Spine Masses
For all spine masses need to determine
Intramedullary vs. Intradural Extramedullary vs. Extradural
Age
Location doesn’t help much in the spine
Imaging characteristic - whatever, anything can look anyway, look for key differences
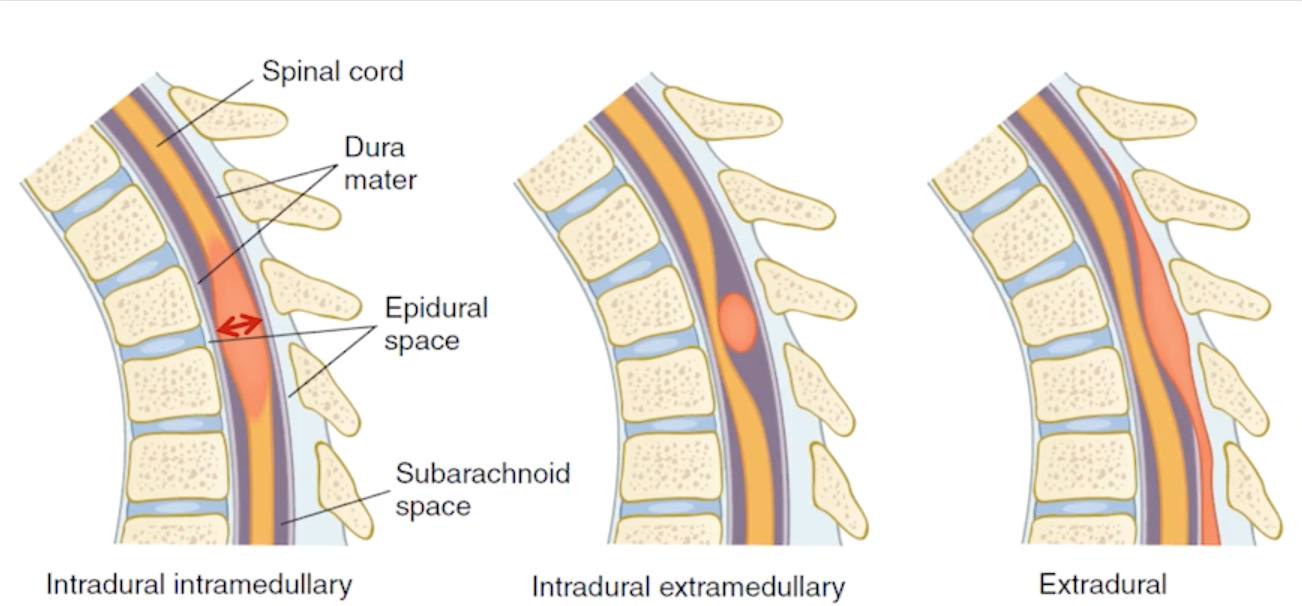
Intramedullary
Astrocytoma
Ependymoma (not myxopapillary form)
Hemangioblastoma (can be extramedullary)
Syringohydromyelia
Intra-dural Extra-medullary
Meningioma
Nerve sheath tumors (schwannomas, neurofibromas)
Hemangioblastoma (can be extramedullary)
Syringohydromyelia
Myxopapillary ependymoma
Drop mets
Intramedullary
Astrocytoma & Ependymoma
T1-hypo
T2-hyper
Variable enhancement
Associated with NF
Involves entire cord/longer segments —> favors astrocytoma
Cysts and hemorrhage —> favors ependymoma
Ependymoma
Adults (40s)
Cysts and hemorrhage —> favors ependymoma vs astro
Cellular form
Myxopapillary form
Intradural & Extramedullary (others are intramedullary)
Seen at filum terminale / conus - a solitary lesion in this location is highly suggestive of MPE
Meningiomas
Multiple meningiomas —>NF
Strong enhancement
Broad dural base
Note: schwannomas will not have broad base, commonly extend through neural foramen and are more likely to undergo cystic necrosis due to less vascularity
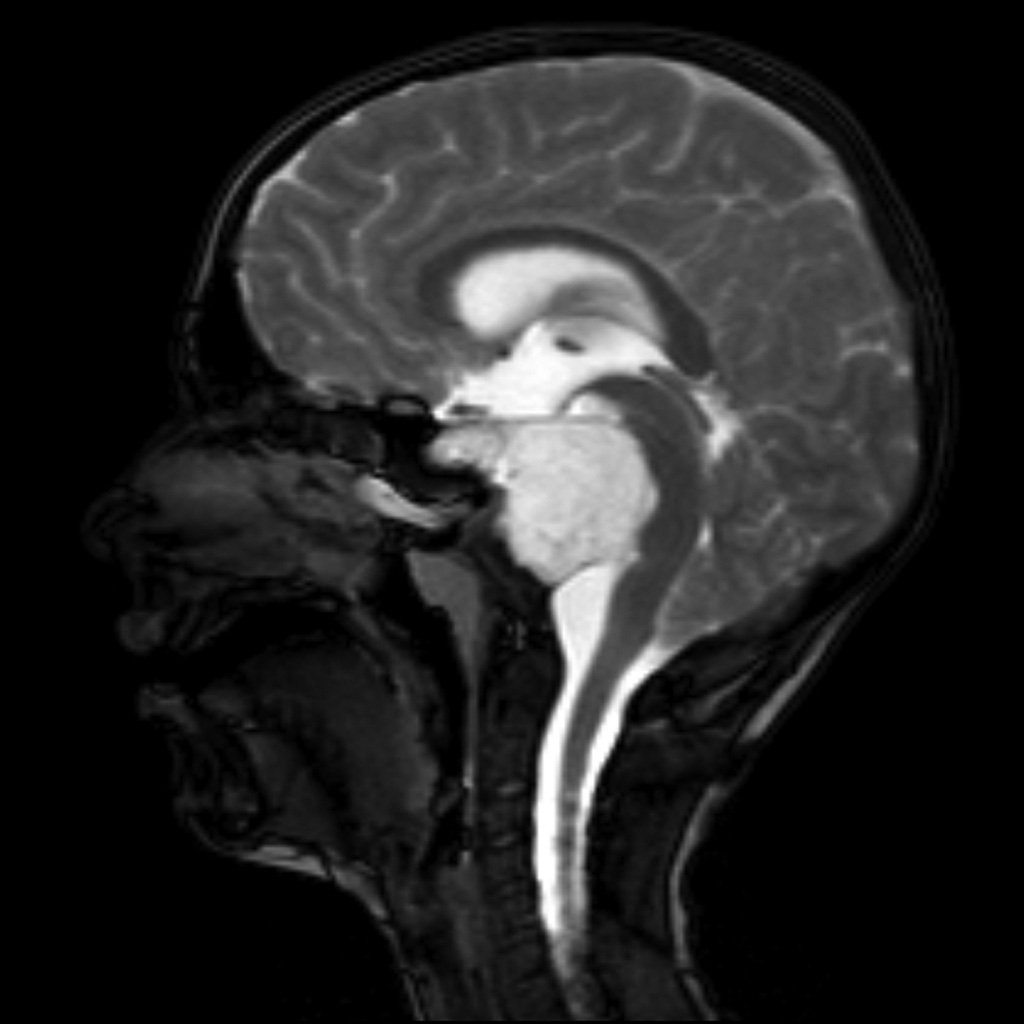
Chordoma
Arise from notochord (therefore can arise anywhere from sacrum to sella)
Locally aggressive bone mass
Commonly present in spheno-occipital (near clivus) (young adults) or sacro-coccygeal (older adults) regions - typically in midline
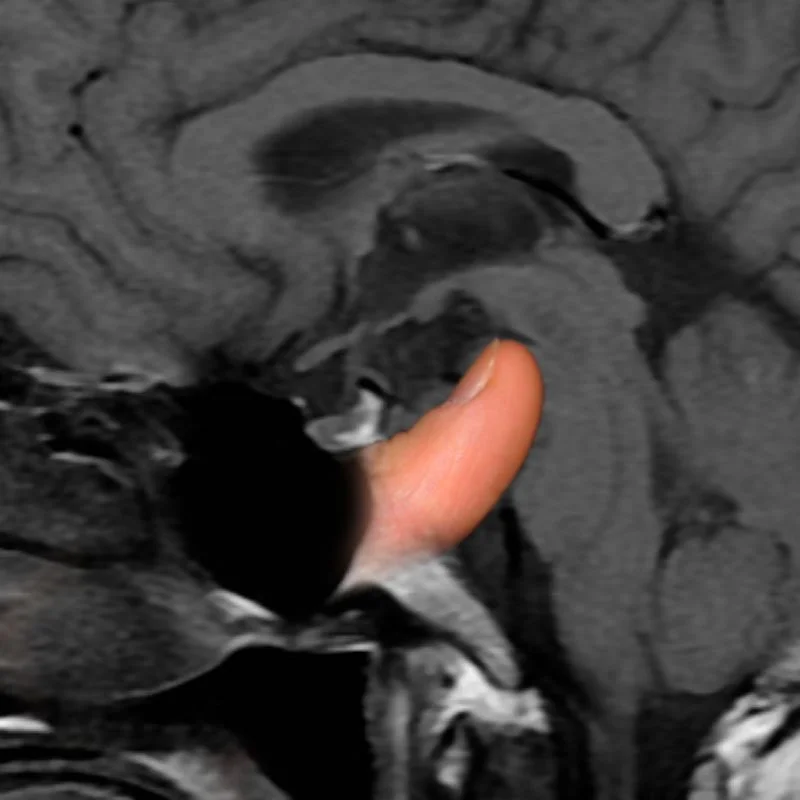
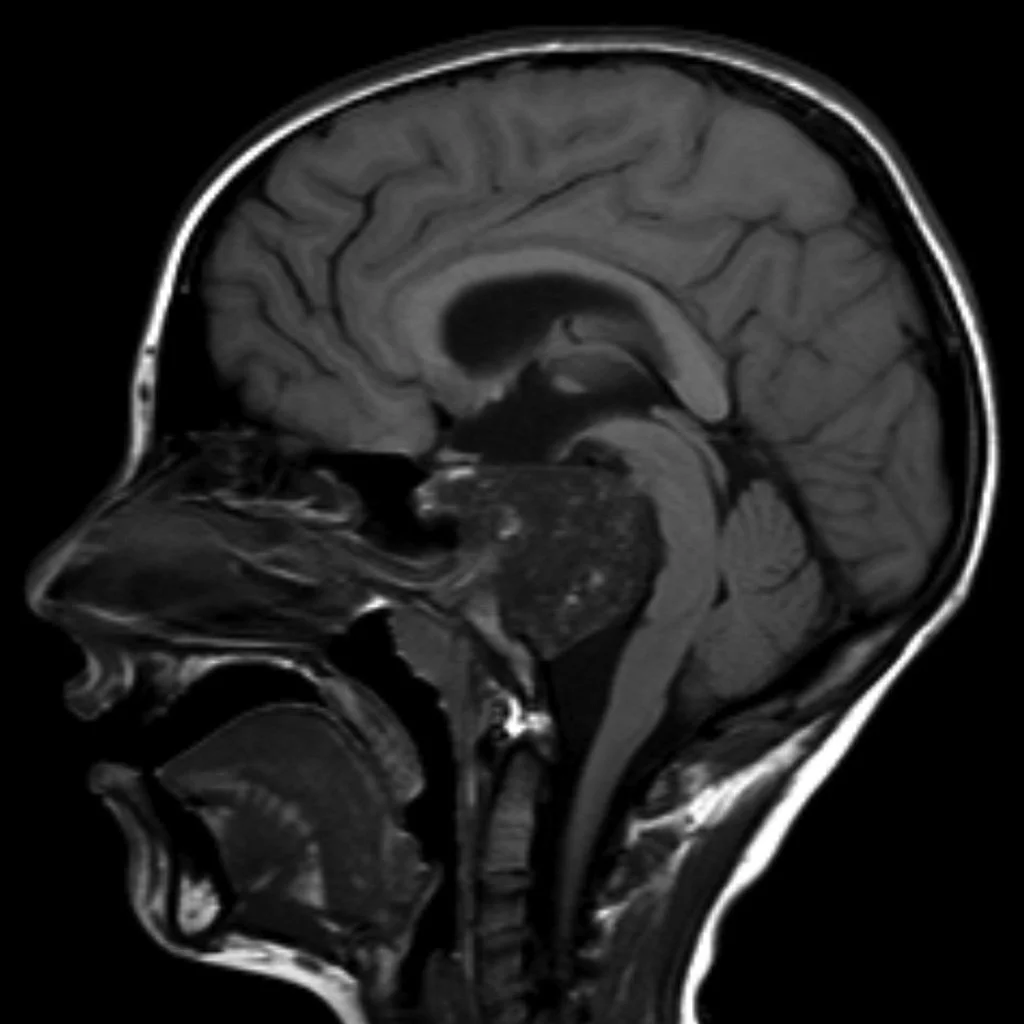
Thumb sign - the chordoma projects posteriorly causing mass effect on the anterior aspect of the pons as if your thumb was pushing it back
Hyperattenuating and well circumscribed, may have intra-lesional calcifications (from erosion of local bone)
MR:
T1: low sign
T2: high signal
Typically septated
T1 C+: heterogenous enhancement with honeycombing appearance
Astrocytoma
Kids to 30s (on younger side vs ependymomas)
Upper half of spinal cord
Affects multiple vertebral levels of cord
Protoplasmic form
Involves entire cord/longer segments —> favors astrocytoma vs ependymoma
Pseudomeningocele
Abnormal collection of CSF due to a defect in the dura, typically from trauma/surgery
Should evaluate for nerve root injury if you see pseudomeningocele
Should also look for superficial siderosis - (T1/T2 hypo, blooming on SWI)
Terminal Ventricle
Normal variant
Large cystic lesion at distal tip of spinal cord
Meningocele
Protrusion of meninges through defect in skull/spine
Scar tissue
Can occur anywhere after surgery and look like an irregular shaped mass near the surgical site
Will enhance
Disc will not enhance
Tarlov Cyst (Perineural Cyst)
CSF filled dilation of nerve root sheath (basically CSF filled cyst)
Extra-dural (but do contain neural tissue)
Associated with connective tissue disease (marfans, Ehlers danlos, etc)
Typically asymptomatic, may cause mass effect causing related symptoms to whatever they compress
Findings
Will follow CSF characteristics
T1: low signal
T2: high signal
T1 C+: does not enhance
Extra-dural
Angiolipoma
Chordomas
Giant cell tumors
Hemangiomas
Sarcomas
Mets (ascend via batson plexus)
Disc Disease
Nerve Sheath Tumor (Schwannomas & Neurofibromas)
Typically arise from dorsal nerve roots but are extrinsic to the nerve itself
Adults (50s)
Dumbbell appearance (half of mass is intraspinal and part extraspinal with waist compressed at nerual foramen)
Neurofibromas —> NF1
Lipomyelomeningocele

Giant Cell Tumor
Heterogenous signal
Hypo on T2
Blood products

Chondrosarcoma
Chondroid matrix - rings and arcs
T2 bright
Septations present
References:
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 7880 (chrodoma case)
Case courtesy of Bruno Di Muzio, Radiopaedia.org, rID: 43095 (tarlov cyst case)