Peritoneum & Mesentery
General & Anatomy
Peritoneum is membrane that covers abdominal cavity and is lined by mesothelium
Falciform ligament
Separates the right and left subphrenic spaces
Connects peritoneum to diaphragm
Remnant of ligamentum teres (umbilical vein)
Bare area of liver
Posterior and right aspect of liver that is not covered by peritoneum
Lesser Sac
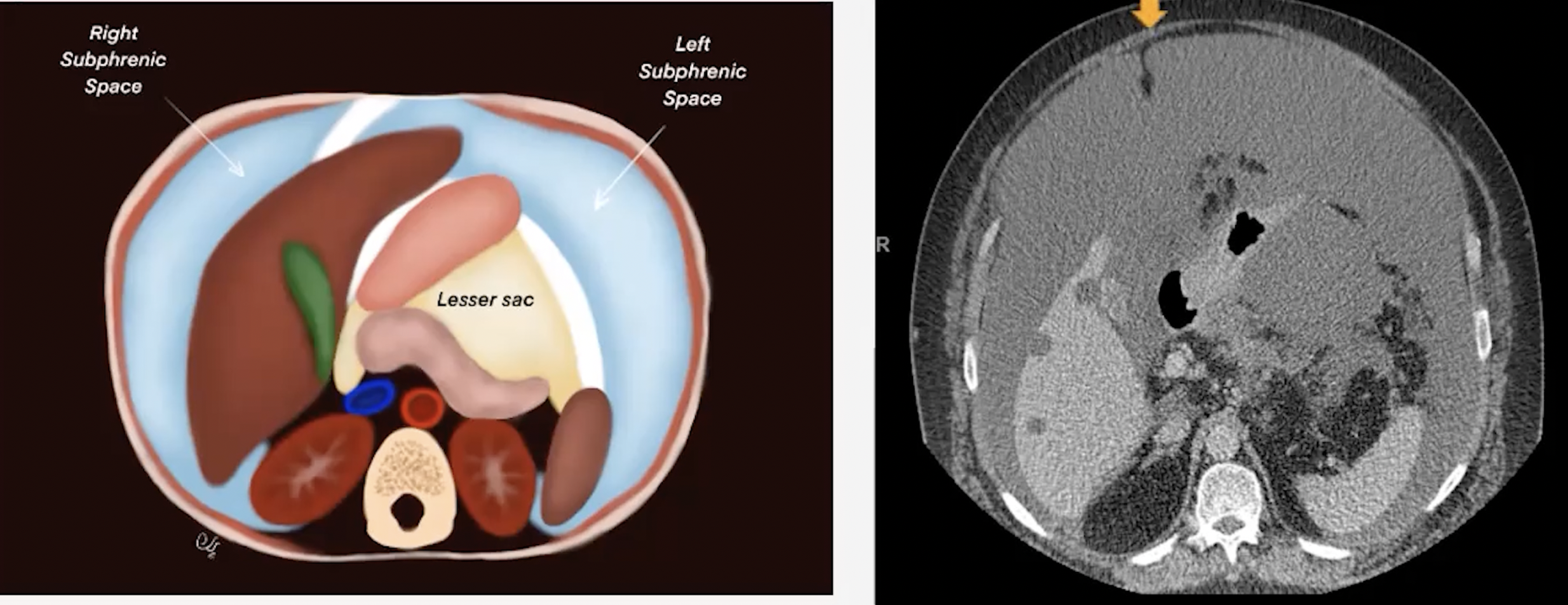
Free Air
Air should rise so if you see free air that is anti-dependent portion can give you clue as to what organ it is from
Peritonitis
Infection
Hemorrhage
Findings
Basically thickening and enhancement of the peritoneal lining, use image above to see the lining as when there is fluid it really just looks like a thickened wall of the abscess but will be in the location of the peritoneal wall, not the abdominal wall!
Peritoneal Malignnacy
Rare & hard to differentiate from mets
Mesothelioma
Associated with prior asbestos exposure
Dry type
Pain with palpabale abdominal masses
Wet type
Multiple nodules with ascites
Mixed type
Carcinomatosis (basically mets to peritoneum), most commonly from
Ovarian
GI
Gallbladder
Pancreas
Peritoneal Infection
May mimic carcinomatosis
TB
Typically from reactivation than from primary
Encapsulating Peritoneal Sclerosis
Fibrocollagenous cocoon like encapsulation of the small bowel
Associations
TB
Dialysis
VP shunts
Non-specific shit
Thickend peritoneum
Fixed bowel loops, thickened bowel, bowel obstruction
Peritoneal or mural calcifications - key
Loculated ascites
Mesentery
Double later of peritoneum that surrounds the organs and keeps them in place
Internal hernias
Associated with rapid weight loss - look for weight loss surgeries and shit
Swirling of vessels (more than 360 deg), likely with vessel caliber changes
Pinching or odd angulations of the bowel (90 deg angle would be abnormal)
Signs of ischemia
Tumors
Desmoid
Does not metastasize and considered benign
Locally aggressive and can engulf adjacent shit
Must have complete resection in surgery or they will occur
In mesentery, retroperitoneum or abdominal wall muscles
Associated with FAP
NOTE: Desmoid will be negative on PET where as colon cancer mets would be positive
Looks like soft tissue mass
Carcinoid
Calcifications
Typically soft tissue density mass
Usually a metastatic finding
Look for the primary mass —> look at the bowel wall , may be subtle
Liposarcoma or other sarcoma
Lymphoma
Typically with misty mesentery appearance but with fucked up nodes
Infection - Abscess
Typically from adjacent process (pancreatitis, appendicitis etc.)
Misty Mesentery (Hazy appearance of the mesentery)
Increased density of the mesentery without displacement of the vessel
May have associated nodes
Typically in small bowel mesentery
Causes
Panniculitis
Edema
Hemorrhage
Neoplastic
Creeping fat of the mesentery
When fat wall of an inflammatory process
Most commonly associated with Crohns
Mesenteric Adenitis
Clustered LN
3+ nodes which are 5 mm or more each and are homogenous
No additional cause on imaging (not reactive)
Typically in kids and young adults
References: