Rectal MR
General
Usually get a T2 fast spin or turbo spine echo and a T2 single shot spin echo
The fast spin/turbo spin is the one which looks nice and can actually see shit, higher signal to noise - use this one
The single shot is faster but ass
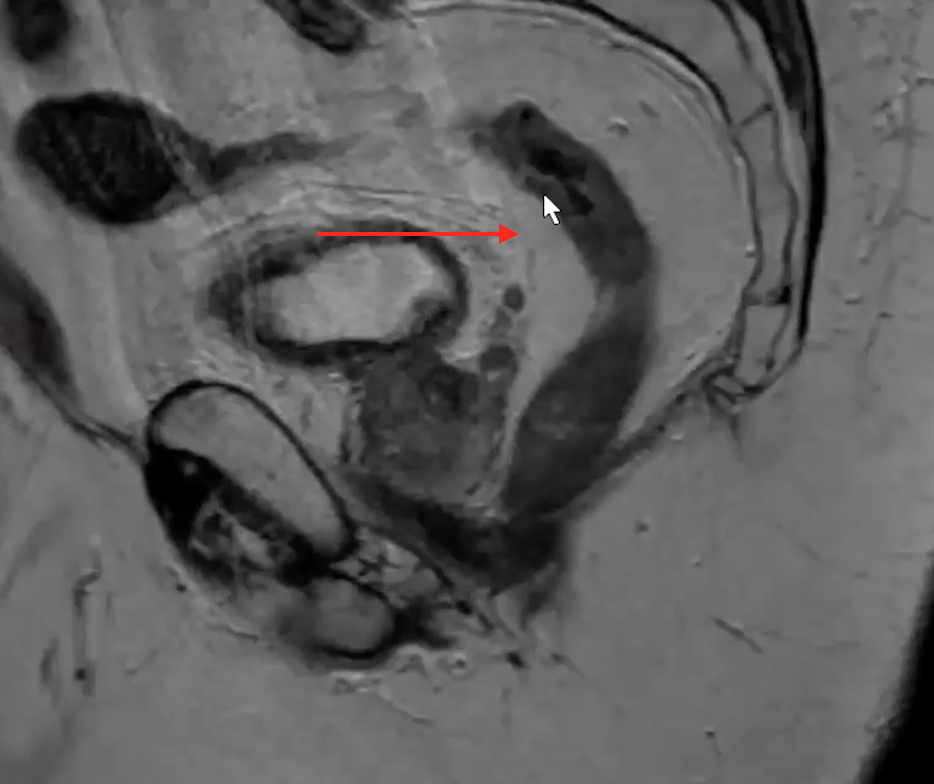
Will get an oblique-axial view which is used to look down the lumen of the rectum
Will get an oblique coronal view which is used to look down the lumen of the distal rectum and anus
Glucagon sometimes give to stop peristalsis in the bowel - better images
Rectum considered distal portion of bowel and is the distal most 15 cm of bowel ending at the anal verge
Superior 5 cm = Upper rectum
Middle 5 cm = middle rectum
Lower 5 cm = lower rectum
Below the peritoneal reflection (low rectum) is completely extra-peritoneal
Superior to the peritoneal reflection the mid and superior anterior rectum is intra-peritoneal
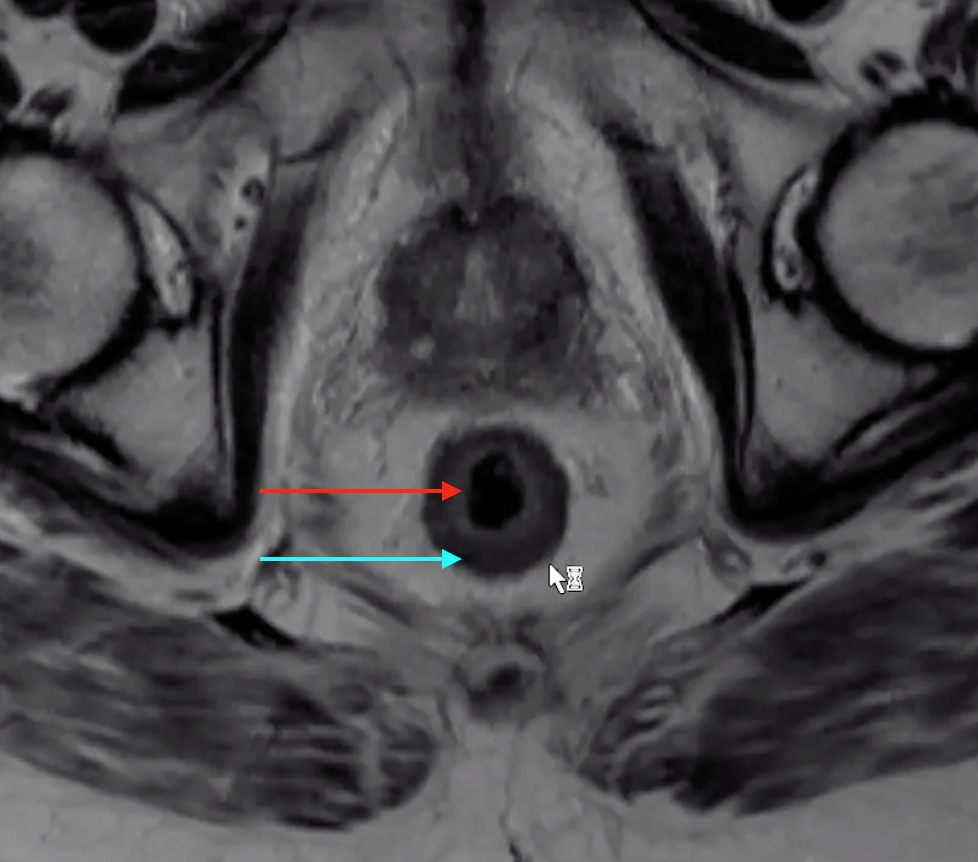
Anal Sphincters
External sphincter
Darker external line (blue)
Extends slightly lower than internal
Internal sphincter
The brighter/white internal stuff (red)
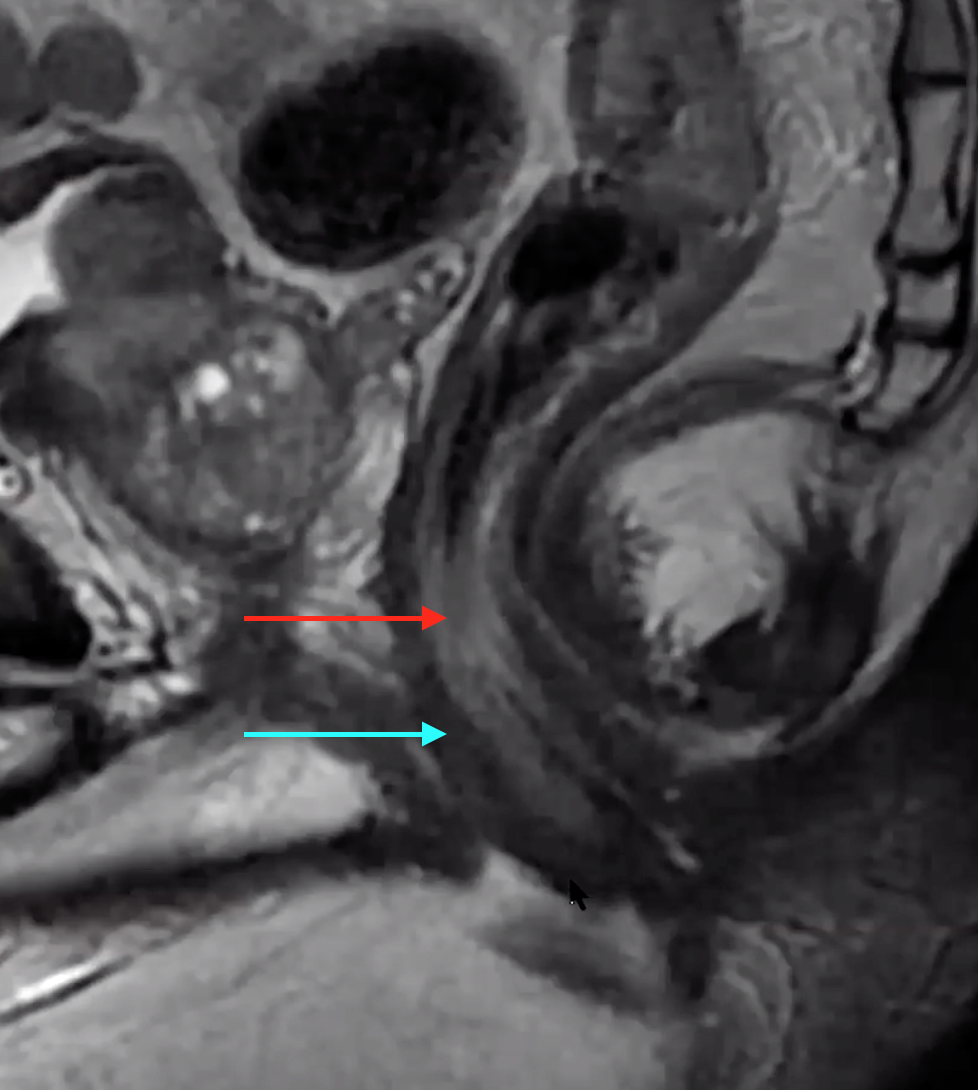
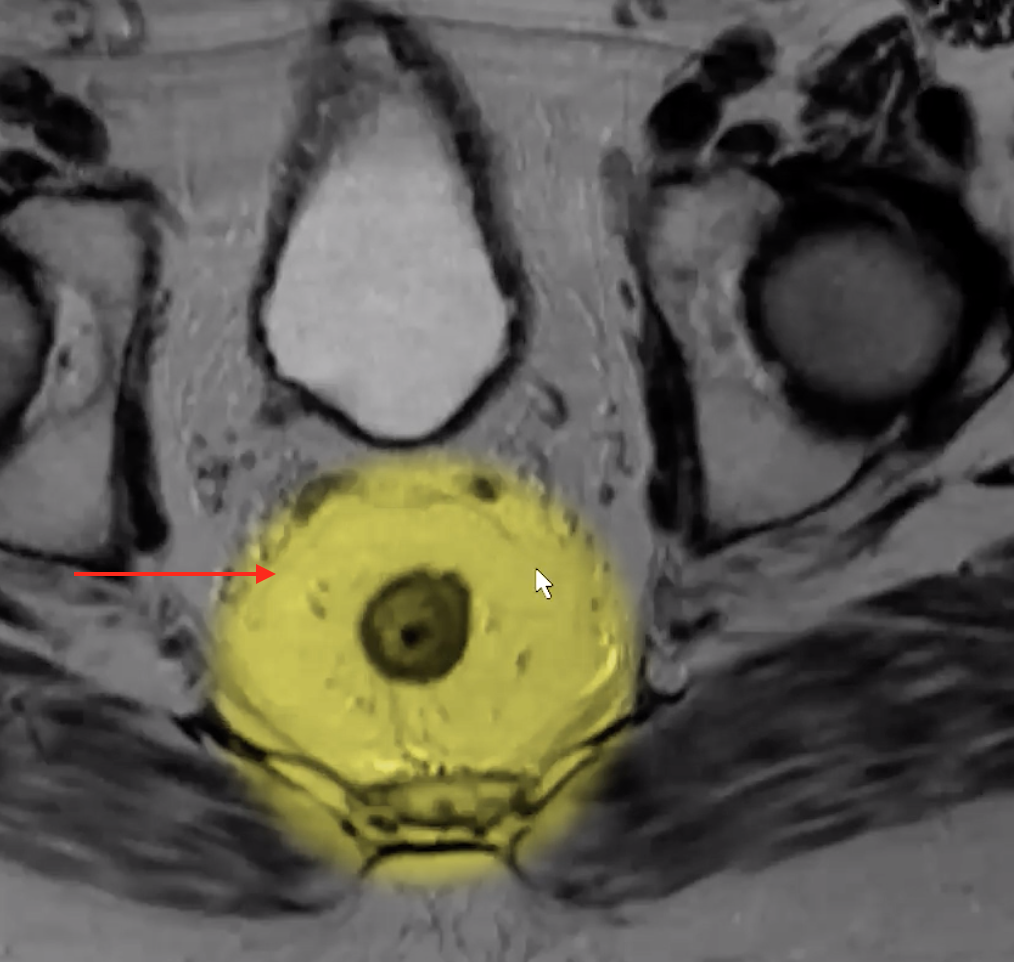
Mesorectal Fascia
Thin dark line surrounding the mesorectal fat
Like a tear drop shape
Superiorly ends at the level of the recto-sigmoid junction where it blends into the sigmoid mesentery
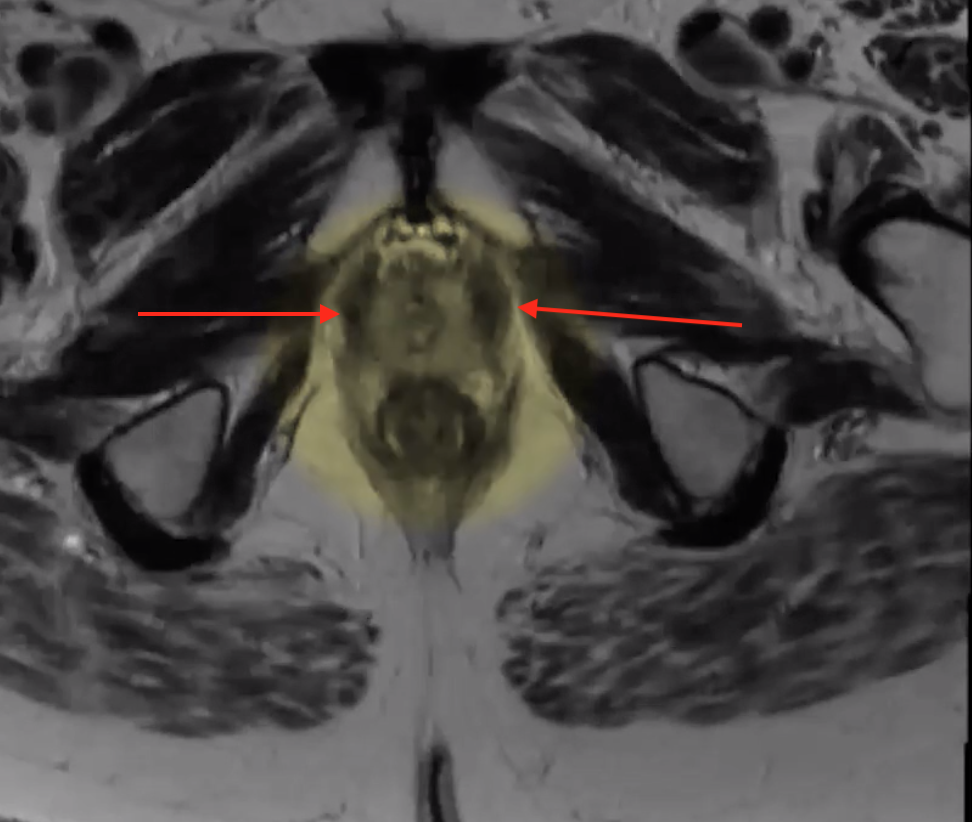
Inferiorly blends into the puborectalis and levator muscles
Wide in the center
Puborectalis
U shaped muscle on either side
Interpretation
Staging
Confined to the submucosa = T1
Confined to involves muuscularis but not beyond it = T2
NOTE: On imaging we cannot differentiate between T1 & T2 so they are grouped together
Extends beyond muscularis and into the mesorectal fascia = T3
IF you see T3 you need to state how far the tumor extends from the border of the muscularis to its fartherst part into the mesorectal fascia
T3a = extension < 1mm into MRF
Treated as a T1/T2 cancer with resection
T3b = extension 1-5 mm into MRF
T3c = extension 5-15 mm into MRF
T3d = extension > 15 mm into MRF
If extension is >5mm, 50% 5 year survival
If less >85% survival at 5 years
Extends beyond muscularis into mesorectal fascia AND invades adjacent structures = T4
Common adjacent structures
Prostate
Sidewall muscles
T3 is the big divide
Once it is T3 then they have to get neoadjuvant chemo prior to surgery
If T1/2 I think they can just go straight to surgery
References:
Anatomy
Rectal Wall
Muscularis
Darker external ring (blue)
Mucosa
The brighter/white internal stuff (red)
Made up of the mucosa and submucosa but these cannot be differentiated on imaged they run together
Peritoneal Reflection
Thin dark line that has a bend in it anterior to the rectum
Iliococcygeous
