Shoulder MRI
Tendons
Critical zone = basically area just proximal to the tendon’s attachment on bone, less vascularity here so higher risk of injury
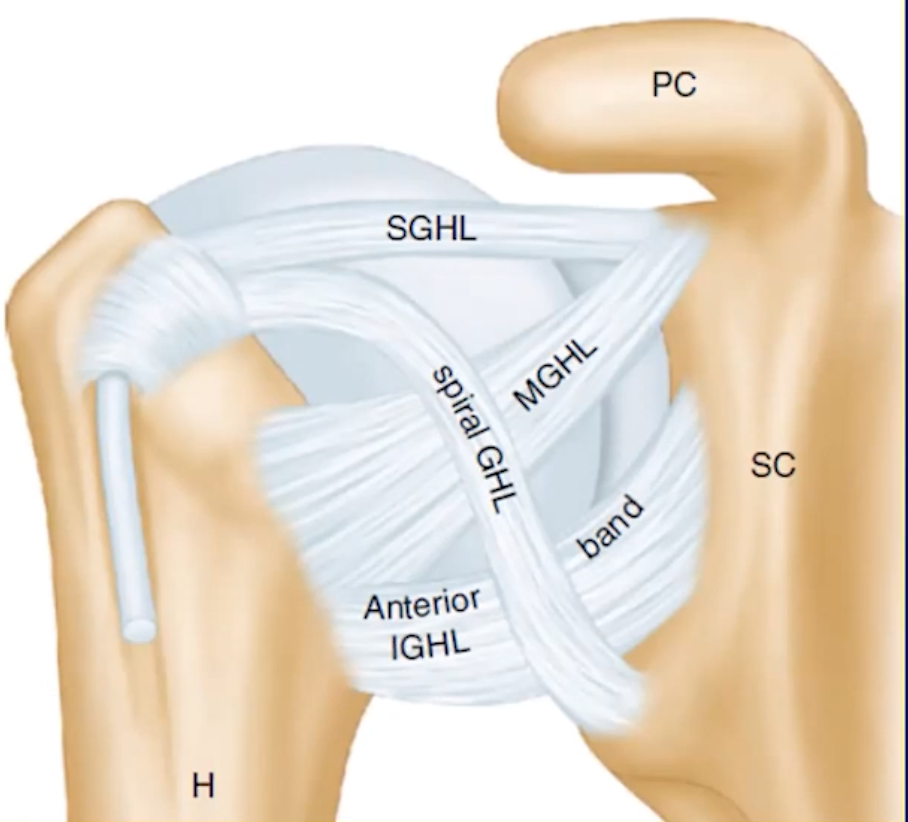
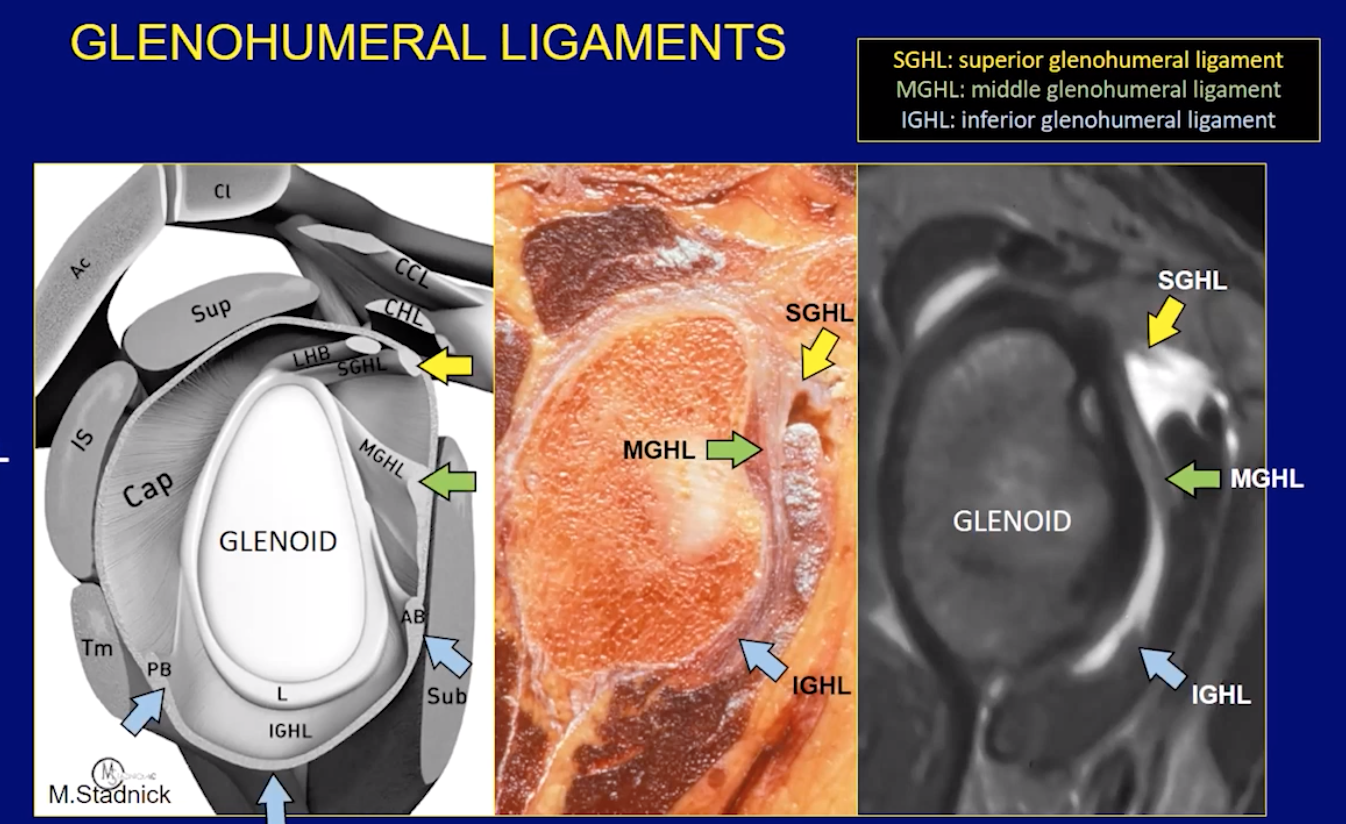
Major ligaments
Superior, middle and inferior glenohumeral ligaments
Passive Stabilizers of the glenohumeral joint
SGHL
Inserts near lesser tubercle of humerus
Acromio-humeral interval
>12 mm: shoulder dislocation, inferior subluxation
8-12 mm : normal
6-7 mm: thinning of supraspinatus tendon
<6 mm: supraspinatus tear
Bony Bankart lesion
> 25% glenoid surface bone loss is an indication for surgery
should comment on this in report
Labral Variants
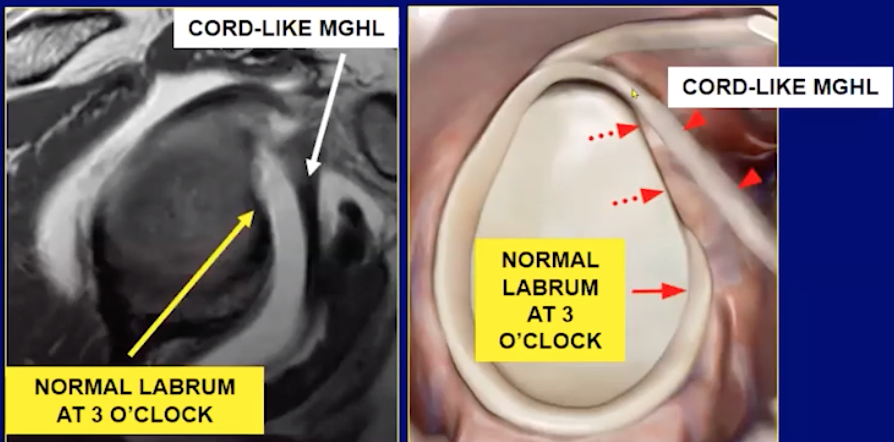
Buford Complex
Absent anterior-superior labrum + cord like MGHL
Labral Pathology
Superior labral pathology is commonly assoicated with paralabral cyst formation
Depending on cyst size and location can fuck up surrounding shit
Can compress the suprascapular nerve (supplies supraspinatus or infraspinatus muscles)
Spinoglenoid notch will affect infraspinatus alone
SLAP 1
Adhesive Capsulitis
Capsule thickening and edema
IGHL ligament thickening, typically >4 mm
Soft tissue thickening of the rotator cuff interval
Loss of fat here
T2 hyperintense & enhance
Coracohumeral ligament thickening (> 4mm)
Decreased capsular volume
Axillary recess appears small
Basically no fluid around shoulder and the tissues adhere close to the humerus bone
Unless concurrent other shit the rotator cuff itself and labrum are normal
References:
Anatomy
MGHL
Find subscapularis and move slightly toward the joint
MGHL runs alongside the subscapularis tendon before inserting at the glenoid
Inserts at lesser tubercle of humerus
Pathology
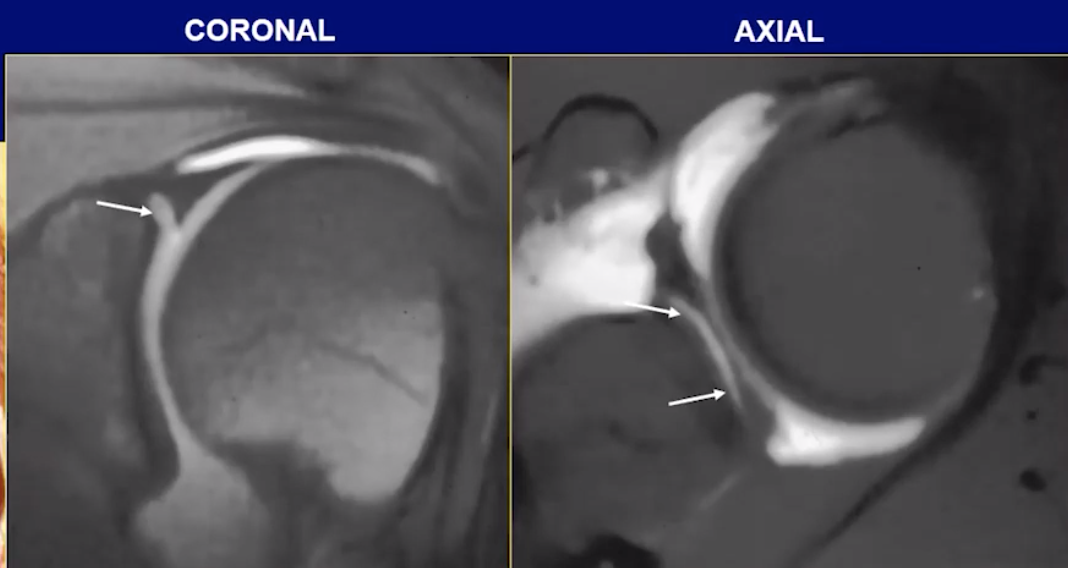
IGHL
Basically forms the anterior and posterior borders of the capsule
Has anterior and posterior fibers
Look for where fluid in the joint ends and trace the black lines to the humerus and glenoid and that is likely your IGHL
Located just inferior to the MGHL anteriorly and is much thicker anteriorly
Tendon injury
Location of the injury
Need to think of the tendon as having 3 layers, like an oreo
Bursal surface - the surface that is not touching and opposite the bone basically, usually superior
From compression from bursa typically
Intra-substance - within the fibers themselves, basically the middle of the tendon and not touching either of the other surfaces
Articular surface - the surface that is touching the bone basically
Most common, from over use (throwers)
Degree of injury
High grade = > 50% of tendon involved
Low grade = < 50% of tendon involved
Grading
Grade 1
Strain/tendinopathy
Fibers are intact with midly increased STIR signal
Grade 2
Partial thickness tearing
Fibers disrupted but some still intact
Fluid signal extending through the tendon
May seen tendon thinning, partial irregularity
Grade 3
Full thickness tearing
Additional relevant items to include
Muscle atrophy/fatty atrophy? —> helps with chronicity
Goutallier classification
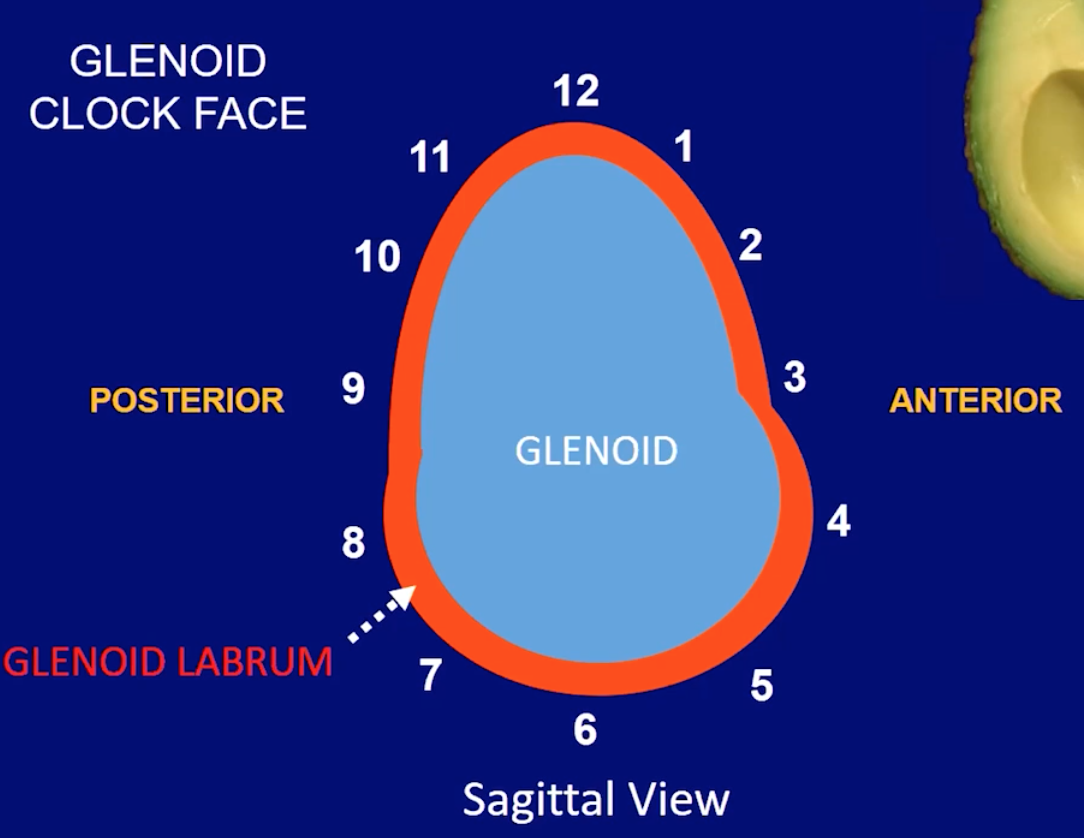
Labrum
General
Use clock position to describe location of shit
12 is superior
3 is anterior
6 is inferior
9 is posterior
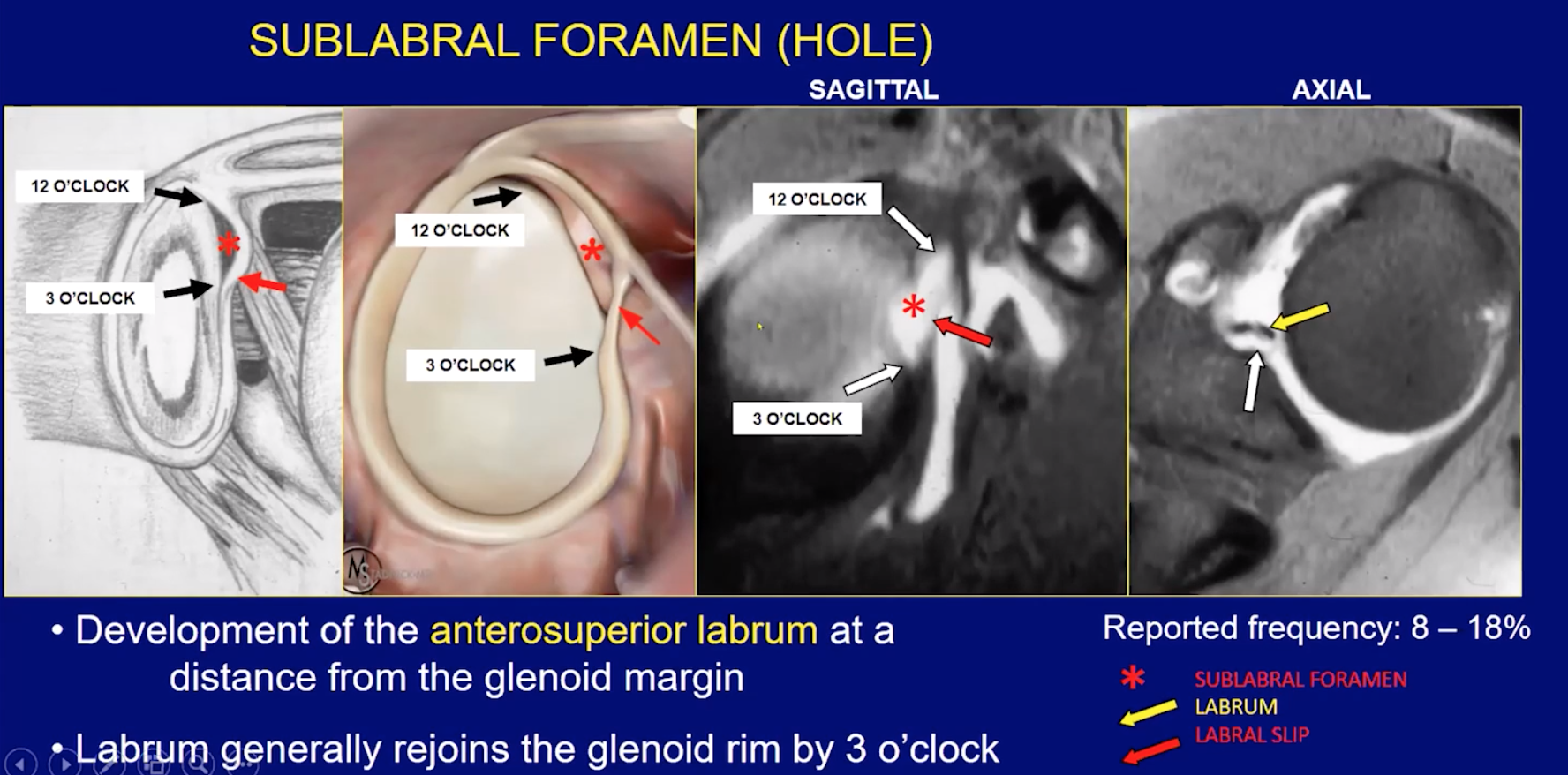
Many variants which usually occur in the 11 to 3 o’clock rang
Below 3 o’clock the labrum should be tightly fixed to the glenoid so if you see it pulled off, or signal that is abnormal
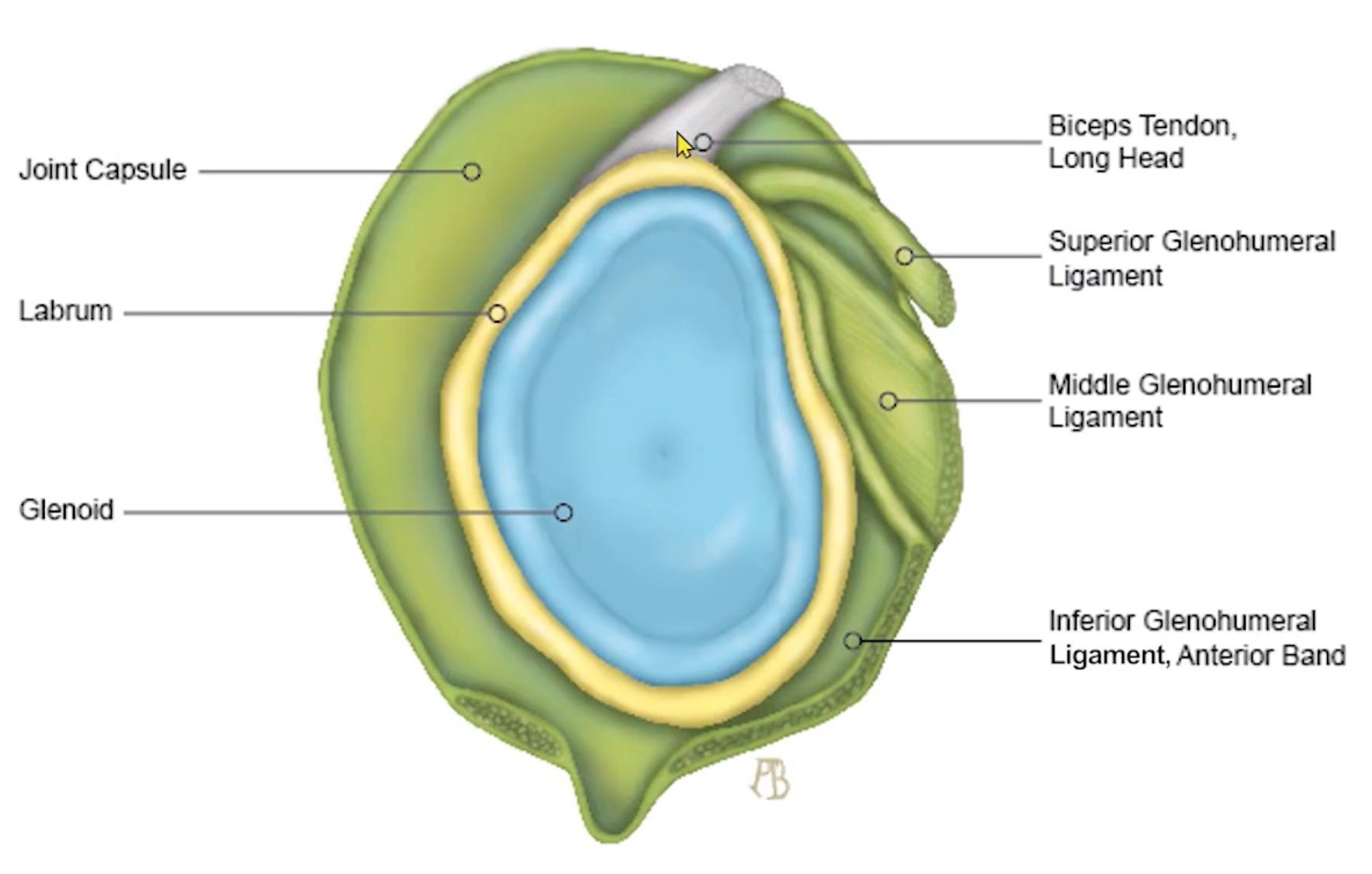
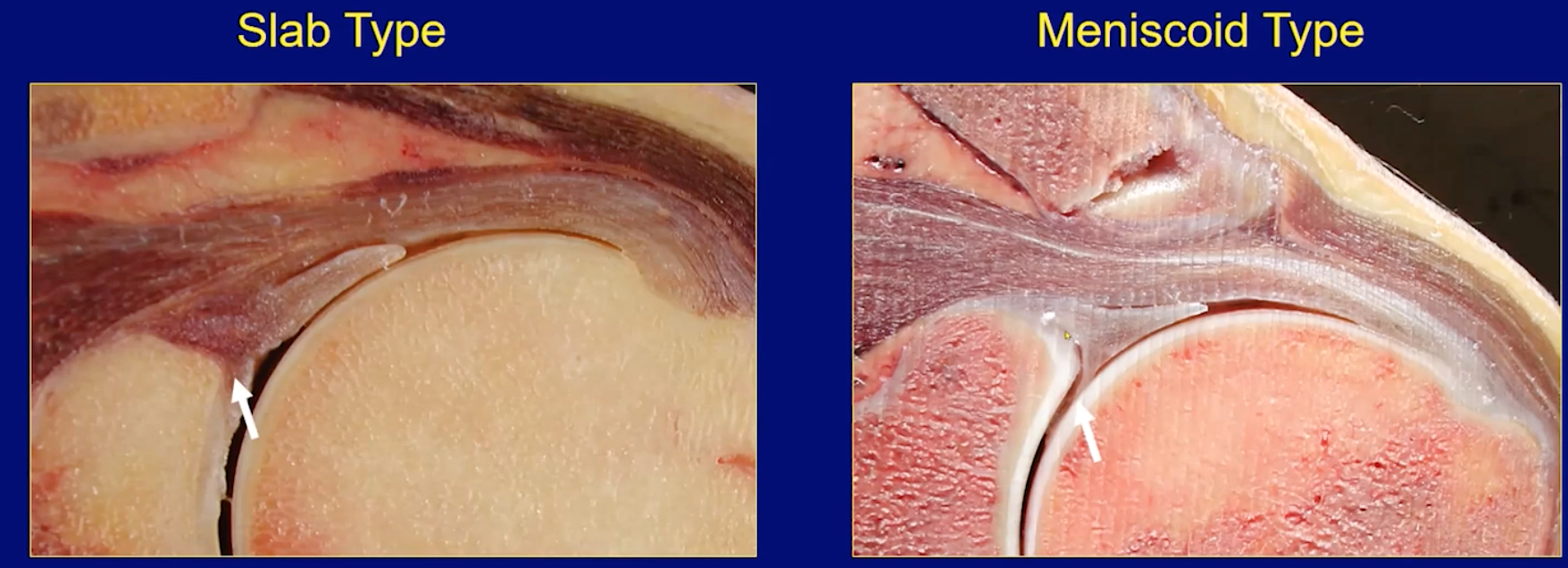
Biceps Tendon (LHBT)
Commonly attaches to posterior superior aspect of glenoid
Commonly has two attachments, one to the glenoid and one to the labrum
Two major variants
Slab type - close approximation of tendon and labrum with little space
Meniscoid type - space between labrum and tendon
Ligaments
Superior glenohumeral ligament
Located along under-surface of biceps tendon (helps stabilize the intra-articular portion of LHBT)
Most commonly arises from anterior-superior labrum
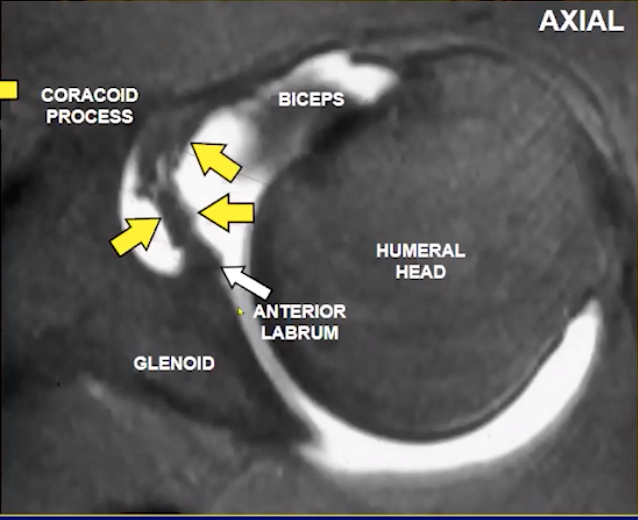
Middle glenohumeral ligament
Close to subscapularis
Inferior glenohumeral ligament
These are all intracapsular ligaments
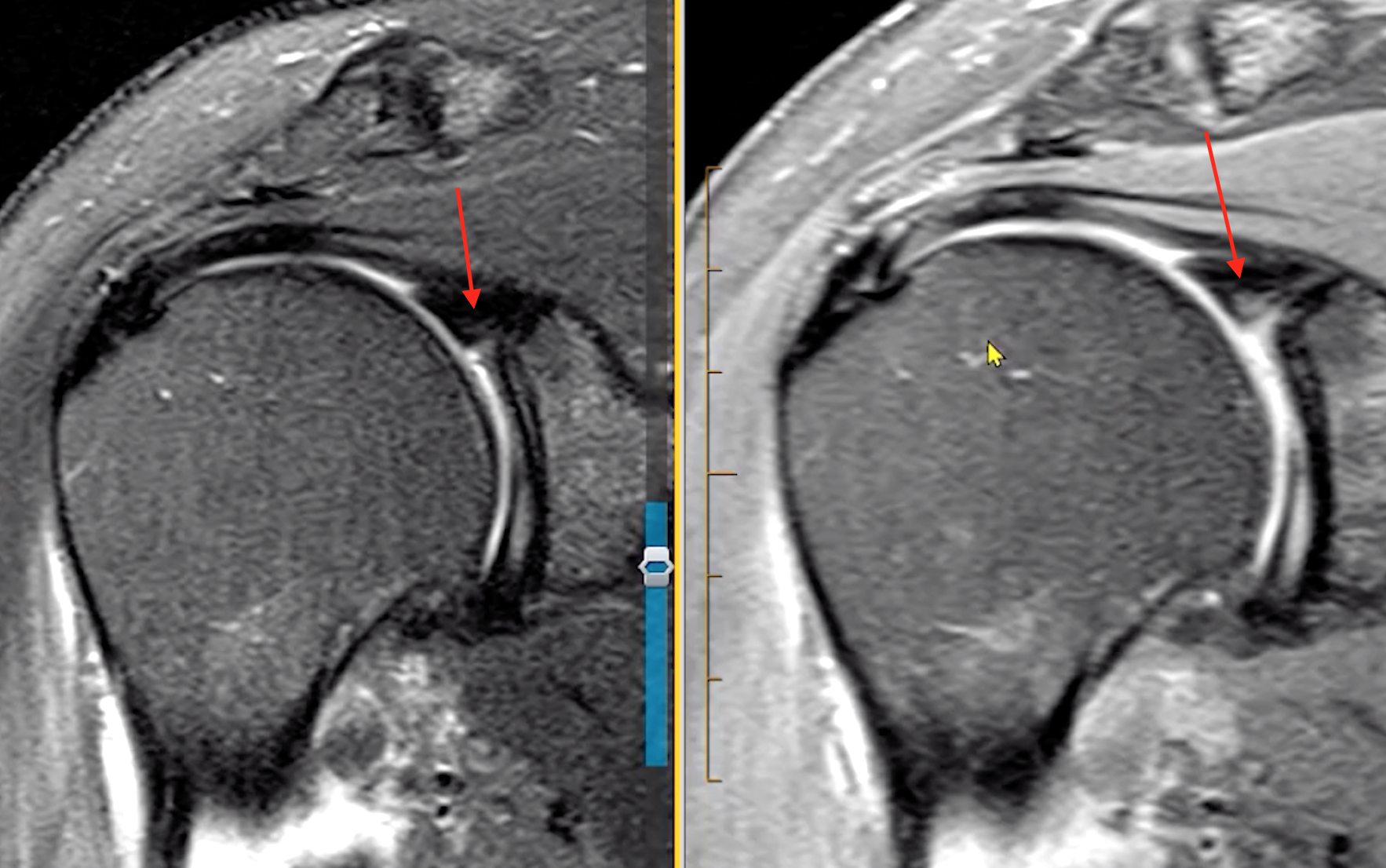
Superior glenohumeral ligament
Image showing its attachment from the anterior superoir labrum
Then swings toward the coracoid process where its joints the coracohumeral ligament
Then continues to its attachment near the bicipital groove
There are other less common morphology like common origin with MGHL
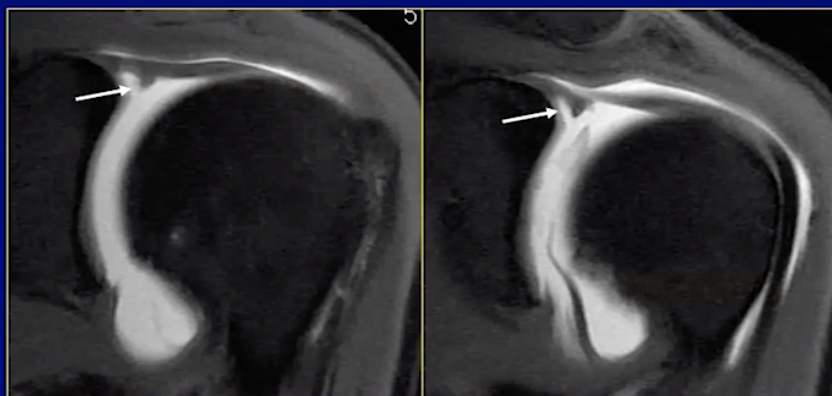
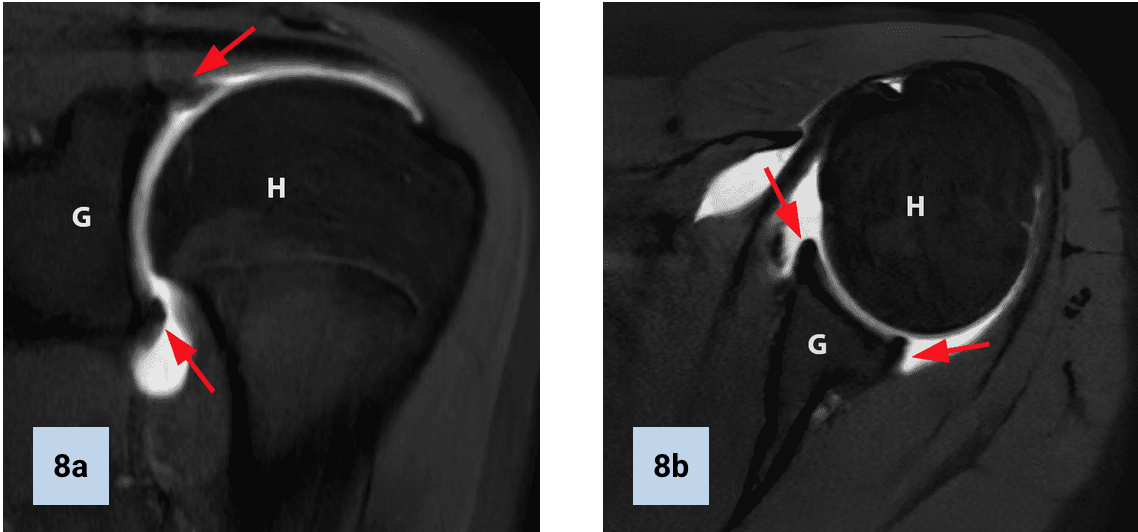
Sublabral sulcus/recess
Space between the labrum & articular cartilage of the glenoid
Smooth borders
Should not extend posterior to biceps anchor
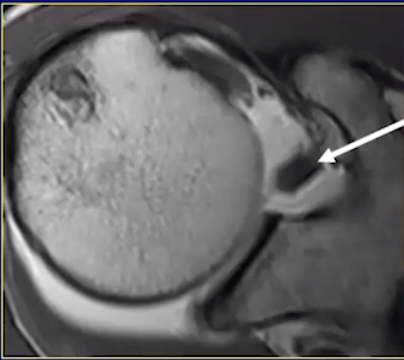
Normal Labrum
Bucket Handle SLAP Tear of Labrum

Middle glenohumeral ligament
Arises superiorly from the glenoid (typically base of labrum), in close proximity to the coracohumeral ligament
Descends to the humerus where it becomes in close proximity to the subscapularis tendon

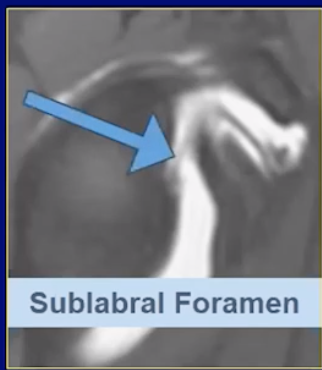
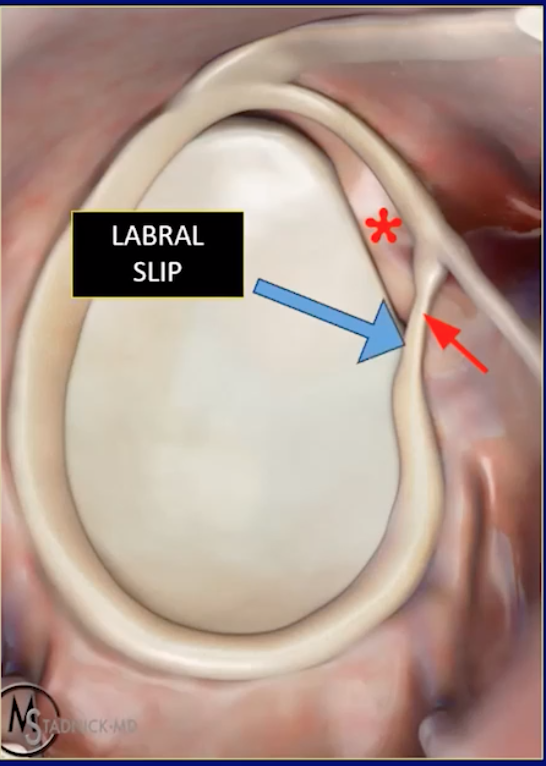
Labral Foramen
Snyder Classification of Labral Tears
SLAP 1
A degenerative type tear
Fraying of the undersurface of the labrum
Depth less than 50%
SLAP 2
Basically SLAP 1 that is deeper and more focal
Depth > 50%
SLAP 3
Essentially bucket handle tear for the labrum
Basically tear in labrum where there is labrum on both sides like a cookie
SLAP 4
Biceps involved
SLAP 2