Spine (All Other)
Scheuermann Disease
Essentially kyphosis secondary to multiple schmorl’s nodes which causes anterior wedging of the vertebral body and therefore secondary kyphosis (exact mechanism debated)
Primarily affects thoracic spine
Mostly seen in kids 13-17
Sorensen criteria (abbreviated)
3+ contiguous vertebra with >5 degrees of wedging AND
Thoracic kyphosis >40 degrees (or thoracolumbar kyphosis >30 degrees)
May also need schmorl’s nodes and anterior end-plate irregularities based on source
Chance fracture
Bertolotti Fracture
Transitional lumbar vertebra with associated back pain
Herniations
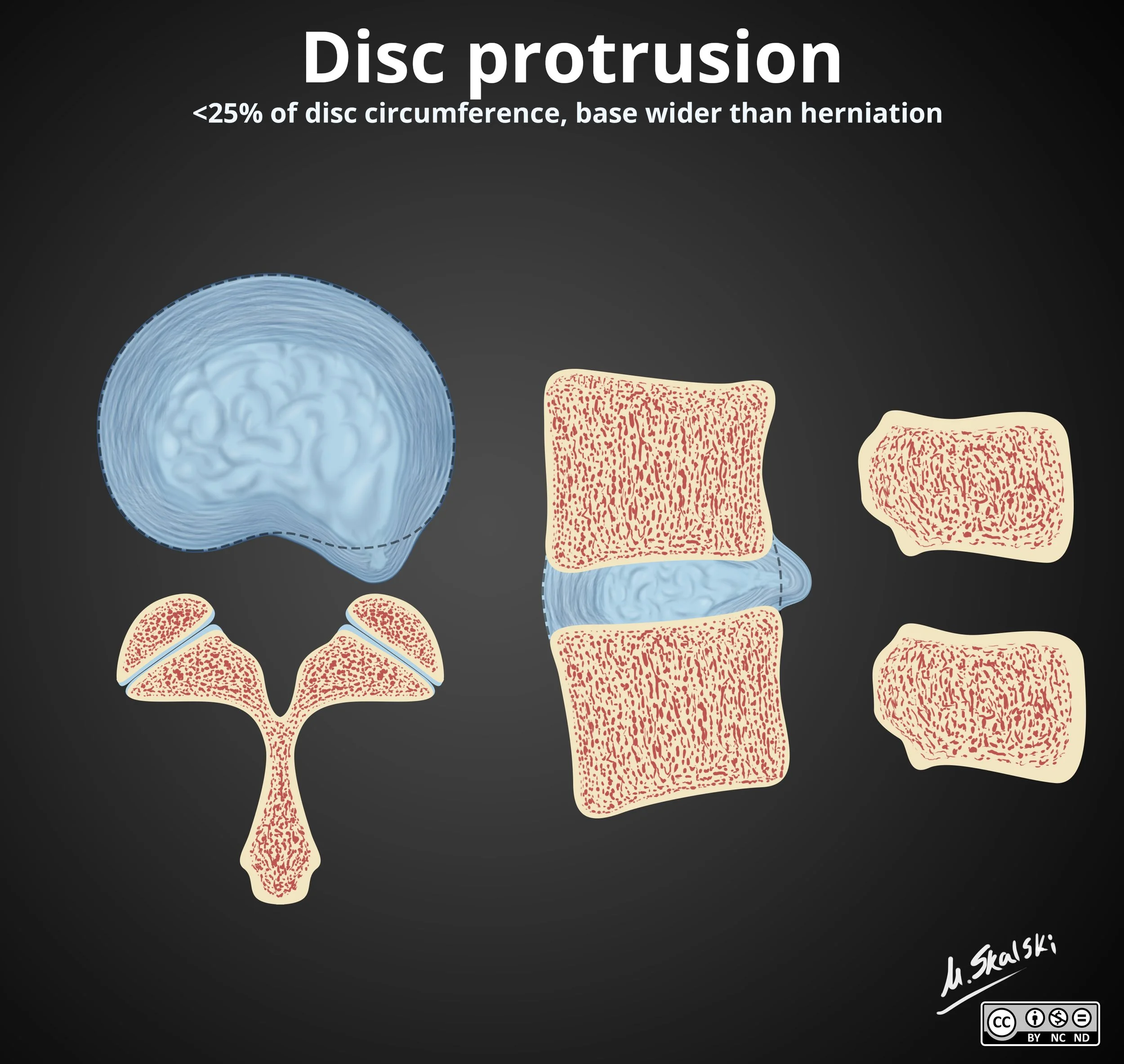
Disc Protrusion
Cannot have free fragment
Discitis-Osteomyelitis
Starts in disc endplate —> disc —> next vertebral level endplate
Note: mets will look similar but almost never involves the disc
TB
Multilevel endplate disease, commonly anterior spread
Spares the discs
Concurrent psoas abscess common
Gibbus deformity may be seen
Severe kyphosis with destruction of vertebral body
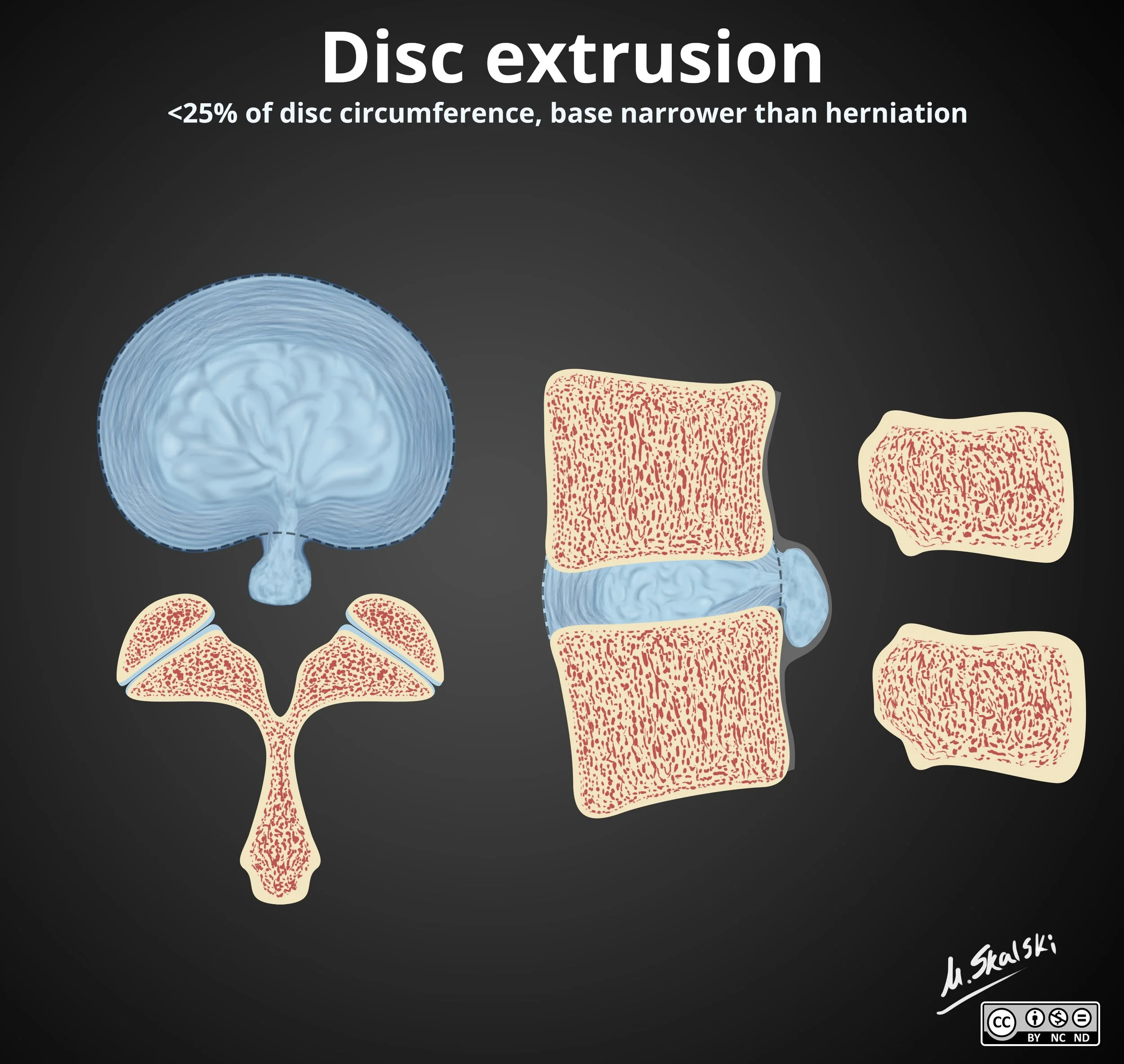
Disc Extrusion
Can have free fragment
Guillain Barre Syndrome
Nerve root enhancement
Anterior nerve roots affected more than posterior nerve roots
Ascending flaccid paralysis
Facial nerve enhancement is most commonly affected CN
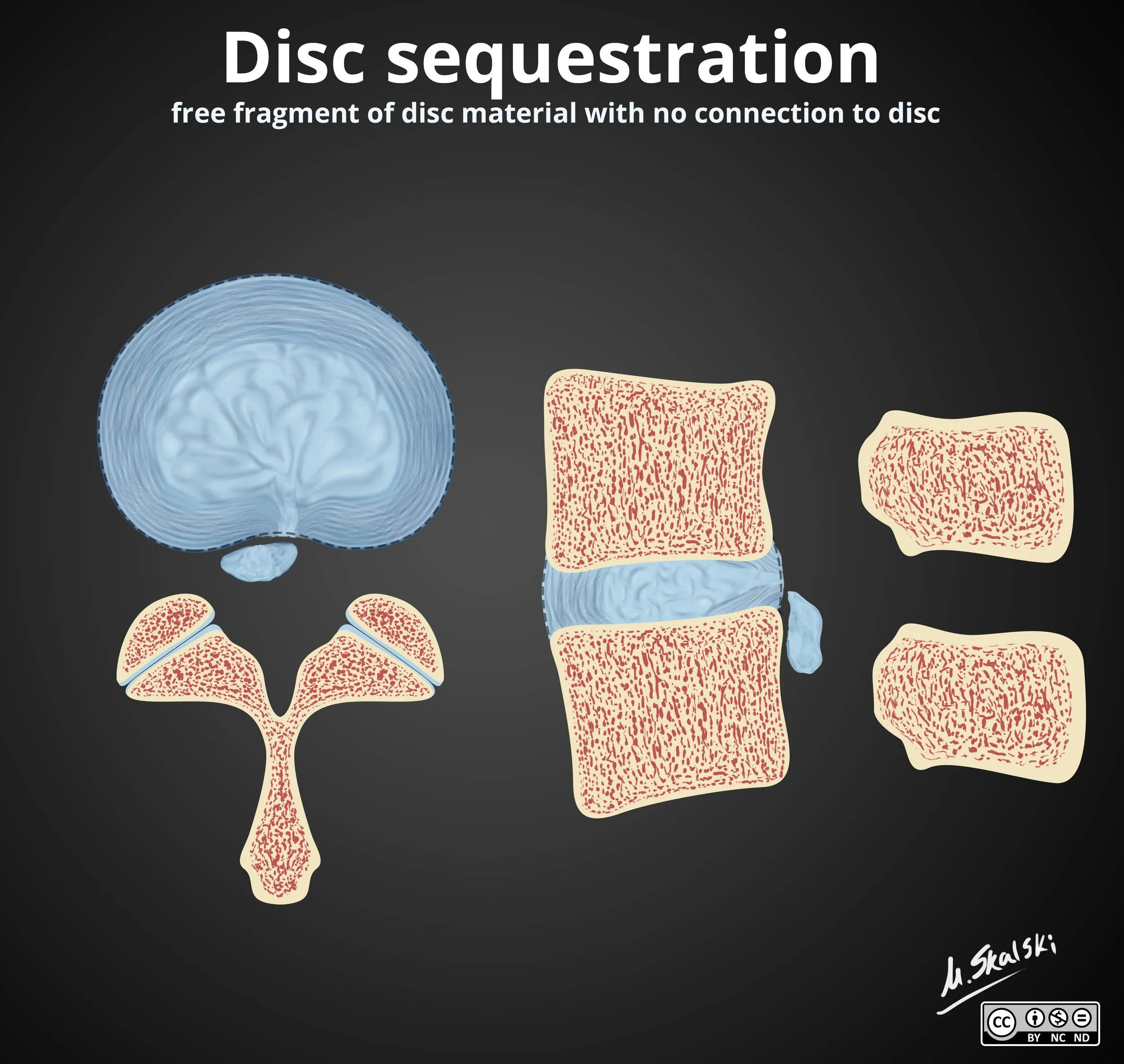
Disc Sequestration
This is the free fragment
Piece of disc breaks off and migrates
Tethered Cord Syndrome
End of cord normally ends at T12-L2
In Tethered cord the conus typically terminates below L2 (85% of cases) and is normal 15% of the time
Typically has filar cyst or lipoma at end of thecal sac
I think of this mass being the anchor that pulls the cord all the way down pulling it taught so that it is beyond the normal endpoint
Thickened filum terminale (>2 mm) may be the only finding if the cord terminates at normal level
Associated with dysraphic sacrum
Who should get screened? Patients with
Anal atresia - VACTERL
Spina bifida
Note: Patients with dimples below the gluteal crease do not need to be screened
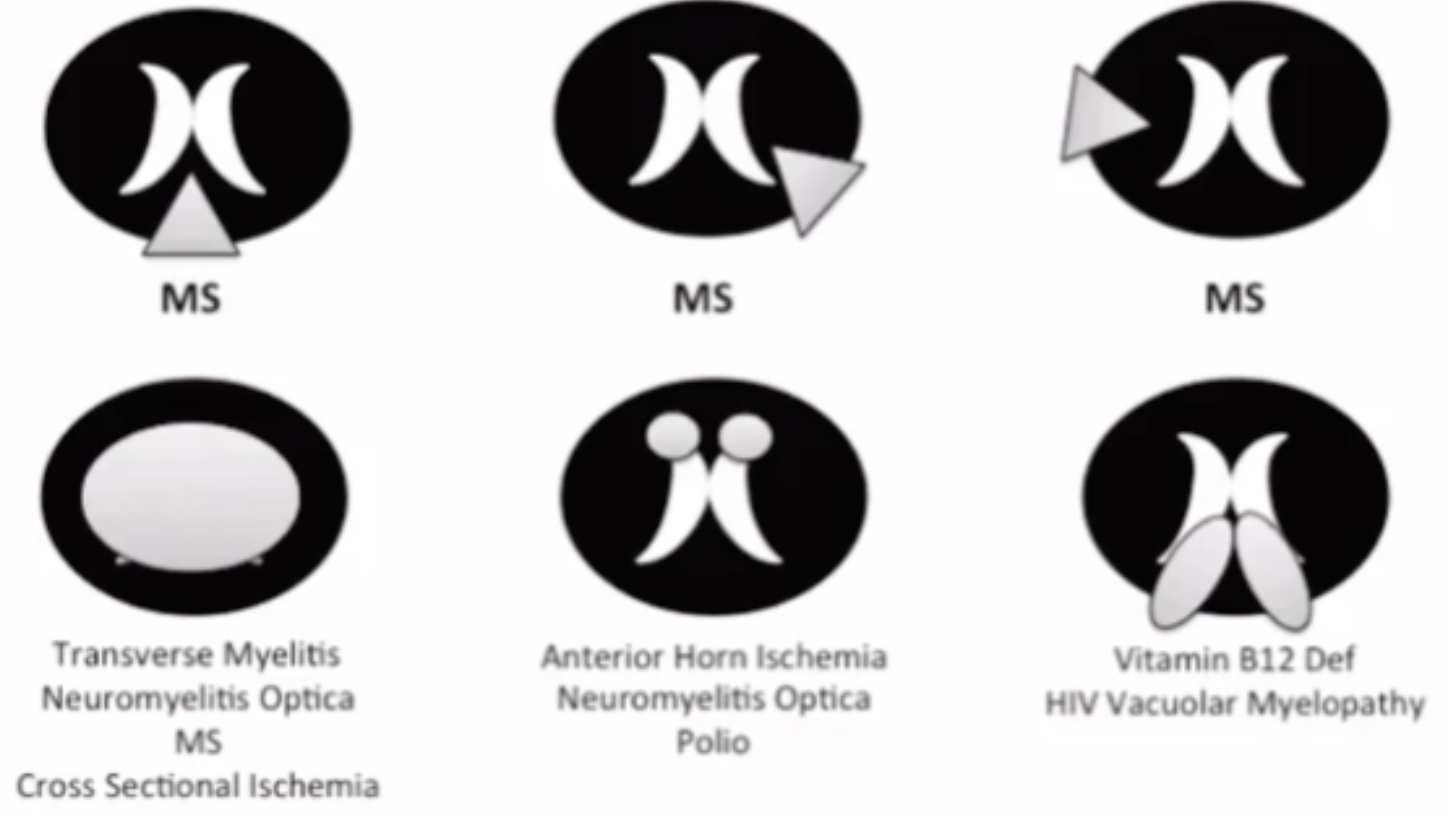
Spinal Cord Ischemia/Infarction
Double barrell sign/snake eye sign
Symmetric T2 hyperintense appearance of central gray matter in spinal cord
Look at T1 —> if low signal then means these lesions are basically holes and not just edema, if they were edema could also be things like transverse myelitis, paraneoplastic myelopathy
Look for associated infarction of the vertebral bodies
Spinal AVF
Flow voids around the cord
Looks like bunch of little dots
Foix-Alajouanine Syndrome
Progressive myelopathy from chronically increased venous hypertension from a spinal dural AVF
Coup de Poignard Michon
Catastrophic subarachnoid hemorrhage caused by a spinal AVF
Sudden onset excruciating back pain (thunderclap headache for your back)
Like you got stabbed in back (poignard = dagger)
Chronic
T1 - return of fatty marrow signal
T2/STIR - no edema
Minimal to no enhancement
Endplate sclerosis
CIDP
Basically chronic GBS
GBS improves in 8 weeks, CIDP does not
Thickened, enhancing nerve roots
Resemble onion bulbs
Really just looks like a lot of nerve roots because they’re so thick
Charcot-marie tooth also looks like this
Arachnoiditis
Clumped nerve roots
Empty central thecal sac with peripheralization of the nerve roots
Enhancement of nerve roots is normal for up to 6 weeks post-op
>6 weeks = abnormal
Very early/Occult
Hours-days or before visible height loss
Edema occurs before height loss
Band edema + T1 hypointensity
Minimal to no visible height loss
Compression Fractures
Compression Fractures
Endplate irregularities with signal changes as below
Note: When a kyphoplasty is performed for a compression fracture the adjacent levels are at increased risk for getting a compression fracture because when you strengthen the previously fucked up level more of the axial load gets placed on the level adjacent to the previously crushed vertebral body which predisposes it to more trauma
So when reading a post-op study after a kyphoplasty you really need to look at the levels above and below the kypho to make sure there is not a new subtle compression fracture
Acute
Hours-2 weeks
T2/STIR hyperintense + T1 hypointensity, signal usually diffuse rather than linear band like
Diffuse internal enhancement
Endplates irregular and sharp
Subacute
Patchy T1 since fat is retruning
Persistent but decreasing T2/STIR signal
Less intense, heterogenous enhancment
Band like edema maybe again
References:
Case courtesy of David Cuete, Radiopaedia.org, rID: 24864 (Bertolotti syndrome)