Pediatric MSK
Apophyseal injuries
Attachment site for muscle or tendon
Acute injury - avulsion injury
Sudden onset pain + popping sensation
Decreased mobility of affected area
Anterior iliac spine and ischial tuberosity = most common sites
Seen with sports (i.e. track)
Chronic - chronic microtrauma that is not strong enough to cause avulsion but will disrupt the growth plate
Conservative management unless significantly displaced ( >1.5 cm)
Toddler Fracture
Oblique fracture at distal tibia in kids starting to walk
Refusal to bear weight
May have history of stand and twist motion
If this is seen in a child who is not walking in anyway then abuse should be considered
Ossification centers
Elbow = CRITOE
Capitellum
Radial head
Internal epicondyle
Trochlea
Olecranon
External epicondyle
Carpal Bones
Capitate 1-3 months
Hamate: 2-4 months
Triquetrium: 2-3 years
Lunate: 2-4 years
Scaphoid: 4-6 years
Trapezium: 4-6 years
Trapezoid: 4-6 years
Pisiform: 8-12 years
Dwarfism
Achondroplasia
Autosomal dominant
Ice cream scoop femur (dont really get this one)
Frontal bossing (protruding forehead)
Inverted V shaped physis (chevron sign)
Metaphyseal flaring
Square shaped iliac wings (tombstone sign)
Genu varum
Spinal deformities
Short limbs
Many findings
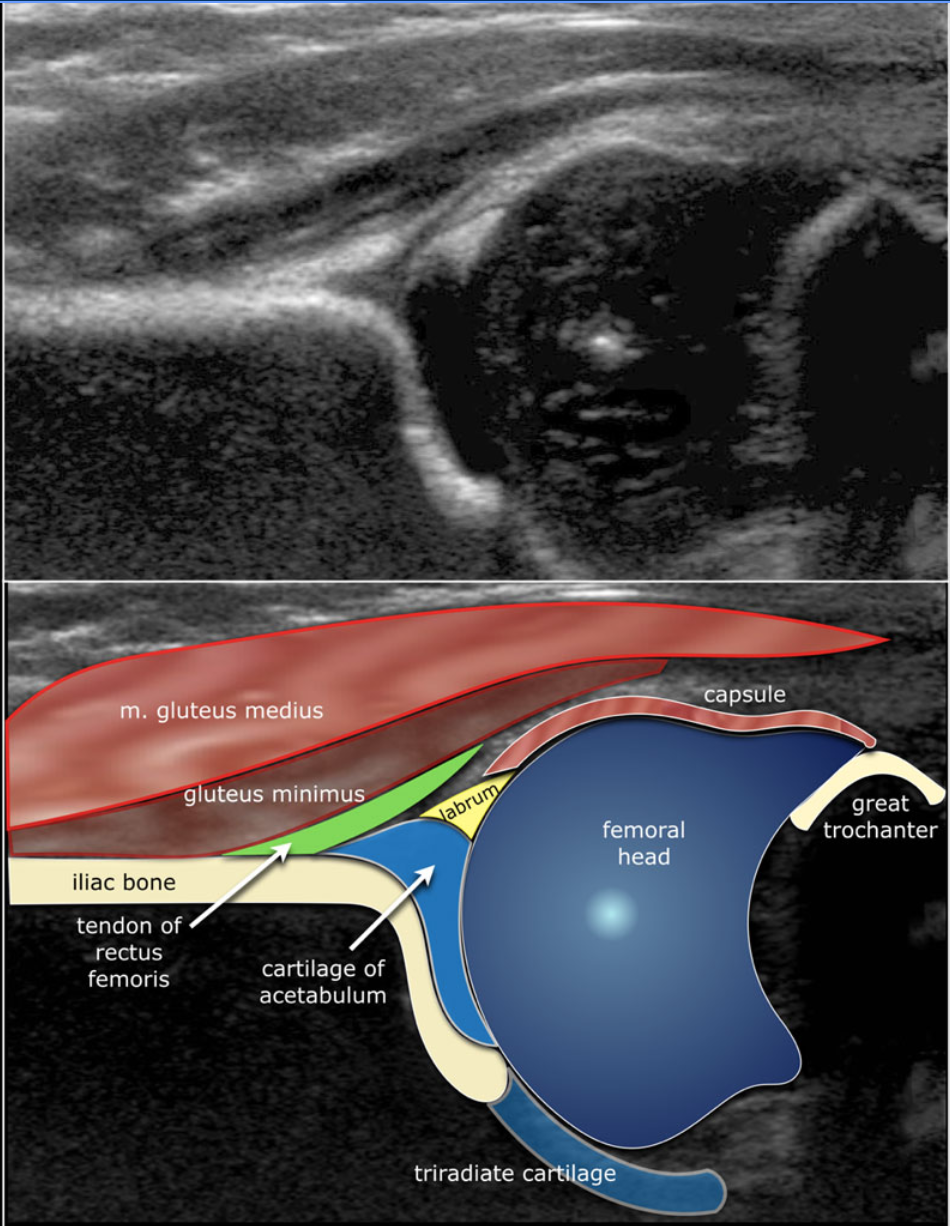
Hip US
Graf classification
Alpha angle
60+ = always good
< 60 = ok if age is <3 months (13 weeks)
Obv if very low then bad
< 50 = ok in neonate as long as gradually increases to 60 by 3 months (13 weeks) old
Want femoral head to be 50% or so seated within the acetabulum
Who gets US - per ACR appropriateness criteria - Any child <4 months old w/
Positive physical exam findings
Equivocal physical exam findings
Females born breech
Family history of DDH
US ideally done at 4-6 weeks
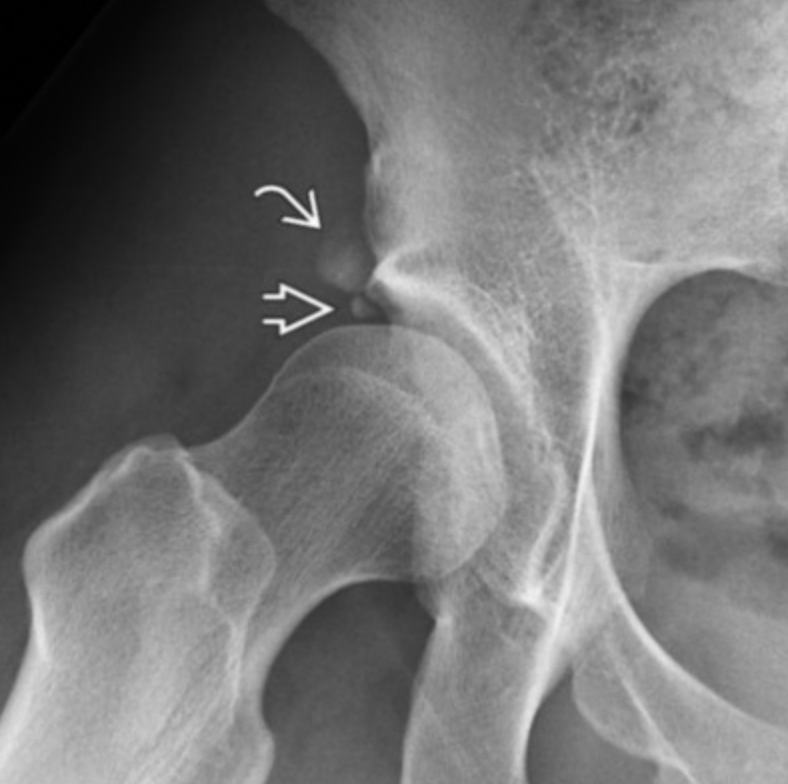
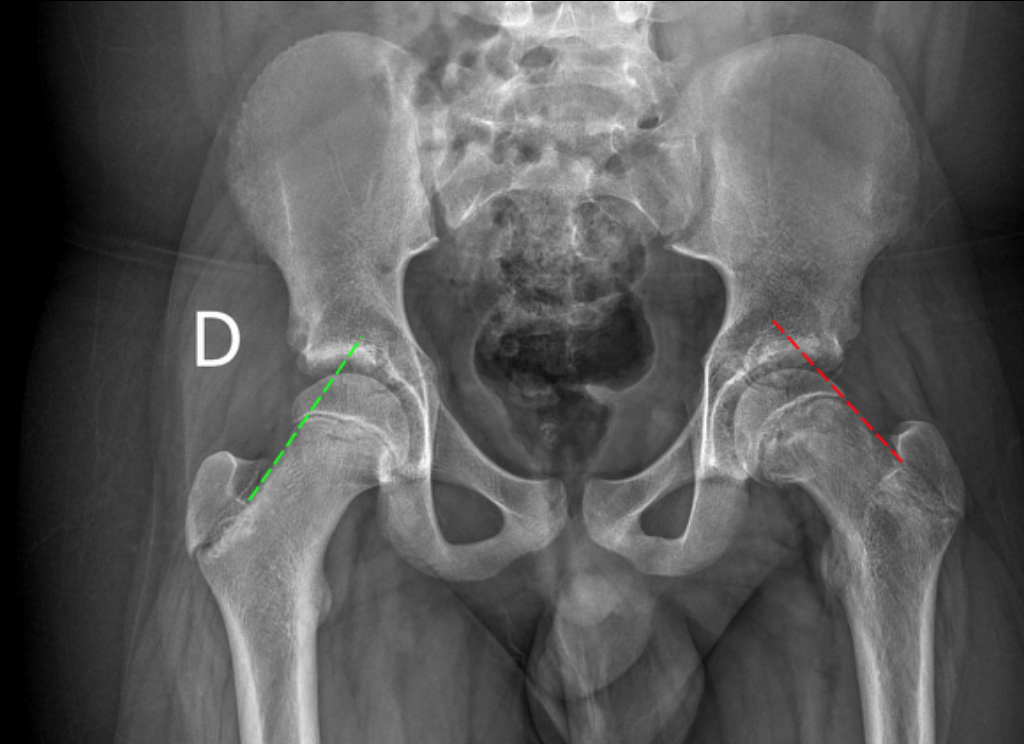
Developmental Dysplasia of the Hips
Shallow acetabuli
Normal acetabular angle <30
Femur can’t sit in acetabuli, uncovered laterally
Sourcil (superior-lateral acetabular roof) is underdeveloped and not downturned
Small osseous fragment that looks similar but not exactly like an os acetabuli due to mineralization of the labrum
Wiberg angle
Crowding in utero
Breech
Twins
Oligohydraminos
F>M
Cleidocranial Dysostosis
Absent clavicles
Wormian bones
Broad mandible/wide angle mandible
Vertebral Plana
Langerhans cell histiocystosis
Medulloblastoma mets
Panner Disease
Avascular necrosis of the capitellum
Thatotrophic Dwarf
2 types
French phone limbs
Significantly curved femurs that look like an old phone handle
Cloverleaf skull
Severe craniosynostosis resulting in skull deformity which looks like a clover
Hips
Legg-Calves-Perthes
Flattening of femoral heads 2/2 idiopathic avascular necrosis
Age 5-8 yo
10% of cases are bilateral
Caucasian > AA
4 Stages
1 - Avascularity - normal XR
2 - Revascularization -
Dense/sclerotic epiphysis
Crescent sign - subtle subchondral fracture of the epiphysis
3 - Healing
4 - Residual deformity - collapse
Slipped Capital Femoral Epiphysis
Fat kids
~12 years old
More often bilateral (30%)
AA >caucasian


Klein Line
Line drawn along superior edge of the femoral neck
Should intersect the superior aspect of the femoral epiphysis
If does not then concerning for SCFE
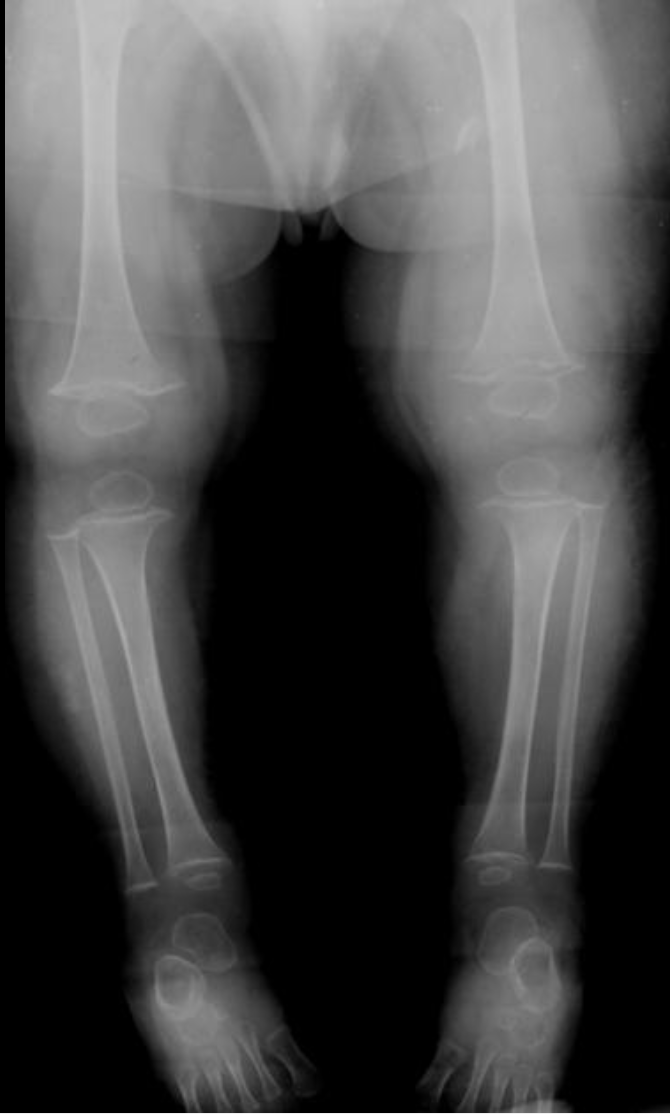
Blount Disease (Tibia vara)
Stress on the posterior-medial physis results in suppression of growth at the proximal medial tibial physis
Angulation is at the metaphysis NOT at the knee joint itself (although the knee joint is probably secondarily angled)
Growth plate slants medially
Metaphyseal-diaphyseal Angle > 11 deg
Can be unilateral or bilateral
Results in genu varum
Compensatory hypertrophy of the medial meniscus
Age 2 and 12 years old
But never before age 2 years old
Does not occur before walking
Thought to occur from too much weight on immature leg
Therefore typically does not occur before age 2
Commonly bilateral
RFs
Fat kids
Early walkers
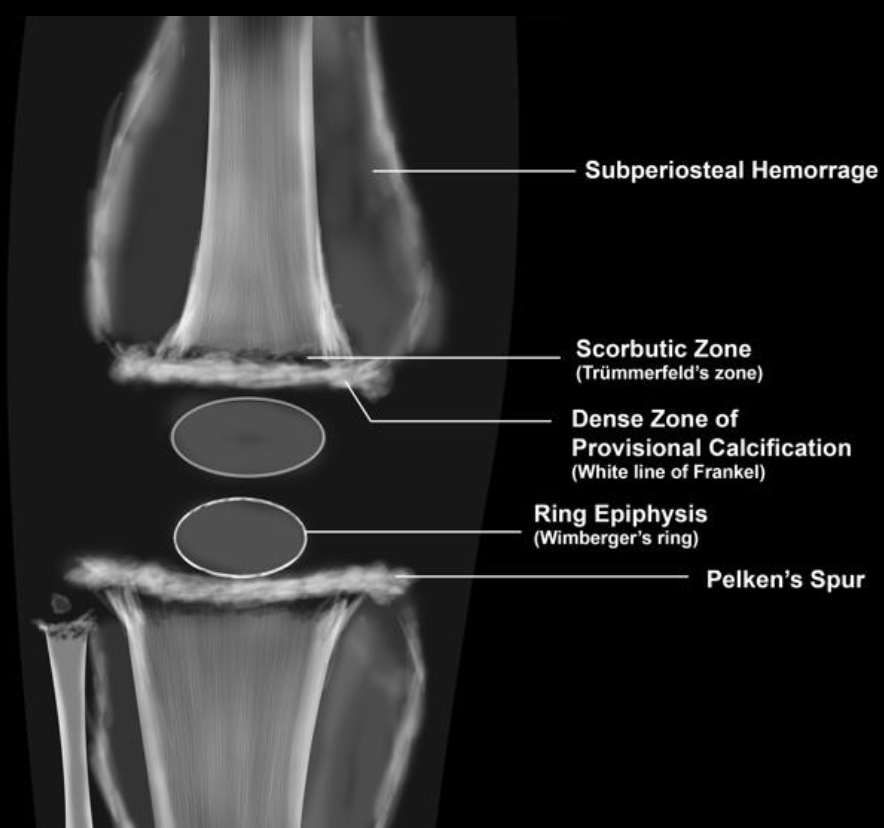
Scurvy
Wimberger Ring sign
Dense calcification surrounding the developing epiphysis
Subperiosteal hemorrhage
Generalized osteopenia
Hemarthrosis
Frankl line = dense line of calcification
Trummerfield zone = lucent zone deep to Frankl line
Pelkan spur = metaphyseal spur from healing microfractures
Campomelic Dysplasia
Chrm 17 mutation in Sox9
Autosomal recessive
Death by 1 year old - respiratory distress
Basically hypoplastic and dysplastic bones - diffusely
Other findings
Hydrocephalus
Hydronephrosis
Congenital heart anomalies
Syphilis
Wimberger sign
Bilateral proximal, medial tibial metaphyseal destruction
Periosteal reaction in Newborn
Infection
Syphilis - seen around 2 months
Rubella - seen before 2 months
Mets (neuroblastoma)
Abuse
Caffey’s
Prostaglandin therapy
Look for heart with PDA clip or some other shit in heart
Physiologic
Seen 3 months of age and should resolve before 6 months old
Proximal (femur) before distal (tibia)
Always involves diaphysis
Osetomyelitis
Metaphysis is a septic tank
Look for normal radiograph followed by lesion development a week or two later near metaphysis
The physis is largely avascular so thought to act as a barrier to prevent spread from metaphysis to epiphysis
Key Organsisms
Staphs aureus > Strep = most common for hematogenous osteomyelitis in kids
Kingella kingae = kids <4 years old, loves the epiphysis/epiphyseal cartilage, gram neg bacillus
Pseudomonas & E.coli = osteomyelitis from penetrating trauma, classically in the foot
Chronic recurrent multifocal osteomyelitis
Multiple relapsing/remitting bones lesions
Kids & adolescents
Basically multifocal areas of edema on MRI, usually in long bones, lytic on XR
Also characteristically may involve the clavicle
Classically the metaphysis like regular osteo
Associated conditions
Psoriasis
Pyoderma gangrenosum
Wegeners
Takayasu
Majeed syndrome
SAPHI
Metaphyseal bands
Lucent metaphyseal band =
Leukemia
Neuroblastoma
Rickets
Oseto
Dense metaphyseal band
Lead
Chronic anemia (sickle cell, thalassemia)
Methotrexate use
Growth arrest band in juvenile RA
Amniotic Band Syndrome
Amniotic bands cut off blood supply to any structure and cause it not to form or form abnormally
No increased risk with subsequent pregnancies
Note thumb and radius
If missing/abnormal think of something more syndromic and not ABS
Probably just fingers in ABS
Engleman Disease
Fusiform enlargement & sclerosis of long bones
Spares epiphysis
Hot on bone scan
Autosomal dominant
Rickets
Targets rapidly growing bones (knees, wrists)
Cupping/fraying and widening of metaphysis - symmetric
Demineralized Bone
Not seen in newborns (still have Vit D from mom)
If you
Idiopathic Chondrolysis
Progressive articular cartilage destruction of unknown cause
Unilateral
No systemic symptoms
Inflammatory markers are normal
Early imaging is normal
Abnormal signal in middle third of femoral epiphysis
Holt-Oram Syndrome
Absent radius
Atrial septal defects
NF-1
Scoliosis
Anterior-lateral tibial bowing
Fibular pseudoarthrosis
Wormian Bones DDx:
Osteogenesis imperfecta
Cleidocranial dysostosis
Pyknodysostosis
Juvenile Idiopathic Arthritis (aka JRA)
Rice bodies (necrotic small bodies) in joint space
Also seen in TB
Age <16 yo + 6+ weeks of joint pain
Nonspecific bone and cartilage damage
Early growth plate closure
Lateral condylar fractures
Ages 5-10 typically
Varus injury to a supinated and extended forearm
Crescentic rim along the condyle (what i thought was the epicondyle is apparently the condyle in kids)
Most commonly SH-4 fxs
Milch type 1 & 2 classifications
Pyknodysostosis
Osteopetrosis
Acroosteolysis
Wormian bones
Multiple fxs with minimal trauma
Short stature
Typically shown on a hand XR with dense bone and missing finger tips
Non-accidental Trauma
Fractures at different stages of aging
Long bone fractures - not specific for NAT
Specific findings for NAT
Metaphyseal corner fracture
Posterior rib fractures near costovertebral joint
Isolated subdural hemorrhage
Duodenal hematoma or post-traumatic pancreatitis in patient with otherwise no history of trauma
Workup
Skeletal survey
Should comment on presence/absence of wormian bones
Consider bone scan
Head CT/MR
Fibromatosis Coli
Benign masses in the sternocleidomastoid of neonates
Looks like testicles in the neck
Looks like two round balls = two heads of the SCM muscle
Goes away on its own
Kohler Disease
Avascular necrosis of the navicular
Equivalent of Muller-Weiss in adults
Hypophosphatasi
Cupping/fraying of metaphysis IN newborns
Thumb-Absent Radius syndrome (TAR)
Absent radius with thumb present
Holder
Osteogenesis Imperfecta
Type 1 collagen issue
Triad of
Blue sclera
Wormian bones - easily fx
Hearing loss
Dental disease too - messed up teeth
References: