Pediatric Body
Renal
If you do not see a kidney on one side you should keep the two major items in the differential
Solitary kidney (other side is just absent)
Be sure to look throughout the pelvis and abdomen first before stating this as kidney may be ectopic
Crossed fused renal ectopia
Basically the two kidneys are fused and located on one side
Will see abnormal tissue along the kidney which is the fused portion of the second kidney, will be more subtle than what a fused kidney looks like in horseshoe kidney for example
Calyceal Diverticulum
Will look like simple cyst but will show strong enhancement on delayed phase which represents communication between the diverticulum and the calyx
Layering of stones, calcium = highly suggestive of diverticulum
Ureterocele
Looks like filling defect in bladder
Bilateral Renal Agenesis
Suspect in newborns with pneumothorax
PTX raises concern for pulmonary hypoplasia
Pulmonary hypoplasia results from in utero oligohydraminos
Oligohydraminos —> renal agenesis
US will show
Flattened adrenal glands
Decompressed bladder (no urine being made)
Lethal
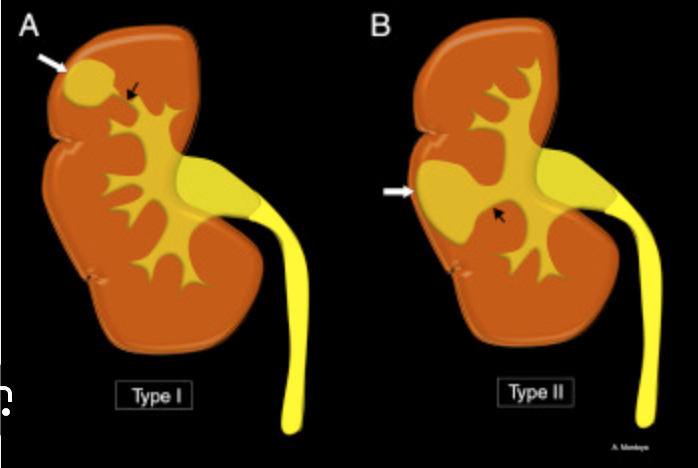
Duplicated collecting system
Can be partial or complete but when there are two collecting systems in one kidney
May be easy to see as they can have enlarged column of berlin
Highly associated with ureteroceles (if you see a ureterocele you need to look for duplicated system)
Upper moiety
typically has the ureterocele and becomes obstructed
Chronic obstruction results in cystic dysplasia and scarring
Upper ureter will insert ectopically
Will be lower and medial
Drooping lily sign
Only lower moiety fills so looks like a flower
Weigart-Meyer rule
the ectopic ureter will be medial and inferior
Multicystic Dysplastic Kidney
Ureteropelvic junction obstruction
Basically what the name says, there is an obstruction at the junction of the renal pelvis and ureter
Causes
Idiopathic
Compression by a vessel (can be a very small vessel and does not actually look like compression, just looks like the vessel is crossing the UPJ)
Look for accessory renal arteries which may be doing this
On imaging looks like severe hydro with dilatation of the ureter proximally
On multiphase urogram will likely not seen contrast in the affected ureter because there an obstruction but can see it in the calyces
Treatment
May resolve
Pyeloplasty (basically cut out the obstructed part and sew the other shit back together)
Can lead to renal cystic dysplasia
Basically chronic obstruction causes normal renal parenchyma to be replaced by communicating cysts which then becomes scar tissue
Different from MCDK because MCDK is congenital and renal pelvis is congenitally absent
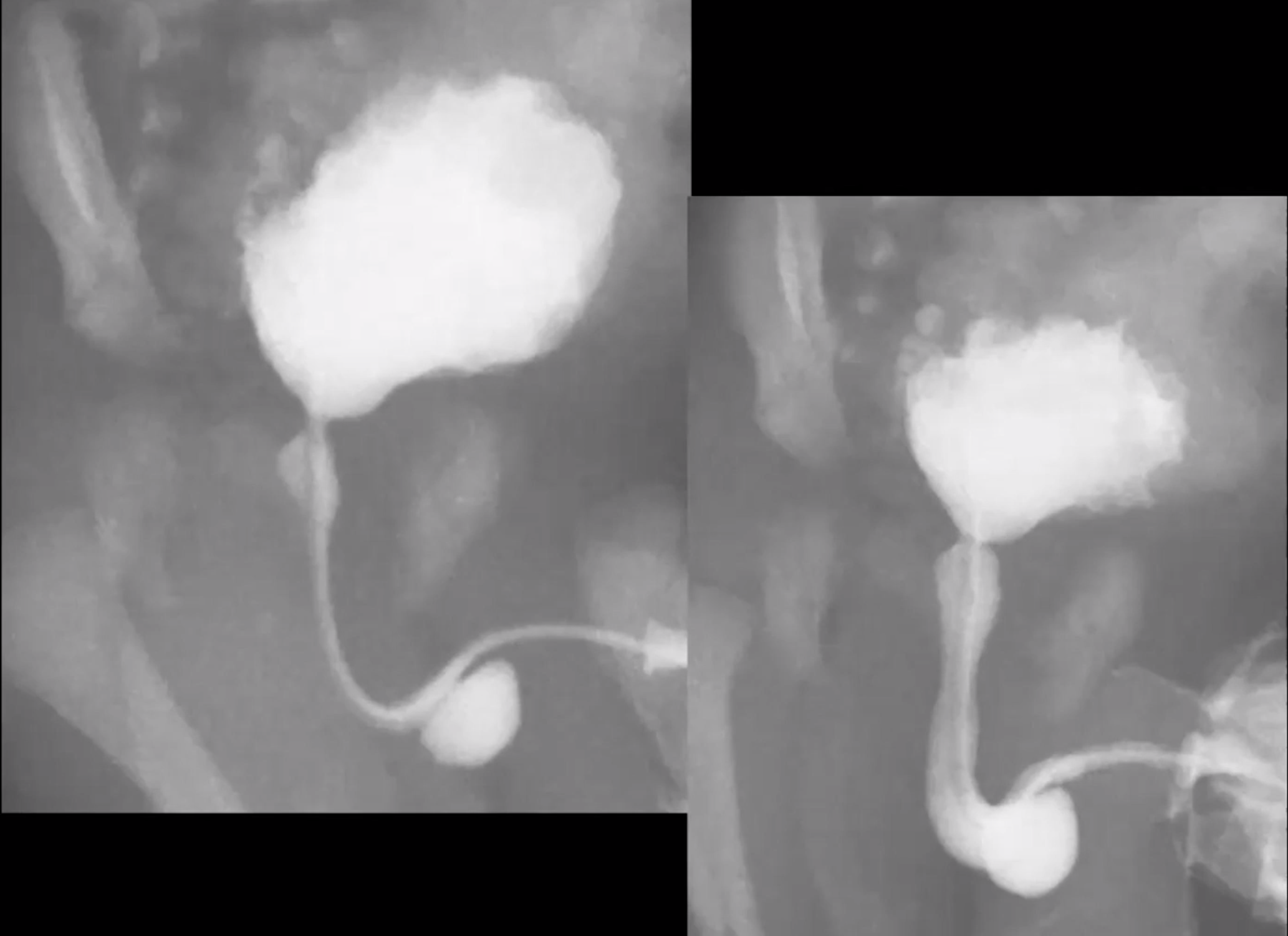
Posterior Urethral Valves
Only males
If identified pre-natally will have oligohydramnios with pulmonary hypoplasia
Keyhole appearance
Due to dilatation of the bladder and posterior urethra
The bladder will typically have irregular contour due to chronic outlet obstruction - all because th ebladder is contracting against a closed door
Elongated
Trabeculated
Maybe some diverticula
Findinsg associated with preserving renal function & therefore better prognosis
Urinary ascites
Severe unilateral vesicoureteral reflux
Urinoma
Large bladder diverticula
These all basically act to relieve high pressure within the bladder
Basically these are all protective features
Treated surgically
Anterior Urethral Valves
Basically same as posterior urethral valves but located within the distal urethra (like in the shaft of the penis)
Will have a diverticula
Will have irregular bladder and dilated urethra proximal to the valve
Prune Belly Syndrome (Eagle-Barrett Syndrome)
Findings
Hydroureteronephrosis
Cryptorchidism
Abdominal wall laxity
References:
Case courtesy of Henry Knipe, Radiopaedia.org, rID: 41934