Pediatric GI
Pyloric Stenosis
Non-bilious vomiting
May just seen distended stomach with air fluid level in on XR
3W to 3 months old
Not in newborns or older kids
More common in first born males
Measurements
> 3 mm wide
> 15 mm long
Double track sign = basically two muscular walls of the pylorus are so thick they look like two tracks
Antral/mucosal heaping sign = pylorus becomes so hypertrophic that it pushes into the gastric antrum and indents it
Managed with pylorotomy
If you have findings consistent with pyloric stenosis on US you need to extend the exam by 3-5 minutes to confirm the pylorus is still closed and does not allow passage of gastric contents
If in 3-5 minutes it opens up and contents can pass freely then you are looking at a pylorus spasm which is managed medically
Intraluminal calcifications of the bowel Ddx:
Total colon Hirschsprung disease
Multifocal intestinal atresia (results in stasis of stool and subsequent calcifications)
Anorectal malformation resulting in mixing of stool and urine
Rectourethral fistula
Intussception
3 months to 3 years old
Not in newborns or older kids
Measurements
< 2.5 cm
Likely small bowel-small bowel
Not getting an air enema
> 2.5 cm
More likely ileocolic
Needs air enema
Air enema
Basically just push air into their butt until you see air throughout the bowel
Contraindications
Need plain film first to rule out perforation
Need to make sure there is no peritonitis based on exam
Pressure should not exceed 120 mmHg
Duodenal Atresia
Caused by failure to cannulate the bowel
Will see dilated fluid filled duodenum
Note typically should not see in utero
Associated with down syndrome (30%)
Polyhydraminos
Double bubble
Colon & Rectum
Gastric Pseudomass
Ingested material in stomach forms a conglomerate
Duodenal obstruction
Double-bubble
Dilated stomach in LUQ
Dilated proximal duodenum in RUQ
Polyhydraminos
Cant get food through so eat less, so more fluid
Need to see an image where the two bubbles connect to ensure it is not another cystic structure
If do not connect, consider
Enteric duplication cyst
Choledochal/ovarian/splenic/liver cyst
Pseudo-dubble-bubble
US scan traverses the gastric fundus and antrum-BOTH STOMACH
Here both bubbles will be in the LUQ
Get image showing connection and will show just stomach basically
Jejunum & Ileum
Normal diameter <7 mm
Normal length <15 mm
Normally seen with minimal fluid
Atresia typically a result of a vascular event
Jejunal atresia
Triple bubble sign

Small Left colon syndrome (Meconium plug syndrome)
I think this may be the same thing as functional immaturity of the colon, but unsure
Seen on contrast enema typically with caliber change at splenic flexure - caliber change is not glaringly obvious
Associations -
Maternal DM
Maternal pre-eclampsia because of use of magnesium-sulfate
Treatment = contrast enema with water soluble contrast
Hirschsprung
Hx
Newborn with no BM
Kid who went home and comes back very sick with necrotic bowel
Recto-sigmoid ratio <1
Sigmoid colon bigger than rectum in Hirschsprung disease
Normally the rectum is bigger than sigmoid colon and the ratio is >1
Multiple dilated loops of bowel with transition point at recto-sigmoid junction on enema
Ondine curse = total colonic hirschsprung disease + central hypoventilation
Sawtooth pattern of bowel on fluoro
Biliary Atresia
Presents with jaundice and essentially signs of cirrhosis in a young child
Extrahepatic biliary duct destruction with progression to involve the intrahepatic ducts
Triangular cord sign - echogenic tissue adjacent to right portal vein which represents fibrotic remnant of bile duct
Ghost Gallbladder triad (multiple findings to say a small and fucked up GB)
Irregular and discontinuous GB wall
Hypoplastic/atretic GB
Irregular GB contour
Can see abnormal/tiny gall bladder but will not really see intrahepatic ducts, especially on angio
Kasai classification
Need liver transplant or will typically die
Nuclear medicine testing
Give Tc-99m Diosgenin (DISIDA) or Mebrofenin (BRIDA) —> high hepatic excretion rate and short transit time
In biliary atresia will see good uptake of the radiotracer with no excretion at 24 hours
Phenobarbital —> increases biliary excretion
Administered 5mg/kg (divided in half for a BID dosing) for 3-5 days before procedure
Giving phenobarbital helps the excretion process so that there is not a false positive (i.e. very slow excretion with otherwise normal biliary anatomy)
Should seen radiotracer excretion into bowel, typically do not see well in the ducts but should be excreted and seen in the bowel (if normal), this will not be seen in BA
Duodenal hematoma
Expect in setting of trauma (abuse, handlebar injury, EGD) or Henoch-Schonlein purpura
Will see narrowing of second and third portions of duodenum
Bowel Obstruction
Draw a line horizontal to the abdomen at the level of the umbilicus
If there are more dilated loops of bowel above the line —> proximal bowel obstruction —> upper GI is next step
If there are more dilated loops of bowel below the line —> distal bowel obstruction —> contrast enema is next step
High bowel obstruction = obstruction proximal to the mid-ileum
Normal caliber colon will be present - there is enough normal proximal small bowel to make secretions which can feed the colon
Ex - high ileal atresia, jejunal atresia will cause this
Low intestinal obstruction = obstruction in distal ileum or colon
Will have micro-colon because not enough proximal small bowel to make secretions to nourish the colon
Ex - low ileal atresia, meconium ileus
Easy DDx for SBO in kids after immediate newborn period = AAIIMM
Adhesions
Apendicitis
Intussception
Inguinal hernia (incarcerated typically)
Midgut Volvulus
Meckel’s Diverticulum
Contrast Enema
Will help you gather information via the following algorith
No microcolon
Normal
Hirschsprung
Meconium plug
Microcolon present
Ileal atresia (long segment microcolon)
Meconium ileus (long segment microcolon)
Colonic atresia (short segment microcolon)
Colon & Anus
Maximum diameter of 2 cm, can look prominent especially in third trimester
Imperforate Anus
Associated with VACTERL
Associated with tethered cord —> need to get a spinal US to evaluate for this
Meconium Ileus
Will see diffuse micro-colon
Highly related to cystic fibrosis
US findings
Dilated and hyperechoic bowel proximal to the stomach
2 types
Uncomplicated
Only an obstruction
Treated with high osmolar enema
Want contrast to get to bowel proximal to obstruction so that the high osmolar contrast can draw fluid into the bowel and flush it out
Complicated
Aka meconium peritonitis - leakage of GI contents into peritoneal cavity after bowel rupture
Intraperitoneal calcifications!
Note you can have other abdominal calcs like benign shit but look for calcs along the inferior aspect of the diaphragm and along the liver edge but not in the liver, these are intraperitoneal and are more suggestive of meconium peritonitis
In males can see calcs in the scrotum due to peritoneum extending through patent processus vaginalis
CMV will cause calcs within the liver and spleen itself
Free fluid within the abdomen, may be complex,
Meconium pseudocyst - basically an abscess with matted bowel surrounding it
Typically need surgery
Malrotation
Midgut = bowel supplied by the SMA
In utero the midgut will push through the umbilical space
Then rotate 90 degrees
Bowel will then come back through the umbilicus and rotate another 270 degrees
If you have a space occupying lesion, or oligohydramnios (decreases space to rotate) then you will have increased risk of malro
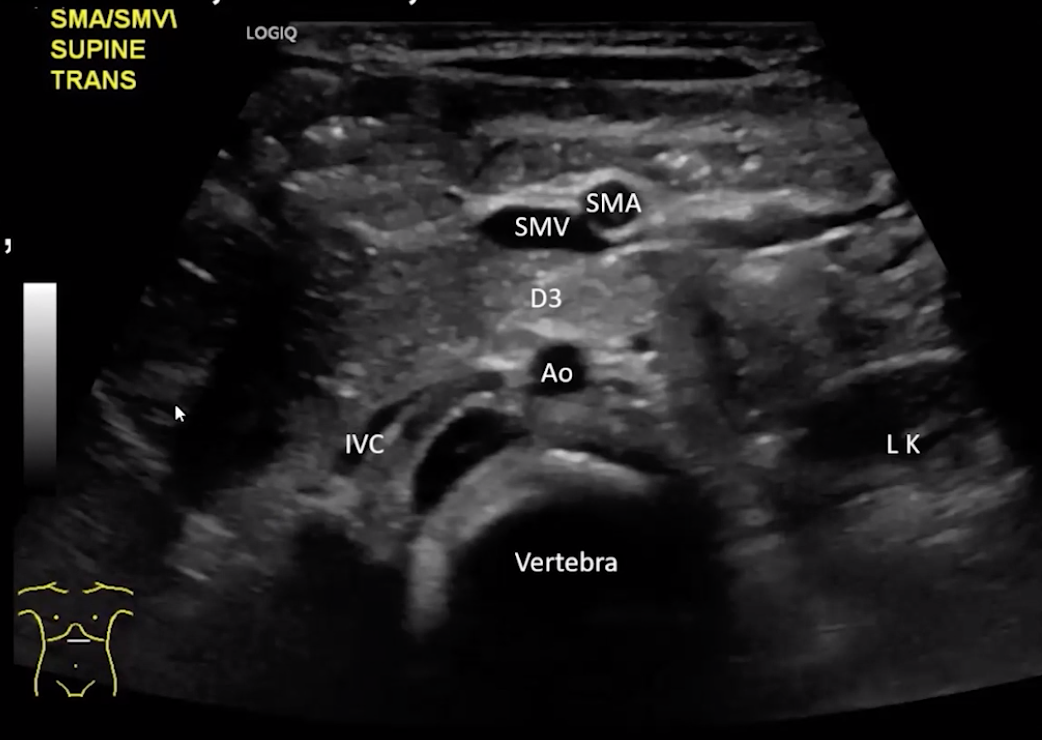
Normal Anatomy
D3 is retroperitoneal, should pass between SMA & aorta
SMV on same side as portal vein
SMA on same side as spleen
Note that the SMA will have an echogenic halo around it and the SMV will not, important when there is concern for volvulus the SMV may be collapsed and you may just seen SMA which can be identified by that halo
May be helpful to look for left renal vein crossing over midline to orient yourself too
Bilious vomiting
Because twisting occurs at the third portion of the duodenum which is distal to the ampulla of vater
Midgut volvulus is the feared outcome
The abnormal orientation of the bowel causes it to twist on its mesentery creating the corkscrew bowel
Normally the mesentery is broad and extended from the ligament of treitz in the left upper quadrant to the ileocecal valve in the RLQ
Whirlpool appearance
Secondary findings may include distended stomach (shit cant pass beyond the distal duodenum)
Ladd Bands
Bands of fibrous tissue between the mal-positioned cecum and the RUQ (abdominal wall, liver)
When the gut mal-rotates the cecum will typically be located in the RUQ next to the duodeum
The peritoneum will then further form and lay down fibrous tissue between the mal-positioned cecum and the RUQ abdominal wall/liver and will have to cross the duodeum in the process
These bands of fibrous tissue then compress the duodeum and cause obstruction
Ladd procedure
Meckel’s Diverticulum
Omphalomesenteric duct remnant
Usually within 2 feet of ileocecal valve
Usually in child <2 years old
2 inches long
Complications
Obstruction
Act as a lead point for intussception
Meckel’s scan
Nuc med scan with pertechnetate which localizes to gastric tissue
So will not be positive is all cases of Meckels, will only be positive in those cases with ectopic gastric tissue which is ~30%, however those are the ones that are typically symptomatic
Done when patient is NOT bleeding
May need to pre-treat with
Glucagon to slow gastric motility
H2 blocker - slows secretion of pertechnetate so it stays around longer so you can see it better
Pentagastrin - enhances uptake of pertechnetate by gastric mucosa
Can also be used in evaluation of enteric duplication cyst as sometimes they will contain ectopic gastric tissue
Necrotizing Enterocolitis
Highest risk around 28 weeks gestation age regardless of when delivery is
blood supply in utero is highly protected to the fetus and so perfusion is almost always present, unless mom is in near death situation
This is why NEC is really only seen in pre-mature babies after delivery because in utero they are protected by moms blood supply
Bacteria dissect between the muscularis and mucosal layers which then develop air between the bowel layers
The air in the bowel wall will eventually spread to the veins which drain the bowel (superior mesenteric vein)
Air in the SMV will drain back to the portal vein
This is why portal venous gas is seen with NEC!!
When evaluating on a radiograph you look for the findings below but a key feature to keep in mind
If you see what you suspect to be air by the liver or free air or whatever, get a left lateral decubitus film to evaluate for free air
If negative and you are still unsure wait 20 minutes with the patient remaining in the left lateral decubitus position and re-image
The reason for this is because the peritoneum will be full of shit and sticky crap which makes the transit of air slower in bad cases of NEC so will take more time for the air to move and may not be seen on the initial lateral film
Findings
Pneumatosis
Focally dilated bowel, classically in RLQ - will be fixed = not change over time
Terminal ileum and right colon is most commonly affected
Featureless small bowel
Unchanged bowel gas pattern
Who gets this
Premature children
Low birth weight
Prenatal hypoxia/asphyxia
Patients with cardiac disease (can be otherwise normal)
Congenital Diaphragmatic Hernia
Left > Right
Not a surgical emergency
Presents with bowel in hemi-abdomen, may appear as a hemi-thorax white out rather than typical appearance of bowel as baby has not “eaten” enough air yet
Stomach
Normally visualized around week 13/14 - not a definitive timeline though
If do not see in an age where you should, repeat study in few days
Can be better or poorly visualized based on distention from baby drinking amniotic fluid
Large stomach
Obstruction
Note pyloric stenosis is very rare to diagnose in utero
Small stomach
Esophageal atresia
Hyperechoic material in stomach
Ingested material/ skin cells
Ingested blood - look for concurrent subchorionic hemorrhage
Esophageal Atresia
Suspect if stomach is not visualized on multiple attempts
Polyhydraminos
Many have tracheo-esophageal fistula so can still have atresia and have fluid in stomach
On radiographs look for no bowel gas
Look for high NG tube, dont mistake for ET tube, enteric tube should not be that high
Look for presence of a right sided arch
Changes surgical approach
Tracheo-esophageal fistulas
Blind esophageal pouch with connection between distal esophagus and trachea (85%)
Lots of air in stomach
No fistula, so blind pouch and stomach connects to nothing proximally
H type - 1% - air in stomach
Associated with VACTERL
Duodenum
Not normally seen in utero
DDx for dilated fluid filled duodenum
Duodenal atresia (most common)
Webs
Extrinsic obstruction —> annular pancreas , malrotation
References: