Pediatric Abdominal Masses
Renal Masses
Neuroblastoma
Mass most commonly seen in adrenal glands > retroperitoneum/paraspinal > elsewhere
Age <2 yo
Arise from neuroectrodermal or neural crest cells
Invade spinal canal
Necrosis, hemorrhage, calcification common
Commonly mets to bone (and chest)
Heterogenous appearance on T1, T2, enhancement
MIBG - neuroblastomas secrete catecholamines
Retroperitoneal lymphadenopathy common
Neuroblastomas
Most commonly from ADRENAL gland, not kidney
Commonly have calcifications
Age <2 yo
More commonly mets to bone (also chest)
May invade spinal canal
Retroperitoneal lymphadenopathy common
More in section below
Mesoblastic Nephroma
Seen in first 3 months of life, 90% before 1 year old
Most common solid renal tumor in kids
Solid mass, typically no calcs or blood

Hemangioendothelioma
Aka infantile hepatic hemangioma
Large abdominal mass arising from liver
Peripheral ring of hypervascularity
Internal doppler flow too
Will eventually regress
Can cause HF, compartment syndrome
Ganglioneuoma
Basically the benign version of neuroblastoma
People <20, note this is way older than <2 for neuroblastoma
Will be more well defined
Occur anywhere along peripheral autonomic ganglion sites, most commonly posterior mediastinum and retroperitoneum
No necrosis
Can invade spinal canal
Appears similar to neuroblastoma but no necrosis and is more well circumscribed almost with a capsule looking rim
Will have higher ADC values than neuroblastoma
Note - schwannoma will be centered in neural-foramen and will be in adults typically
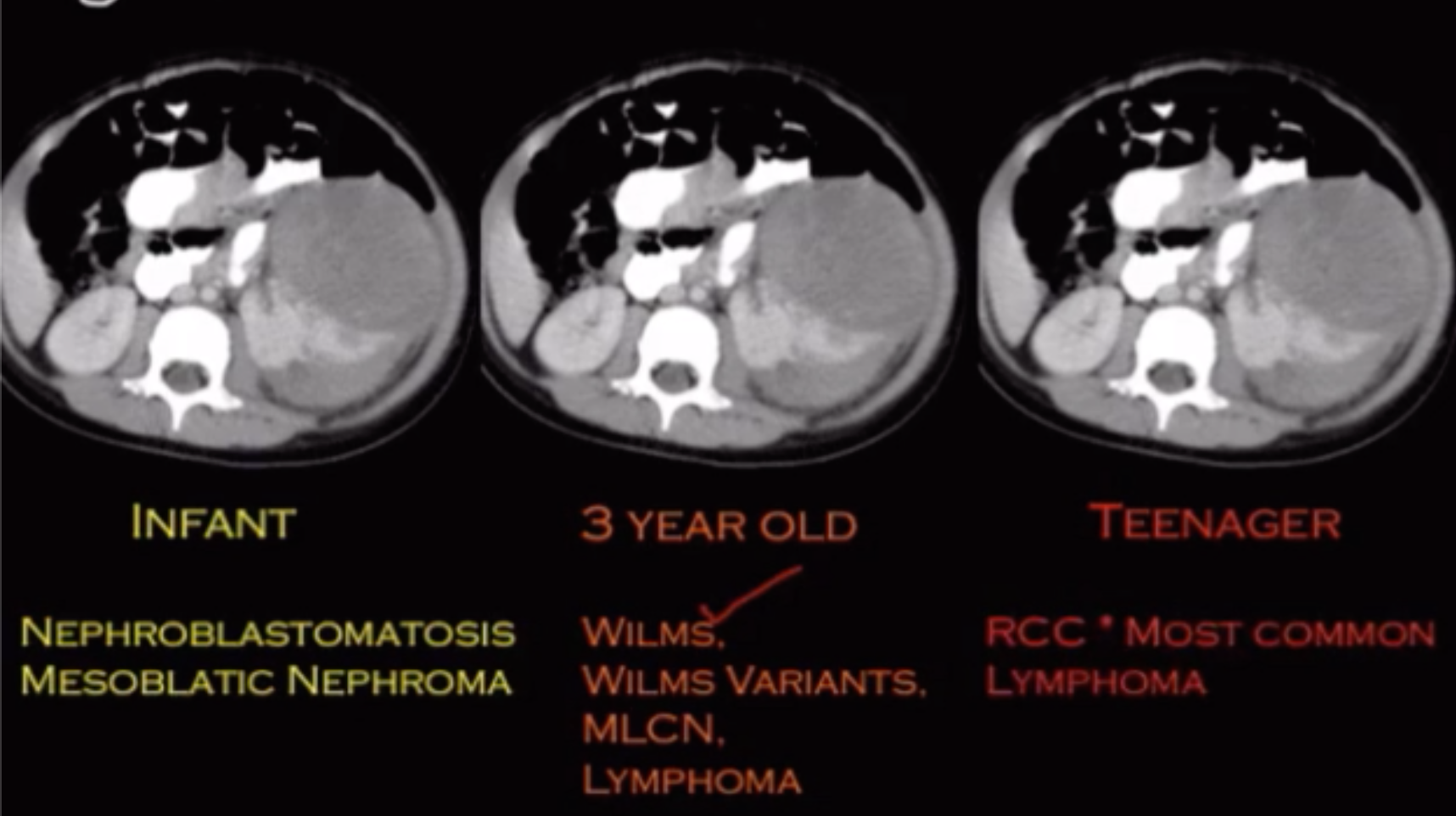
Wilms Tumor
Rarely has calcifications
Age ~4 yo (never seen before 2 months old)
More commonly mets to lung & liver
Does not invade spinal canal
Retroperitoneal lymphadenopathy uncommon
Claw sign
Evaluate for renal/IVC thrombus or invasion
Do not biopsy - will seed
Variants
Clear cell - likes to have lytic met to bone
Rhabdoid - causes WHO 4 brain tumors - worse prognosis
Kasabach-Merritt Syndrome
Rapidly growing vascular tumor leads to thrombocytopenia, MAHA, and coagulopathy
Mostly associated with kaposiform hemangioendothelioma
Infantile hemangioma can also cause
Ganglioneuroblastoma
Basically intermediate between ganglioneuroma (low grade) and neuroblastoma (high grade)
Kids <10 years old
Arise from neuroectodermal cells
Seen in adrenal gland & along sympathetic chain (typically paraspinal regardless of in chest or abdomen)
Cannot really tell the difference from neuroblastoma on imaging, need tissue
Nephroblastomatosis
Persistent nephrogenic rests (embryologic tissue that makes up the kidney)
Looks like thick rhind around kidney (or like the renal cortex is severely thickened)
Can be precursor to wilms tumors
Found in all cases of bilateral wilms tumor
Multilocular Cystic Nephroma
Michael Jackson disease
Males 3 months - 5 years
Middle aged women
Multiloculated cystic mass
Hemorrhage and necrosis uncommon
DICER1 gene mutation
10% associated with pleuropulmonary blastoma
Just looks like densely packed cysts together
Hepatoblastoma
Heterogenous lesion with peripheral satellite lesions
Malignant
Kids < 5 years
AFP secretion
Associations
Beckwidth-Wideman
Gardner / FAP
Lymphatic Malformation
Multi-cystic, lobulated lesion in the abdomen
May have internal fibrous looking tissue but predominantly cystic
Rapidly enlarge with minor trauma, especially with internal hemorrhage
Do not respect soft tissue planes
Liver
HCC
Rare in kids <5 years old
Other
Mesenchymal Hamartoma
Complex cystic mass
Kids < 5 years old
References: