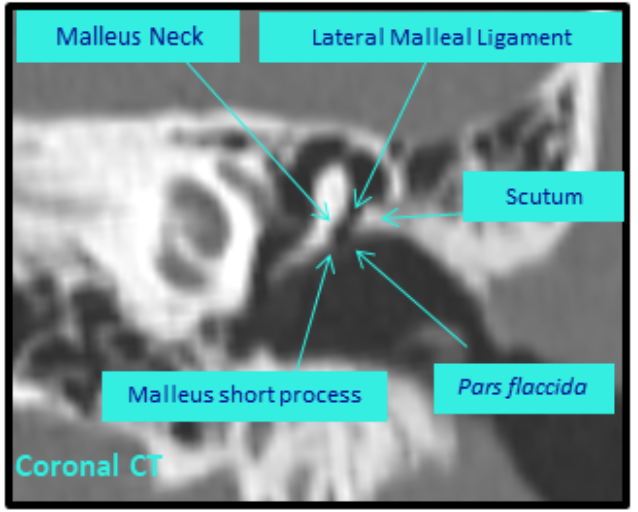
Prussak Space
Clinical relevance - cholesteatoma arise here
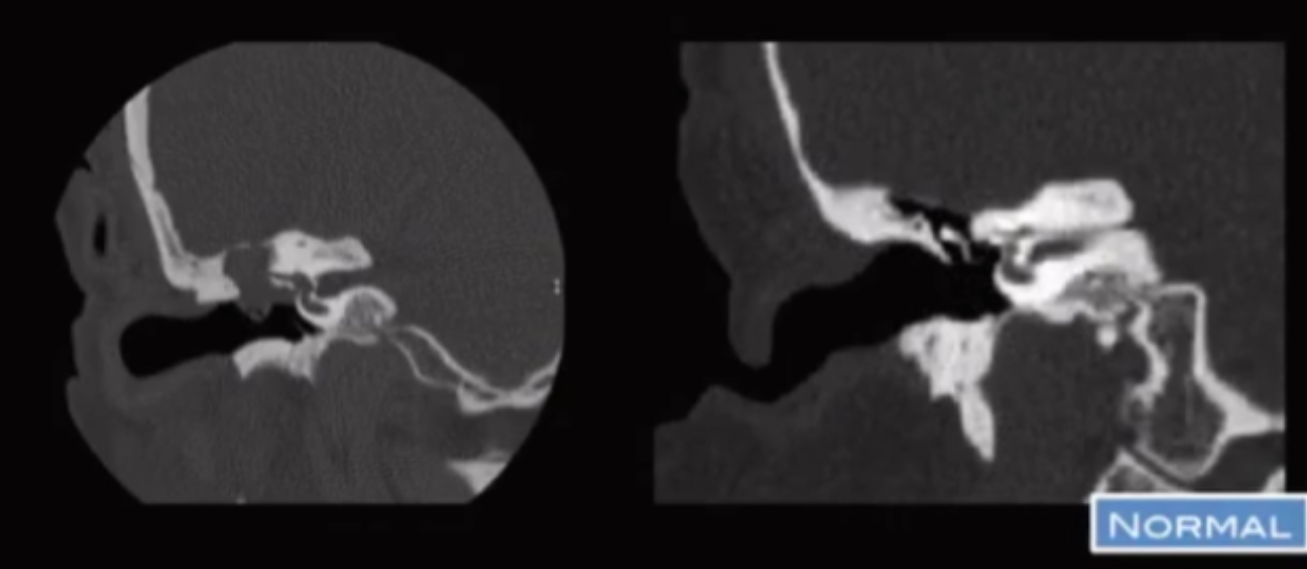
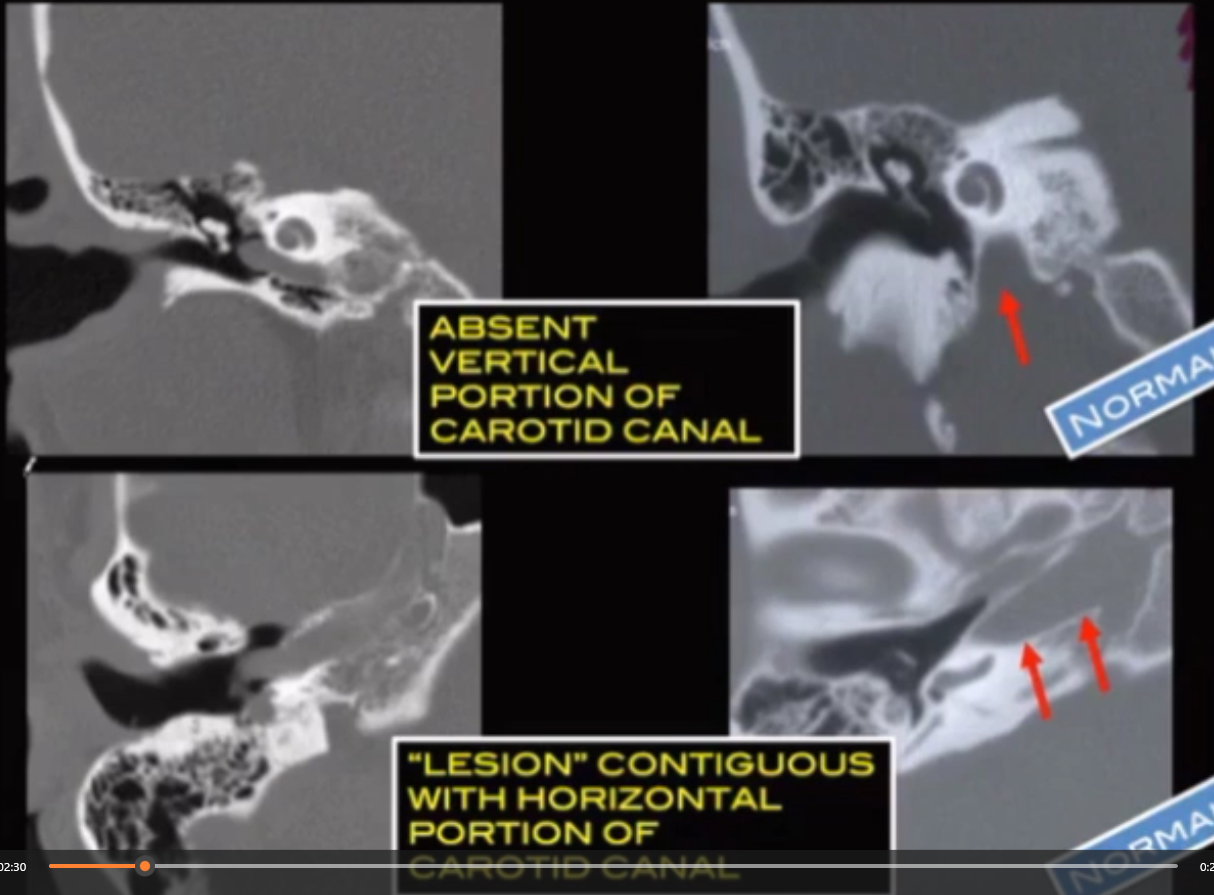
Absent Vertical Carotid Canal
So basically carotid artery has to come straight up from neck to the brain obviously
If your are missing the vertical portion in the carotid canal it will look like this where you have this soft tissue density looking thing horizontally oriented
Also notice vs the normal the lack of the vertically oriented part of the carotid canal
Do not biopsy - common question
Happens because there is regression of the cervical carotid artery and will have enlargement of the collaterals that are through the middle ear
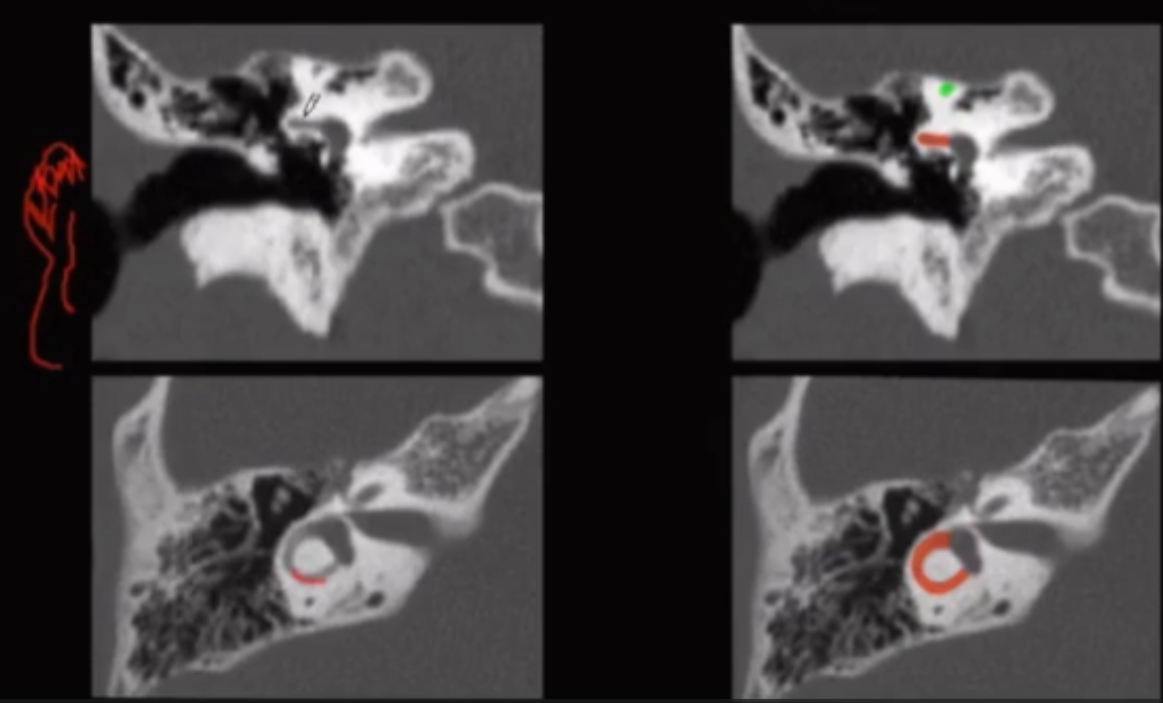
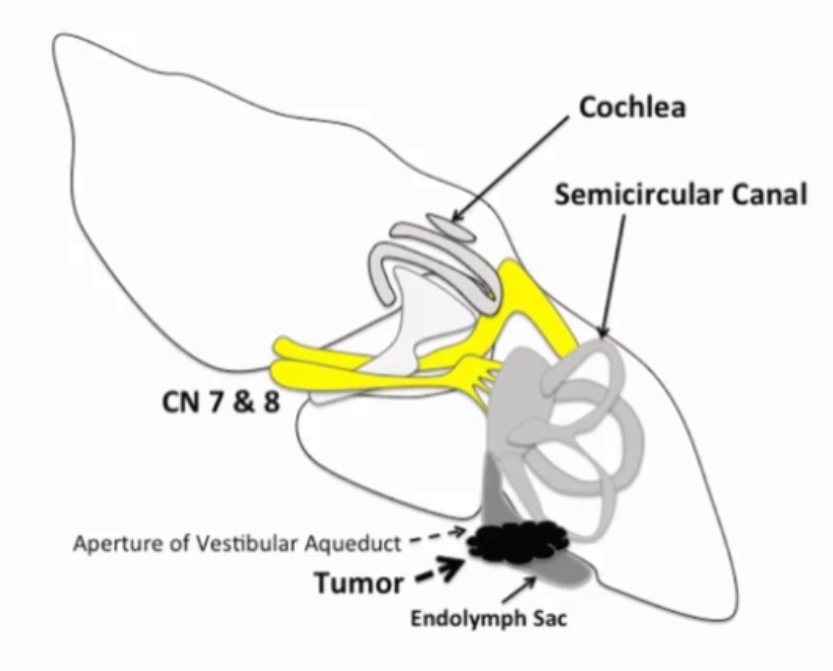
Endolymph sac Tumor
Typically papillary endolymphatic sac cystadenoma
Enhances
Internal calcifications
Looks like bone has been eaten away at
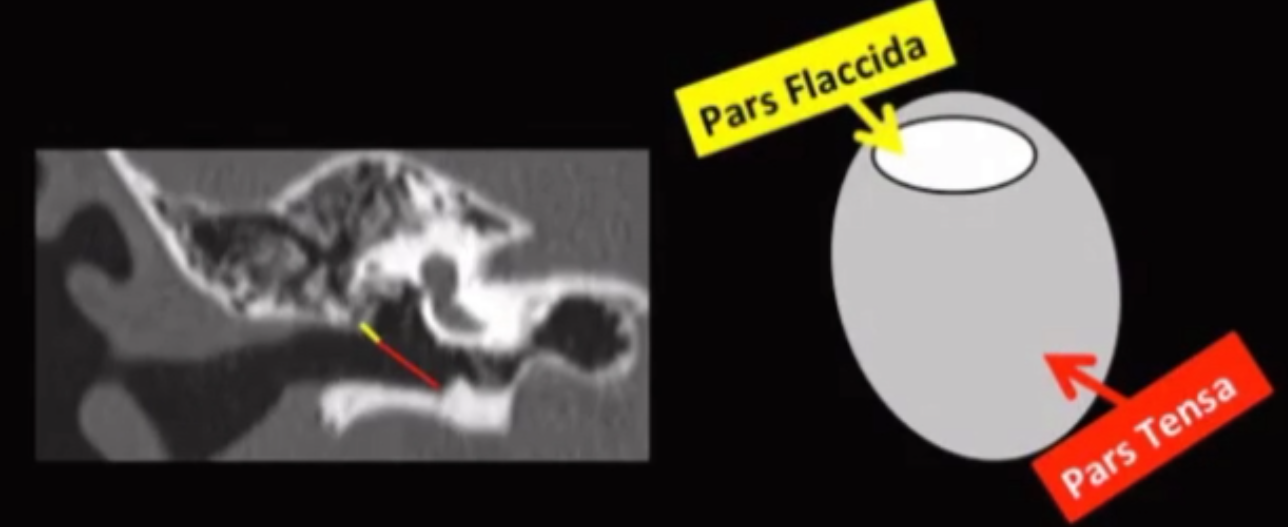
Yellow arrow points to vestibular aqueduct
Strongly associated with VHL (may be bilateral)

Pathology
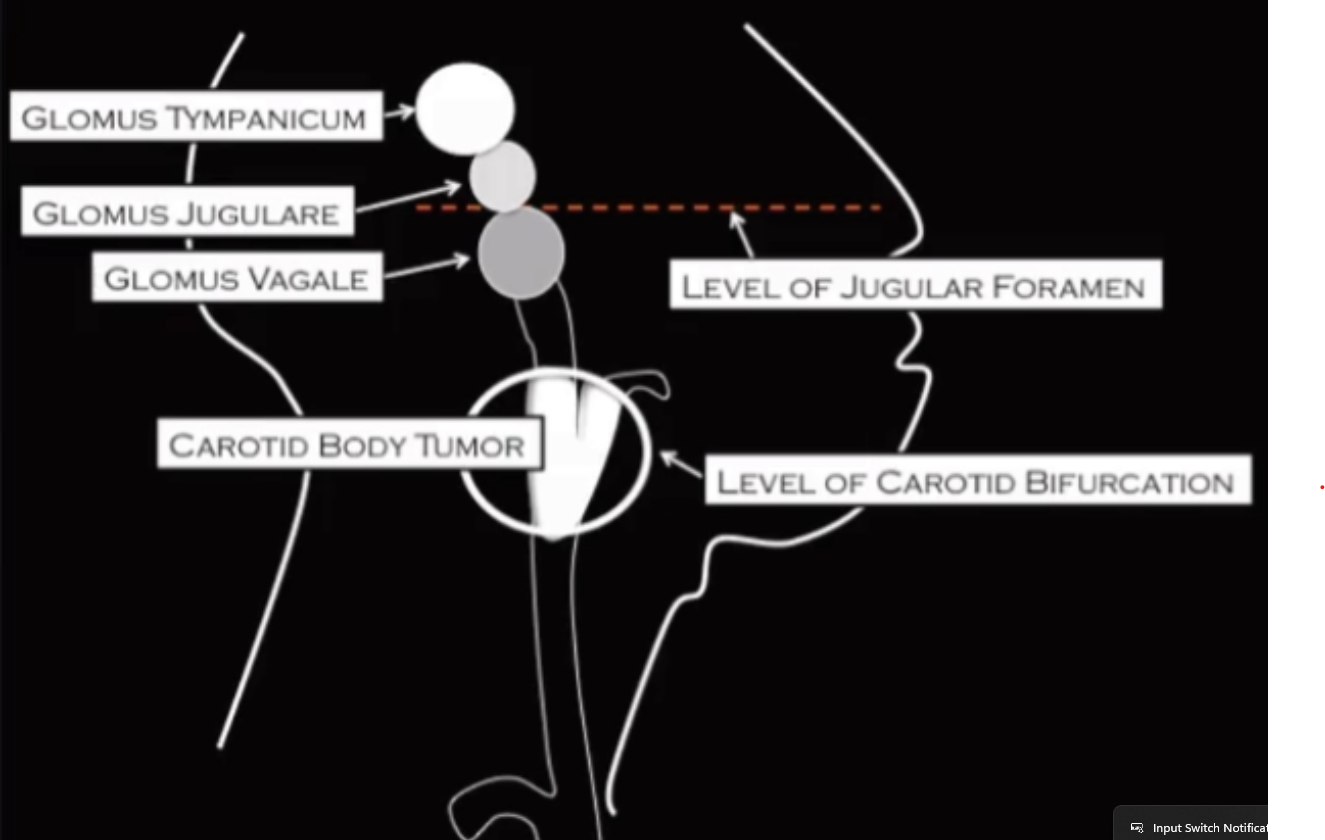
Glomus Tumor
Avidly enhances
Name depends on location
Carotid body tumor
Inferior to jugular foramen
Occurs at carotid bifurcation and will push the internal and external carotids away from each other
Most common one
Often associated with multiple ones
Commonly supplied by ascending pharyngeal artery (branch of external carotid)
Glomus vagale
Inferior to jugular foramen
Occurs laterally and results in anterior and medial displacement of the internal and external carotid arteries
Rarest form
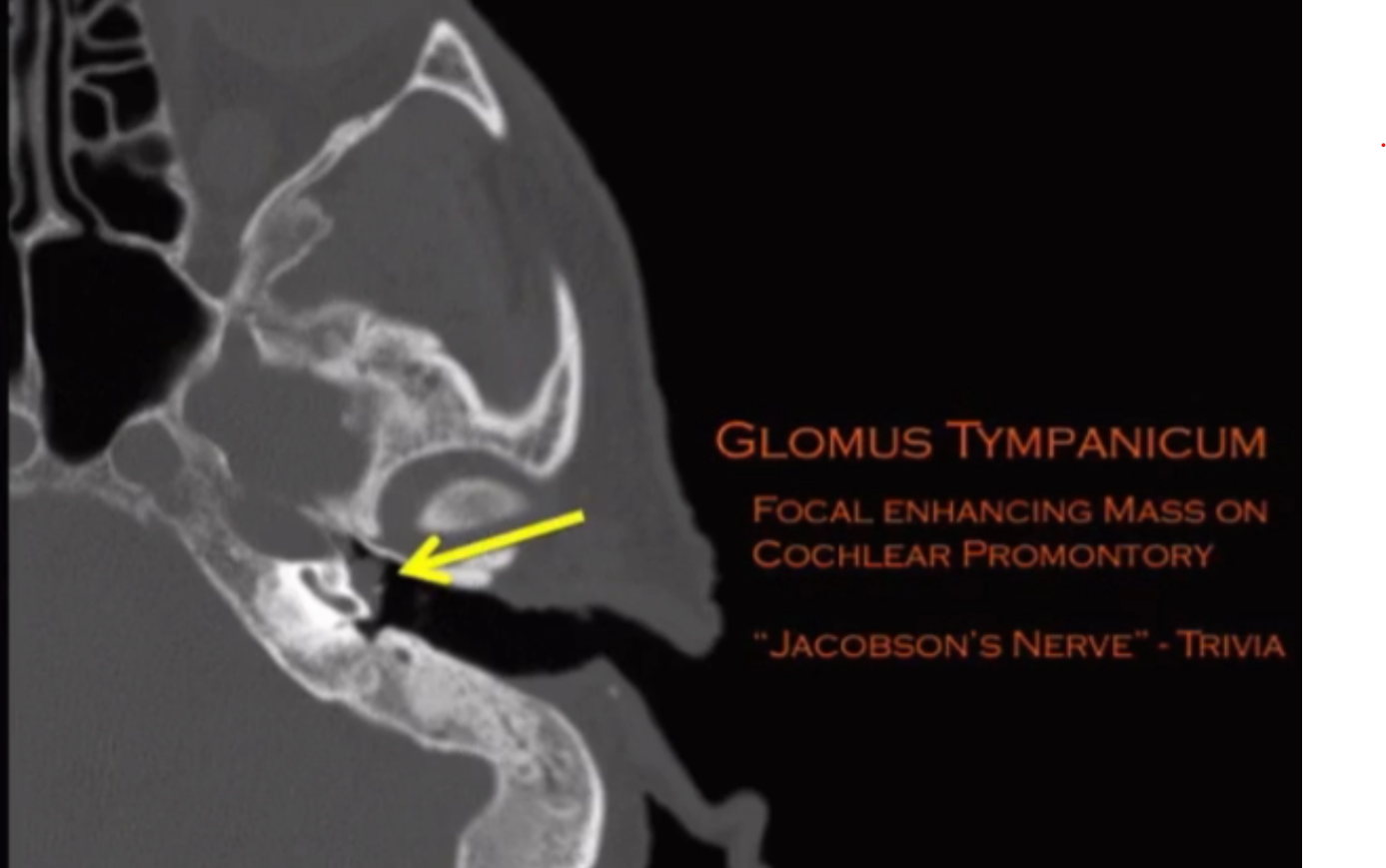
Glomus tympanicum
Superior to jugular foramen (t-bone lesion)
Occurs only in the middle ear
Jacobson’s nerve = tympanic branch of CN 9
Located at cochlear promontory where this shit arises
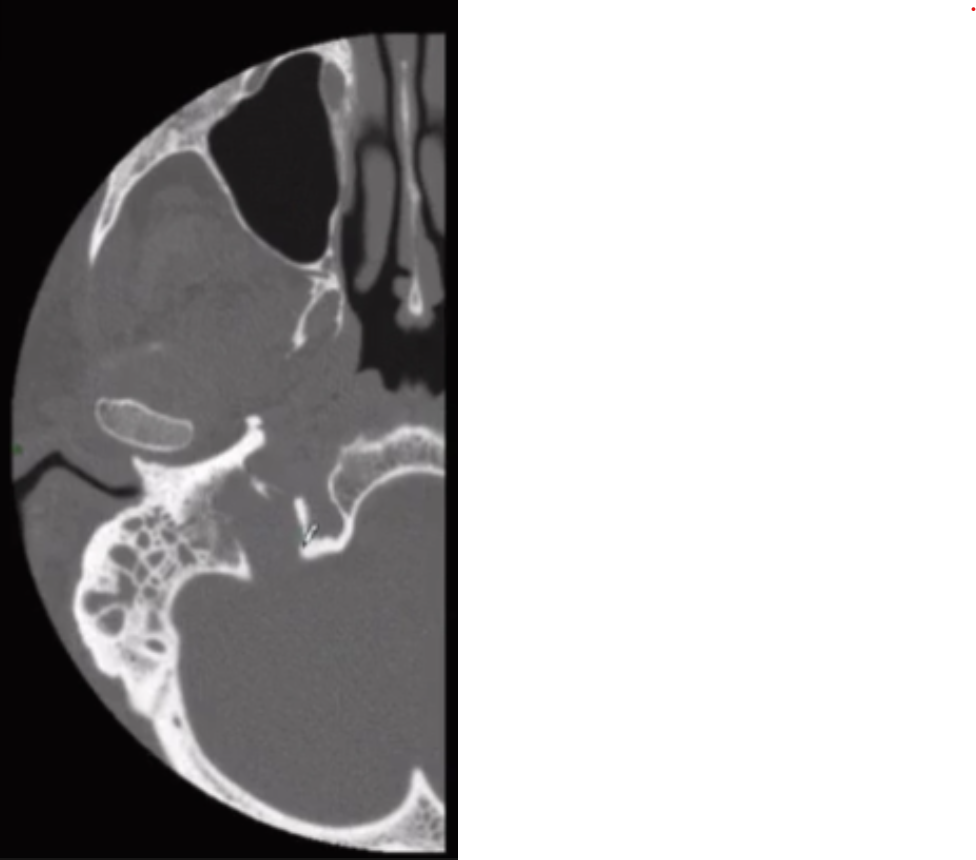
Glomus jugulare (image below tympanicum pic)
Superior to jugular foramen (t-bone lesion)
Occurs only in the jugular foramen
Permeative destruction of adjacent bone, looks like its eaten at
Cholesteatoma
Keratin and skin containing mass
Local osseous destruction
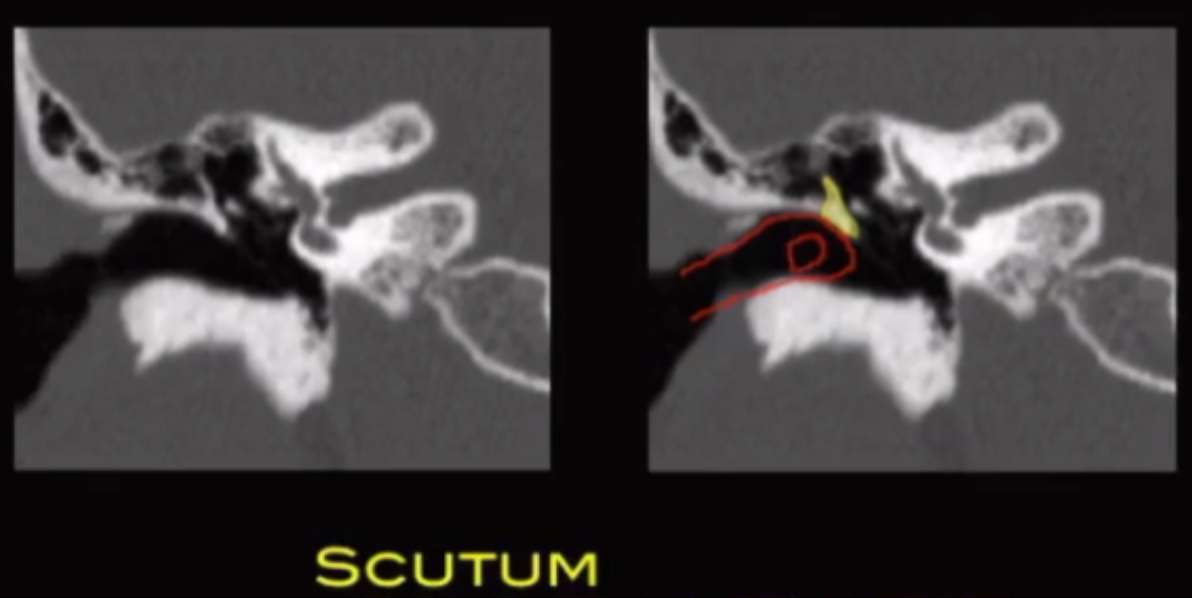
Scutum is where erosion will occur first
Scutum = shield = blocks shit that enters your ear from hitting the ossicles
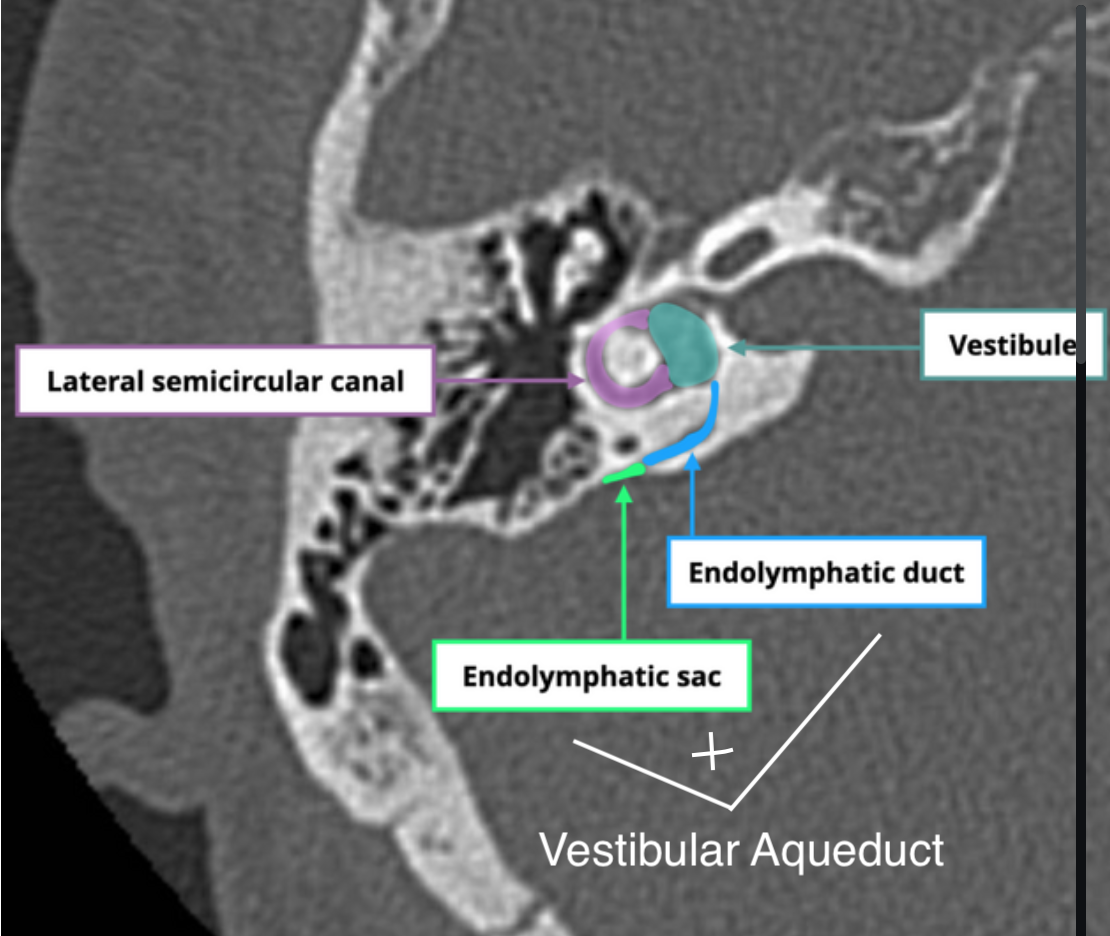
Lateral semi-circular canal (red semi circle in image below) will be the first affected by cholesteatoma
Acquired
The pars flaccida is the floppy and weak part of the TM and is located at the superior aspect of the TM
Over time the flaccida can get pushed around and create like this vacuum where flaccida is pushed inward into the ear
This will create a space for shit (like skin and debris) to accumulate which forms the cholesteatoma
Now when the mass gets big enough it will continue to push the flaccida into the ear and remember since flaccida is at the superior aspect of the TM it will push in and upward into Prussak space
Prussak space is where these will occur
Congenital
Need to differentiate between cholesteatoma and otomastoiditis
Cholesteatoma will destroy the ossicles, otomastoiditis typically would not
Tympanium
Can described by using epi, meso and hypo -tympanum
If you stick your finger in your ear
Everything above = epitympanum
Everything at level of finger = mesotympanum
Everything below = hypotympanum
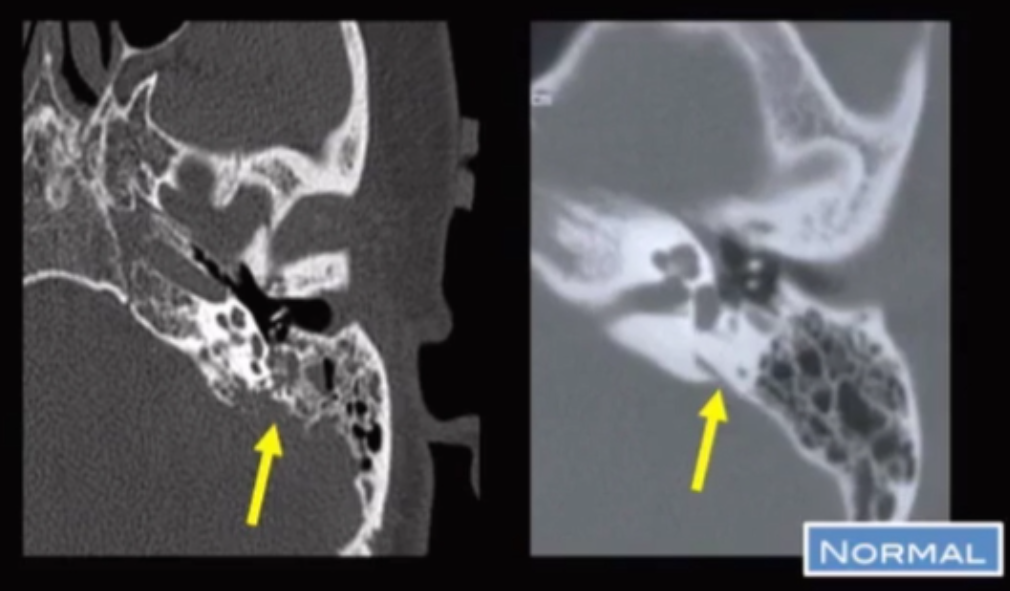
Vestibular Aqueduct enlargement
Vestibular aqueduct = tube that extends from vestibule to petrous temporal bone and contains endolymphatic sac and endolymphatic duct
Enlargement of vestibualr aqueduct can cause hearing issues