Pediatric Pulmonary
Conditions in Premature Babies
Surfactant Deficiency Syndrome (Hyaline membrane disease)
Lucency causing disease
Bronchopulmonary dysplasia
Pulmonary Interstitial Emphysema
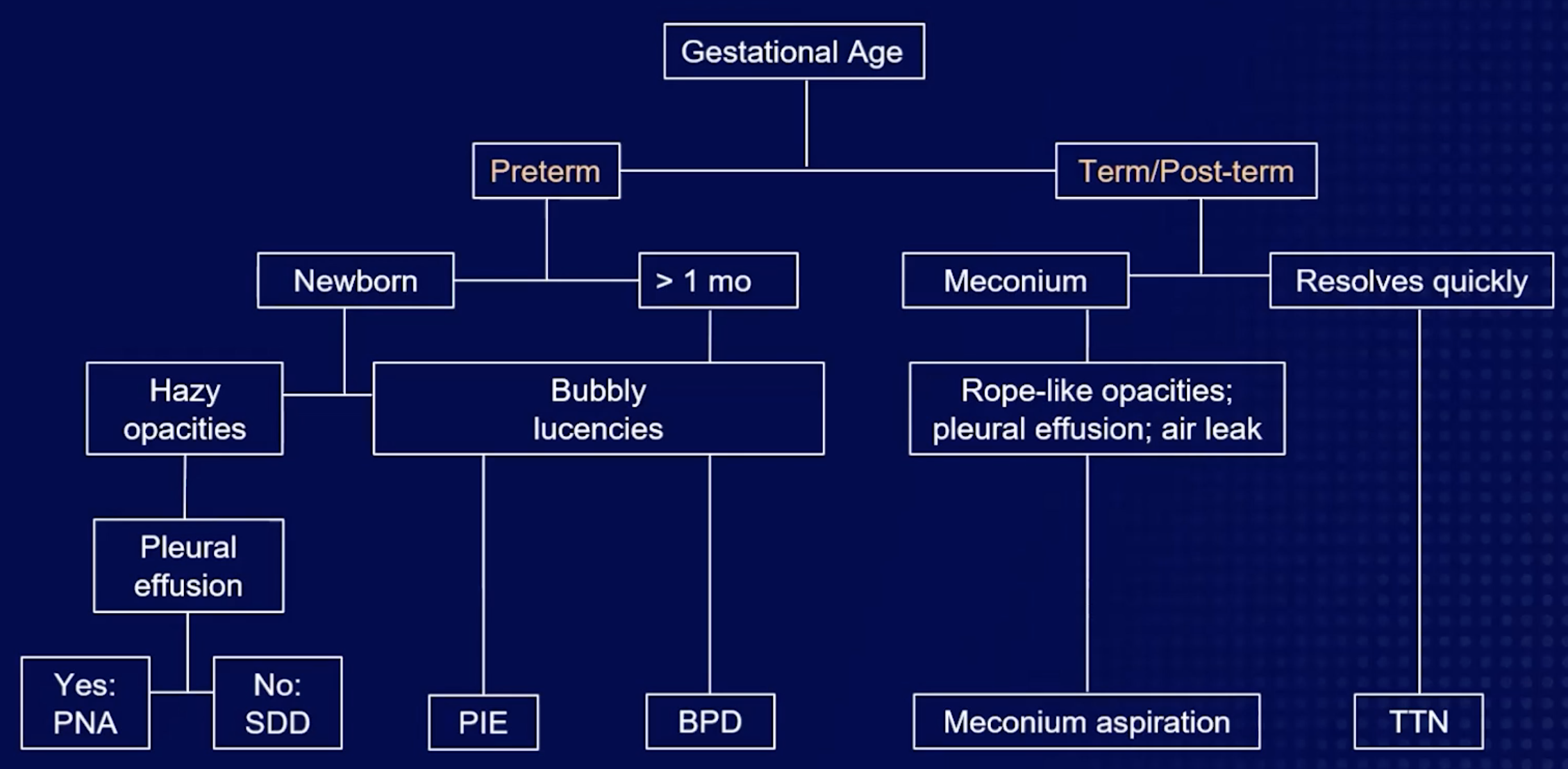
Hyperinflated
Meconium aspiration
Transient tachypnea of newborn
Neonatal pneumonia
Laryngotracheobronchitis (Croup)
Kids 6 months - 3 years old
Steeple sign
Subglottic tracheal edema
Age 6 months -3 years
Barky cough that may improve with exposure to cold air
Parainfluenza virus
Clinical diagnosis
Inflammatory Myelofibroblastic Tumor (IMT)
Most common primary lung mass in kids
Can occur in multiple areas including lung
Imaging appearance varies based on how much fibrotic shit is there
Typically
T1 hypo
T2 hyper
Heterogenous enhancement
Transient Tachypnea of Newborn
Poor clearance of fetal fluid
Associated with c-section delivery
Associated with maternal DM
Seen 6 hours after birth, resolved by 3 days
Non-specific findings similar to pulm edema (diffuse GGO)
Normal lung volumes

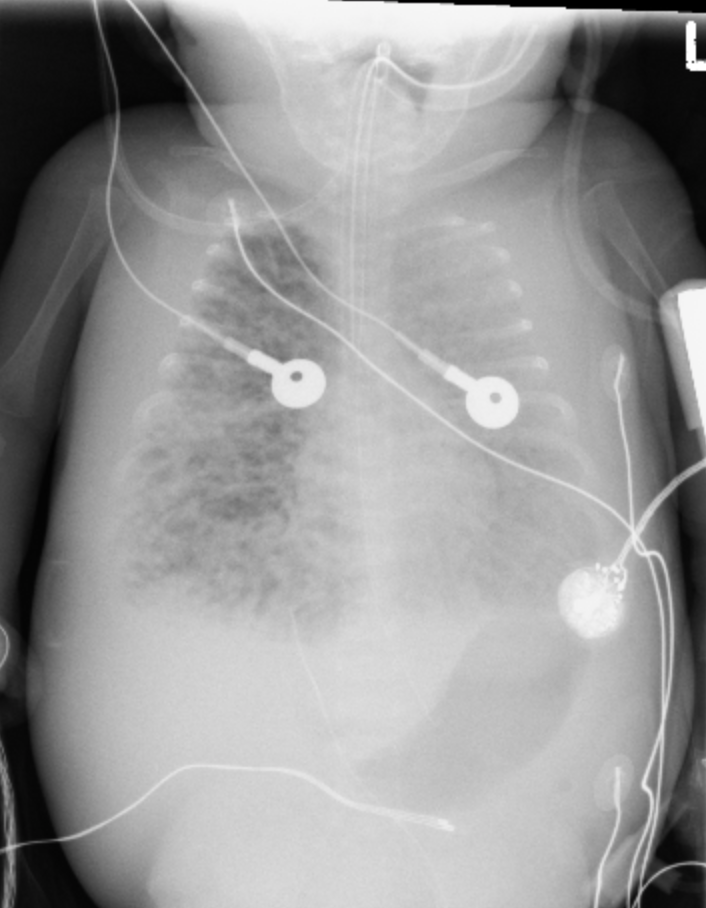
Surfactant Deficiency Syndrome (Neonatal Respiratory Distress Syndrome)
Premature babies
“Hazy” & “Granular” opacities
RF = maternal DM
Immature type 2 pneumocytes cannot make surfactant —> high surface tension
Tx = give surfactant
XR may appear better in hours after administration
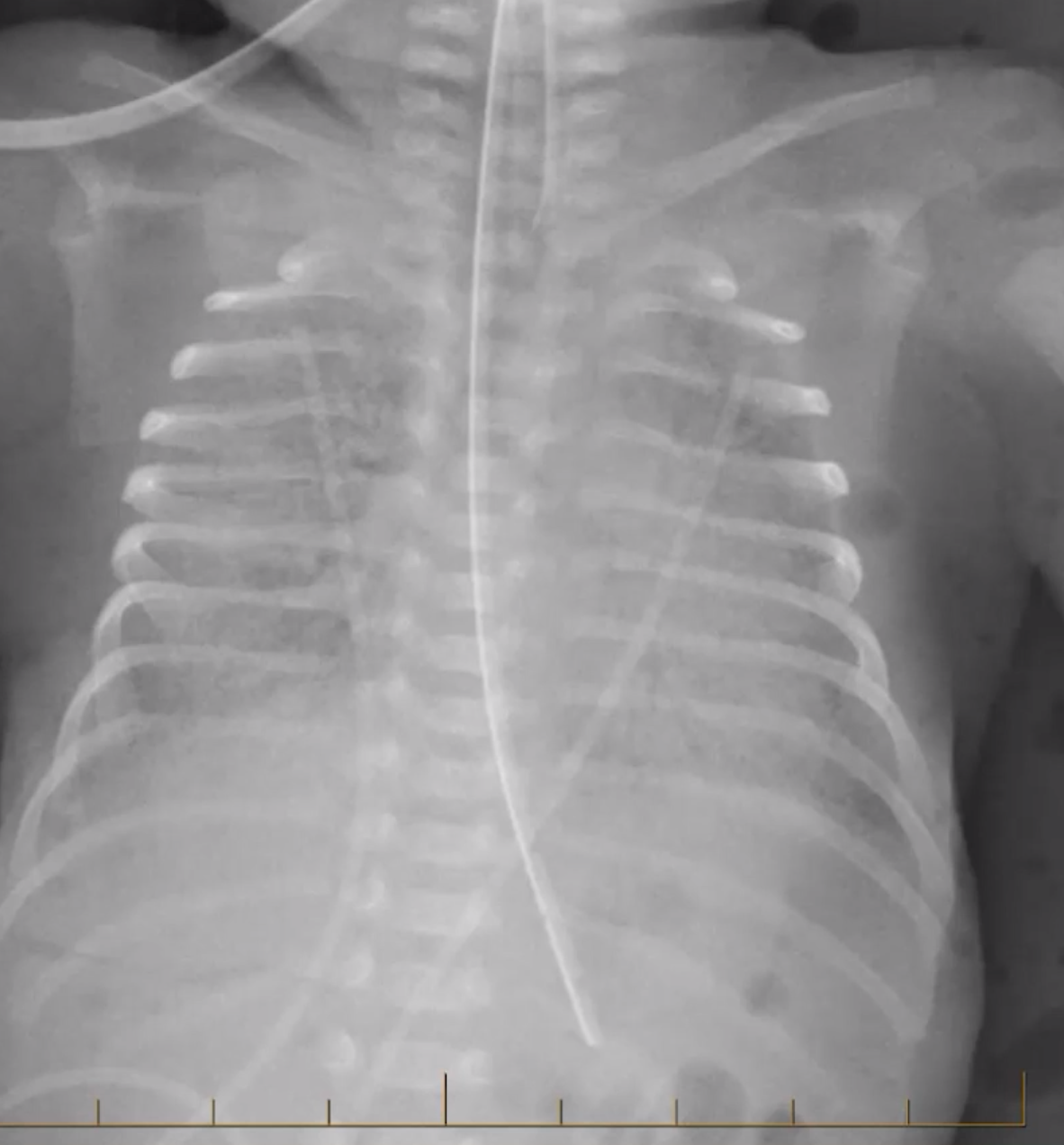
Meconium Aspiration Syndrome
Diffuse bilateral coarse/rope like capacities
If effusion present —> question PNA
Eval for pneumothorax and pneumomediastinum (increased alveolar tension from obstructed airway)
Increased lung volumes (hyperinflated)
then they pop hence the pneumo
Look for hypoxic baby
Look for post-term baby

Congenital Lobar Hyperinflation
Bronchial obstruction
Ball in valve physiology
Hyperexpanded/hyperlucent lobe
Foregut Duplication Cysts
Includes bronchogenic cyst, enteric cyst, neurenteric cyst
Abnormal budding of the ventral foregut at 25-40 days
Bronchogenic Cyst
Pulmonary Interstitial Emphysema
Ventilation in patients with surfactant deficiency causes alveoli to pop and air to escape
Bubbly or linear lucencies
Imaging findings seen at first week of life
<4 weeks old (note BPD >4 weeks old)
Congenital Cystic Adenomatoid Malformation
aka CPAM (Congenital cystic pulmonary airway malformation)
3 Types
Type 1: 1+ 2-10 cm cysts
Type 2: Numerous uniform small cysts
Type 3: Appears solid but is microcysts
Nearly indistinguishable from Pleuropulmonaryblastoma
Congenital Pulmonary Malformations
Bronchial Atresia
Tubular atretic bronchus possibly with mucus plugging
Can also see soft tissue density in area of expected bronchus which is a mucocele
Area of lung supplied by the bronchus that is absent will be hyperlucent
Commonly seen with CPAM & BPS
Bronchogenic Cyst
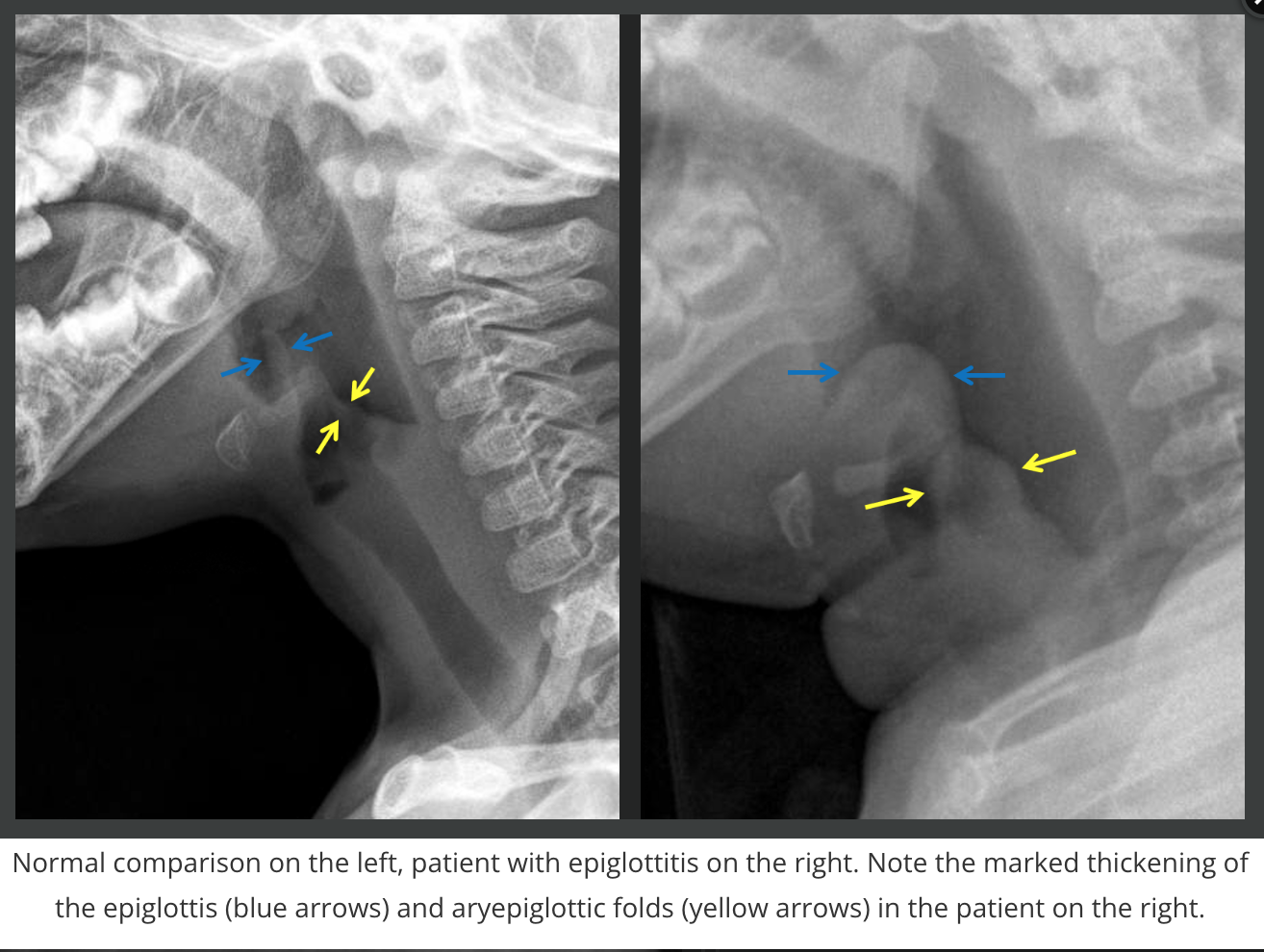
Infectious
Epiglottitis
Kids/teens >3 years old
H-flu
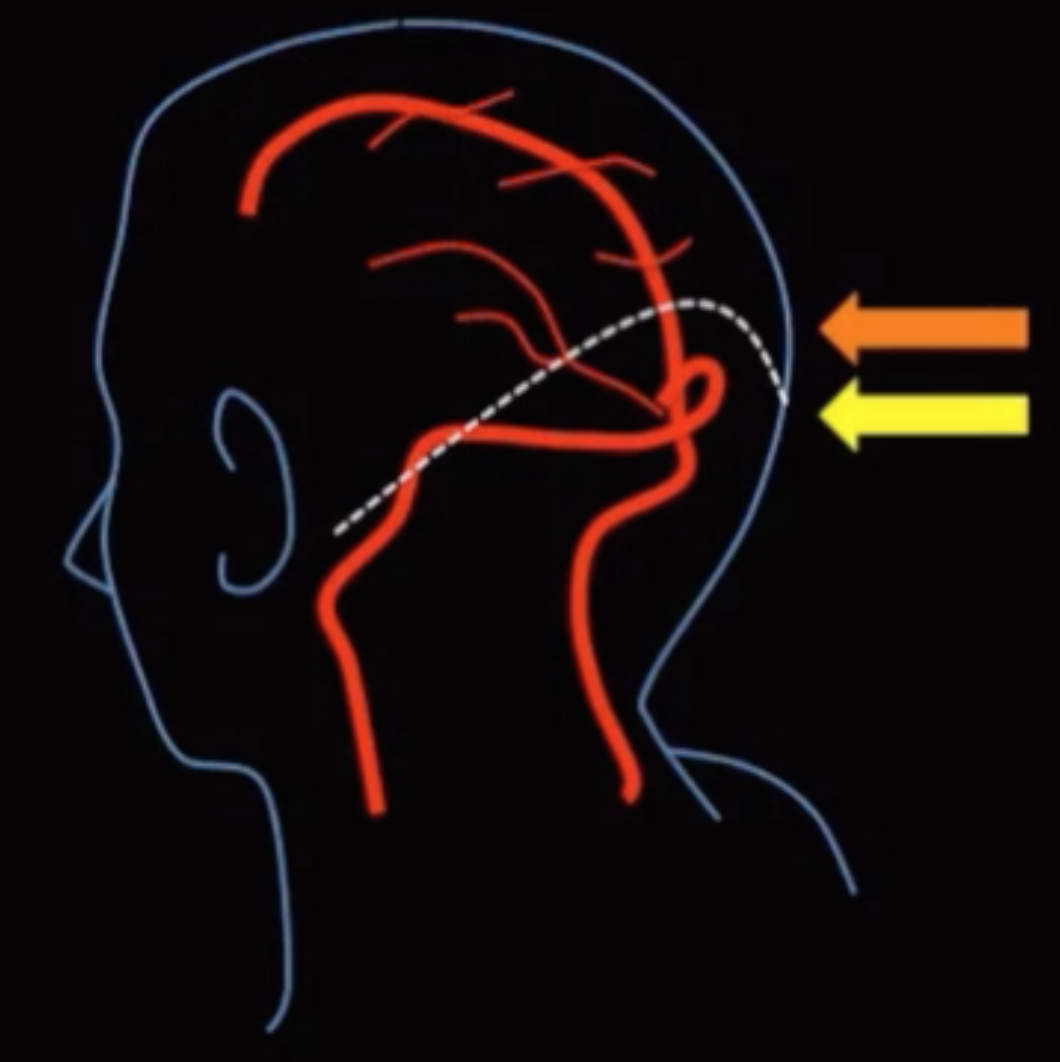
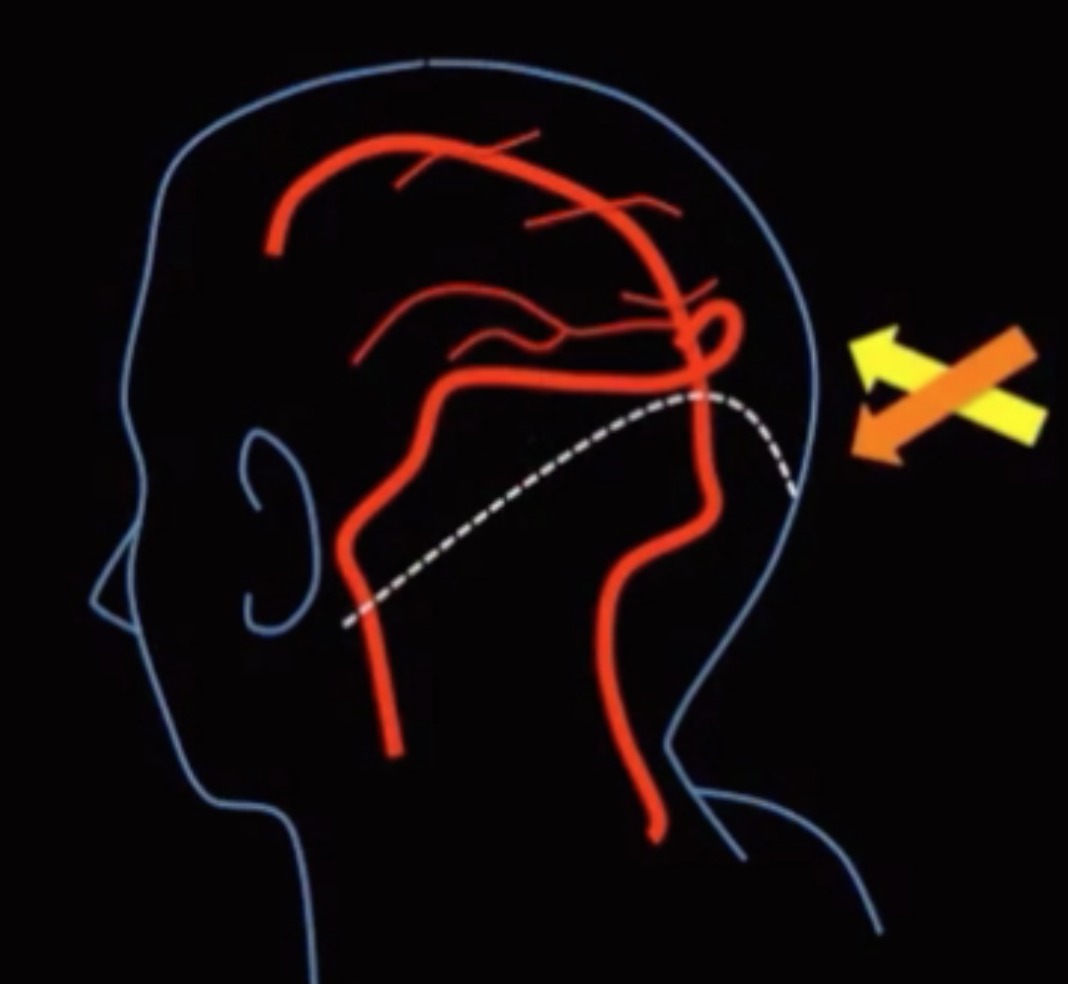
Subglottic Hemangioma
On CXR will look like steeple sign except the walls of the steeple will be asymmetric (because only have the hemangioma on one side)
Associated with torcula-lambdoid inversion
Normally the tip of the lambdoid suture is above confluence of sinuses (top pic), here its the opposite (bottom pic)
Torcula = confluence of sinuses
Lambdoid = suture on back of head
Seen with dandy walker
PHACE Syndrome
Posterior fossa malformations (D-W)
Hemangiomas (subglottic too)
Arterial anomalies
Coarctation of aorta
Eye anomalies
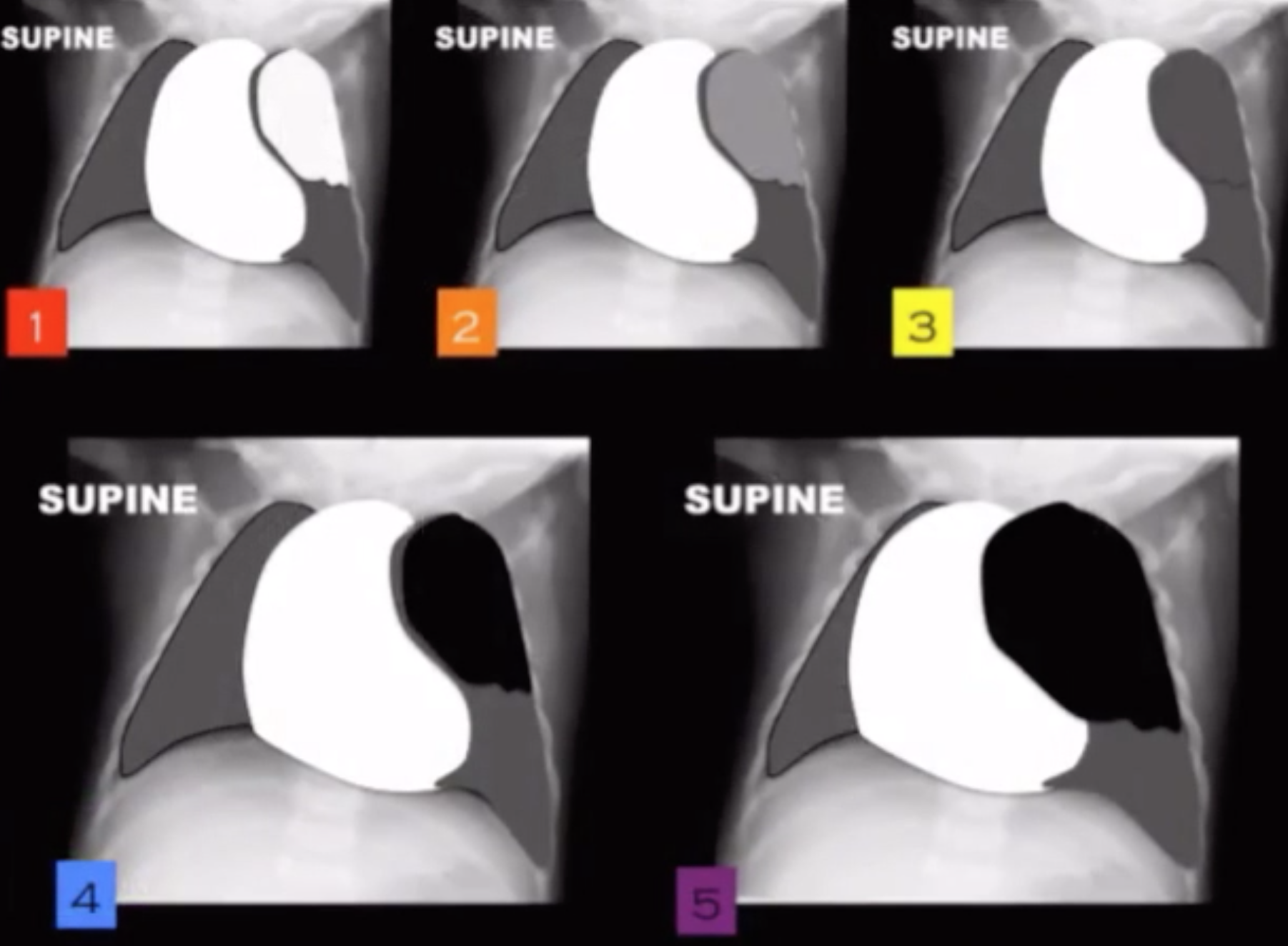
Aspirated Foreign Body
Unilateral lucent lung
Even if you don’t see the aspirated object !
Get lateral decubitus views - if you put the lucent lung on the table and it stays lucent its an inhaled body
Should normally compress under body weight
Note mediastinum will move away from the lucent lung - may be asked Q like this
Retropharyngeal Abscess
Soft tissue thickening of the retropharynx

Conditions in Term/Post-term Babies
Transient Tachypnea of newborn
Meconium aspiration syndrome
Hypoinflated
RDS (no pleural effusions)
Beta-hemolytic pneumonia - betas have low money and low lungs (look for pleural effusions)
Buzz Word vomit
Post-term = mecnonium aspiration
Pre-term = RDS
C-section = TTN
Maternal sedation = TTN
Hypoxic = meconium aspiration

Extra-lobar Sequestration
Less common ~ 25% of cases
Infancy with other associated shit
Diaphragmatic hernias
Congenital heart disease
Venous drainage is systemic and pulmonary
Askin tumor (PNET, Ewings)
Heterogenous mass originating from bone or soft tissue of thoracic wall
May be this big crock of shit and looks like its in the thoracic cavity and can’t actually tell where its coming from
~10 years old
Older so they be ASKin for it (they can talk)
Ewings - eaten rib
Other

Pleuropulmonary Blastoma
Mixed solid and cystic large intrathoracic mass
<2 years old
Cannot distinguish from CCAM
Bronchopulmonary Dysplasia
Seen in premature babies, >3-4 weeks after birth (>4 weeks old give/take)
Lungs damaged by prolonged mechanical ventilation
Trach is a good clue
Coarse markings with intermixed bubbly lucencies
Markings gradually decrease over years
Wilson-Mikity = BPD but no hx of mechanical ventilation
Congenital Lobar Emphysema
S&S within 6 months of life
Usually affects only a single lobe
LUL > RML > RUL
Starts as a dense area that progressively gets less dense and eventually looks lucent, then it starts looking more lucent and exerts surrounding mass effect from expansion from air trapping
May be caused by extrinsic compression by a foregut duplication cyst
Associated with aberrant left pulmonary artery
Note: Looks similar to pulmonary hypoplasia but the expanded lung in CLE will push mediastinum away and be enlarged where as in PH the bad lung will be small and pull mediastinum toward it
Pulmonary Sequestration
Basically accessory lung
Look for vessel coming off aorta and feeding lung
No connection to bronchial tree
Prefers lower lobes
Intra-lobar Sequestration
More common ~ 75% of cases
Young adult with recurrent pneumonia
No pleural covering
Venous drainage from pulmonary system
Looks like cluster of grapes of cystic shit in a small area or clustered lucent area in the lung
Bronchopulmonary Sequestration
Bronchogenic Cyst
Bacterial (exudative) tracheitis
Ill defined soft tissue densities over the trachea
Tracheal narrowing
Basically shit & debris in the trachea
References: