OBGYN Ultrasound
Imaging approach
Transabdominal
Want full bladder
Allows window for US waves to travel through
Distended bladder will displace bowel loops out of the imaging view
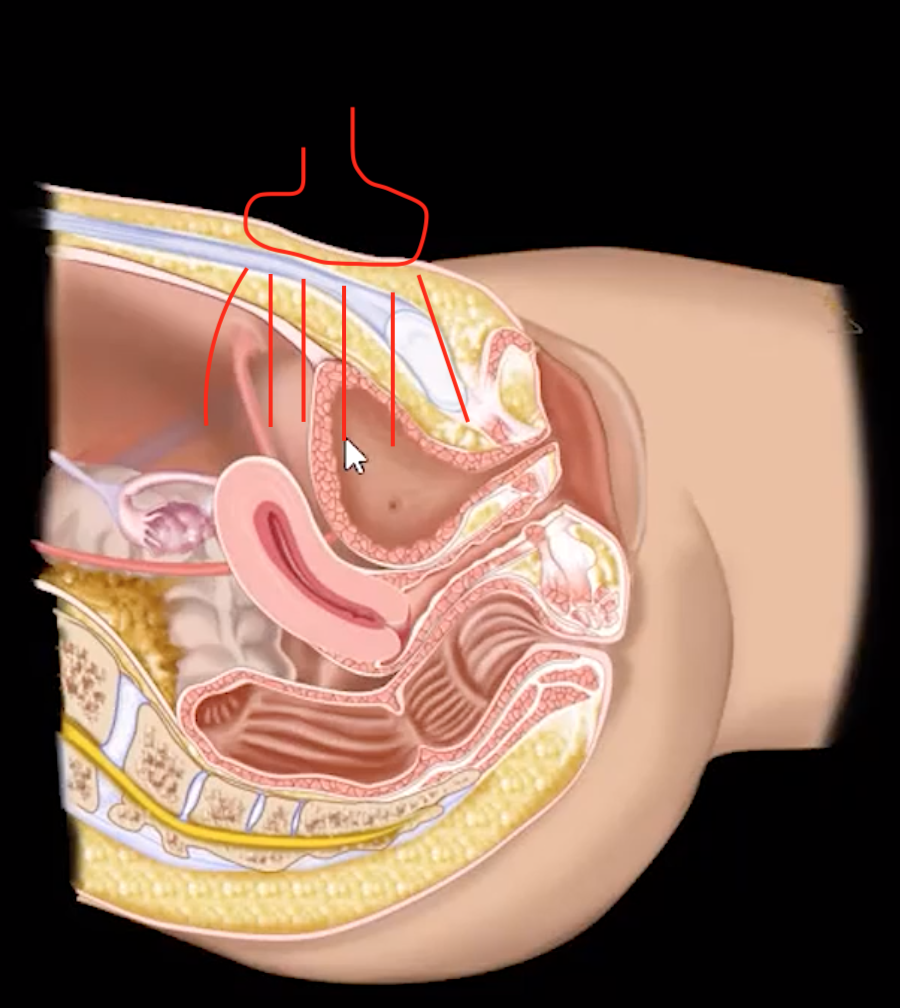
Version & Flexion
Most commonly ante-verted & ante-flexed
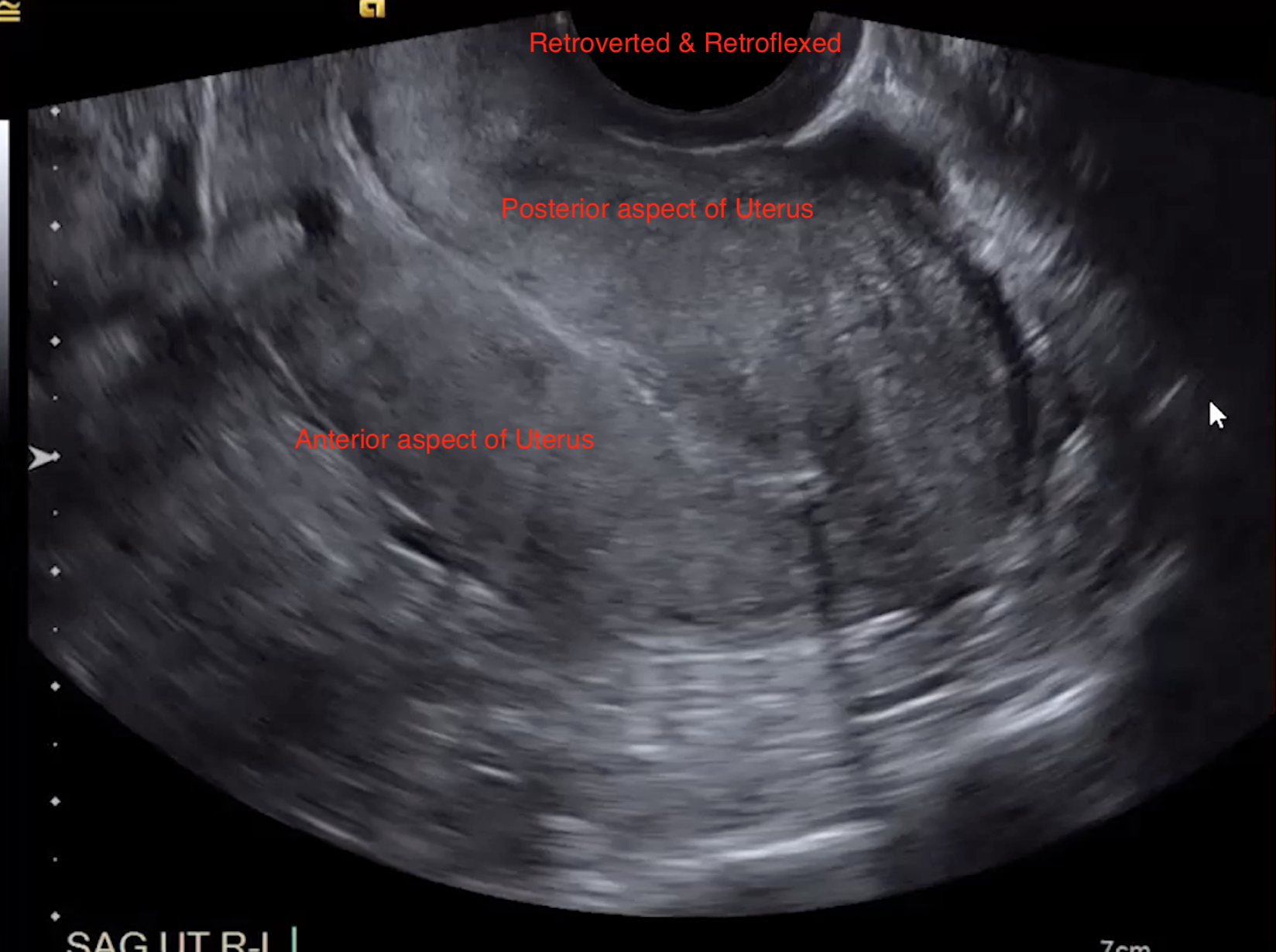
Second most common = retro-verted & retro-flexed
Version = cerVix
Ante-verted cervix = Internal os is anterior toward bladder (& external os is posterior toward rectum)
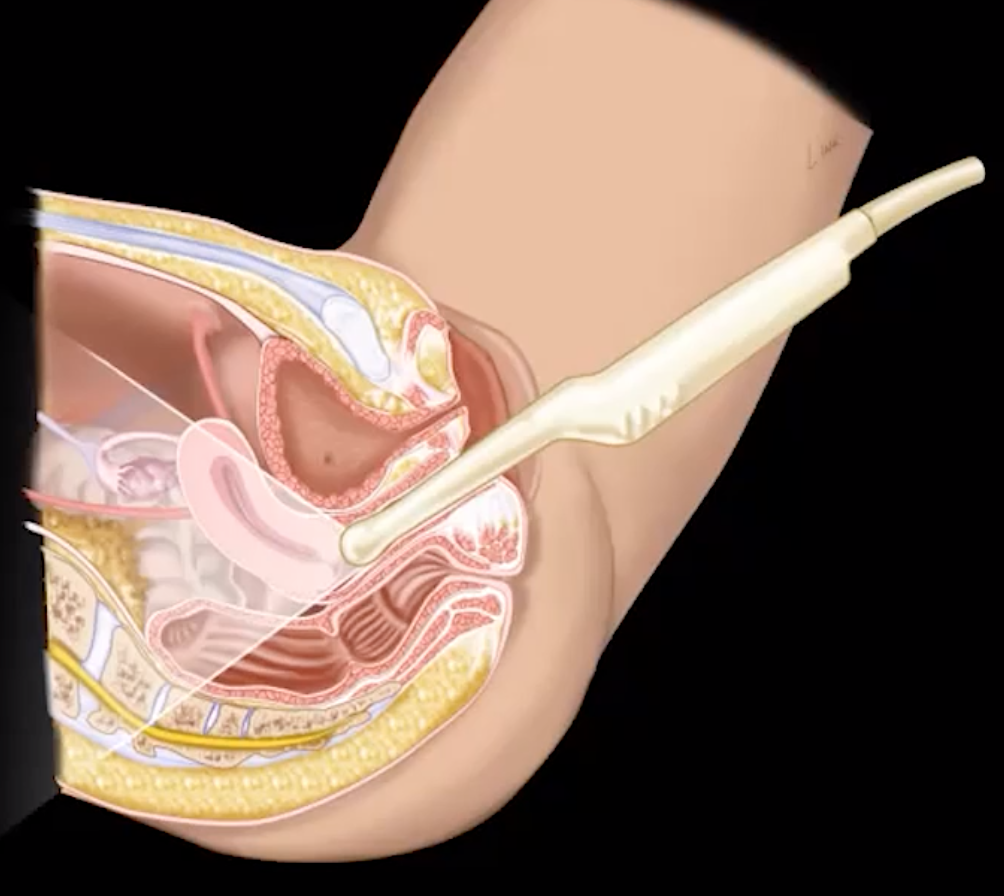
Transvaginal
Want decompressed bladder
Uncomfortable for patient
Will displace uterus which now may be outside the field of view
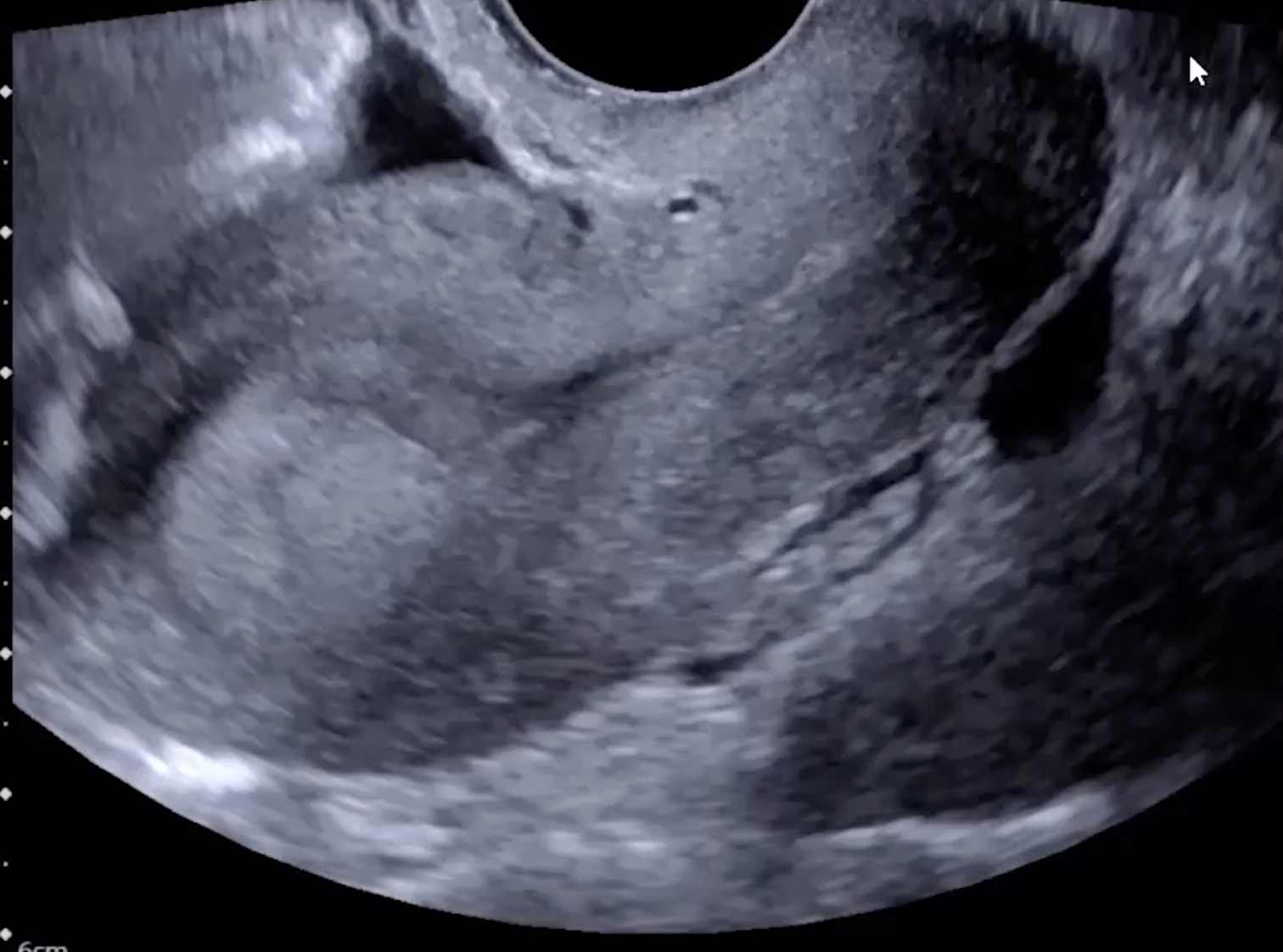
Ovarian Torsion
Twisting of ovary on suspensory ligament leading to occlusion of vessels
Veins occluded first so blood cannot leave ovary leading to venous congestion and increased size of ovary
Arterial occlusion then occurs
Remember primary supply to ovary = ovarian artery, which arises directly from the abdominal aorta
Secondary/minor supply = uterine artery, which branches from the internal iliac artery
Because of this dual supply, the presence of doppler flow alone does not exclude a diagnosis of ovarian torsion
Thrombosis may be seen later on
Imaging findings
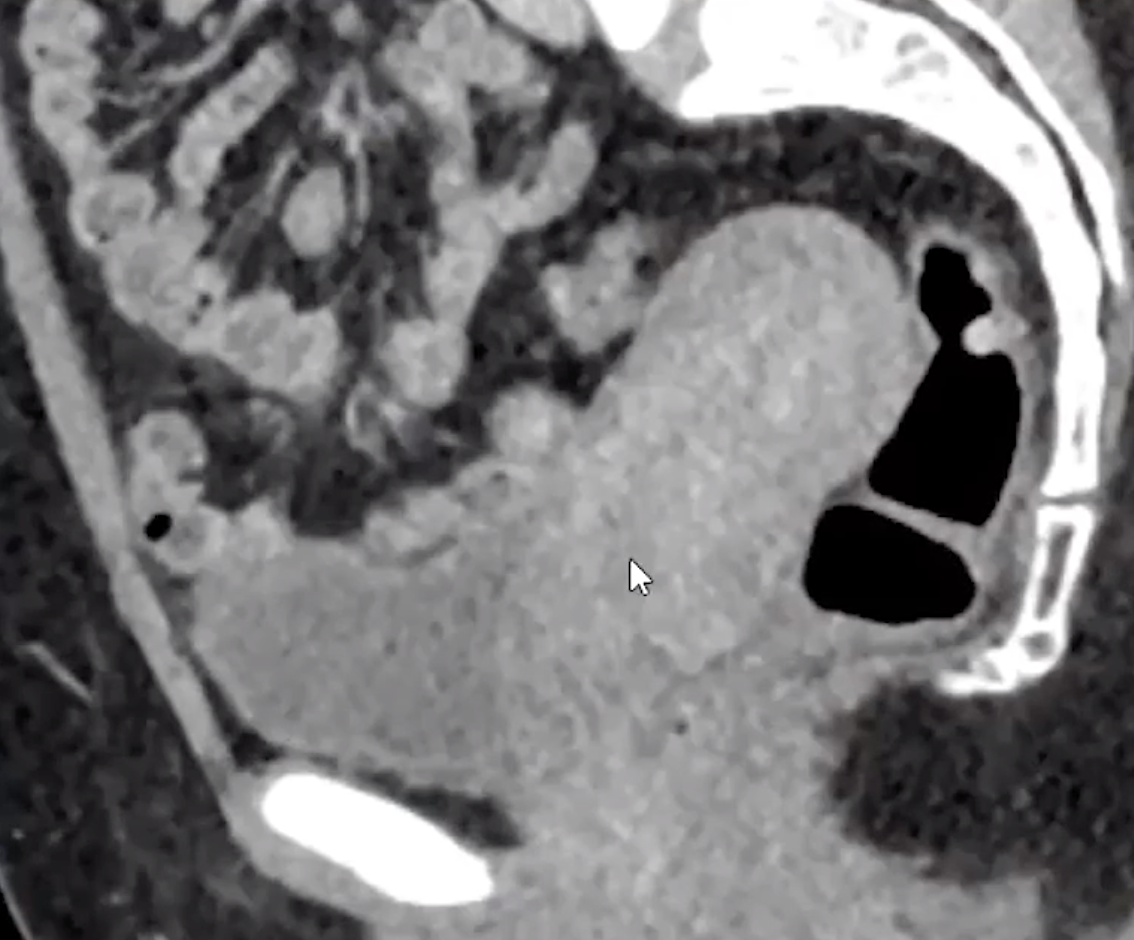
Enlarged ovary (>4 cm)
Lack of doppler flow (not required, can have torsion with flow!)
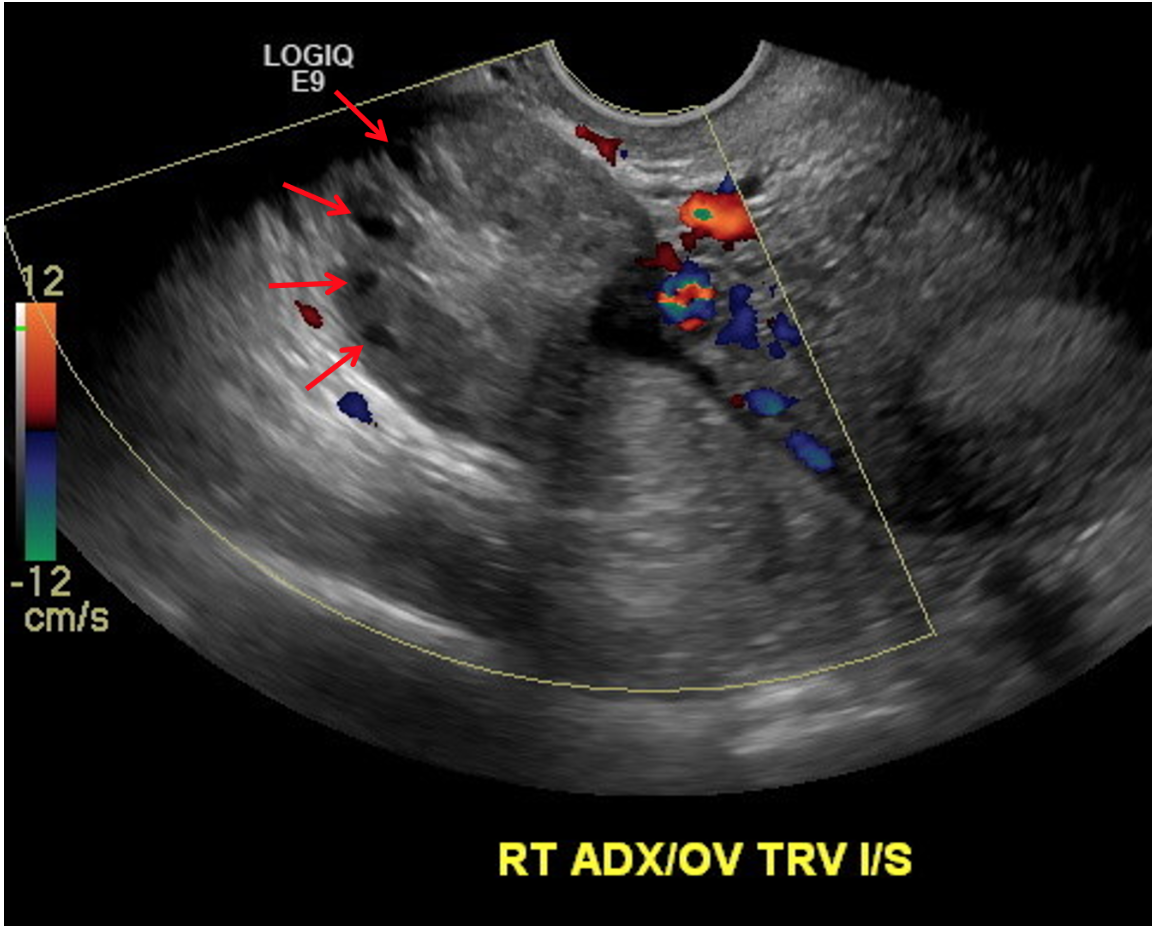
Peripheralization of ovarian follicles (also seen in PCOS)
Free pelvic fluid
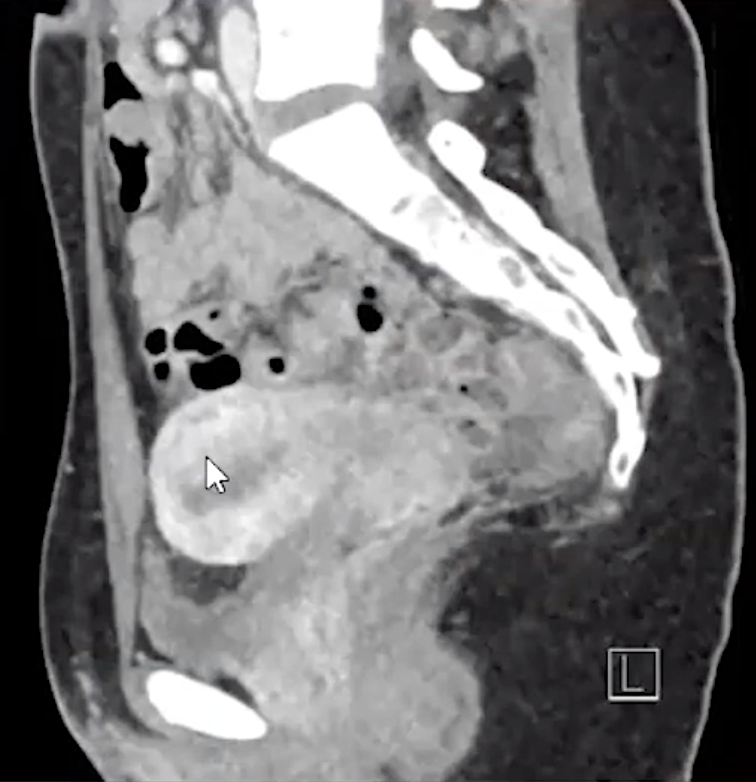
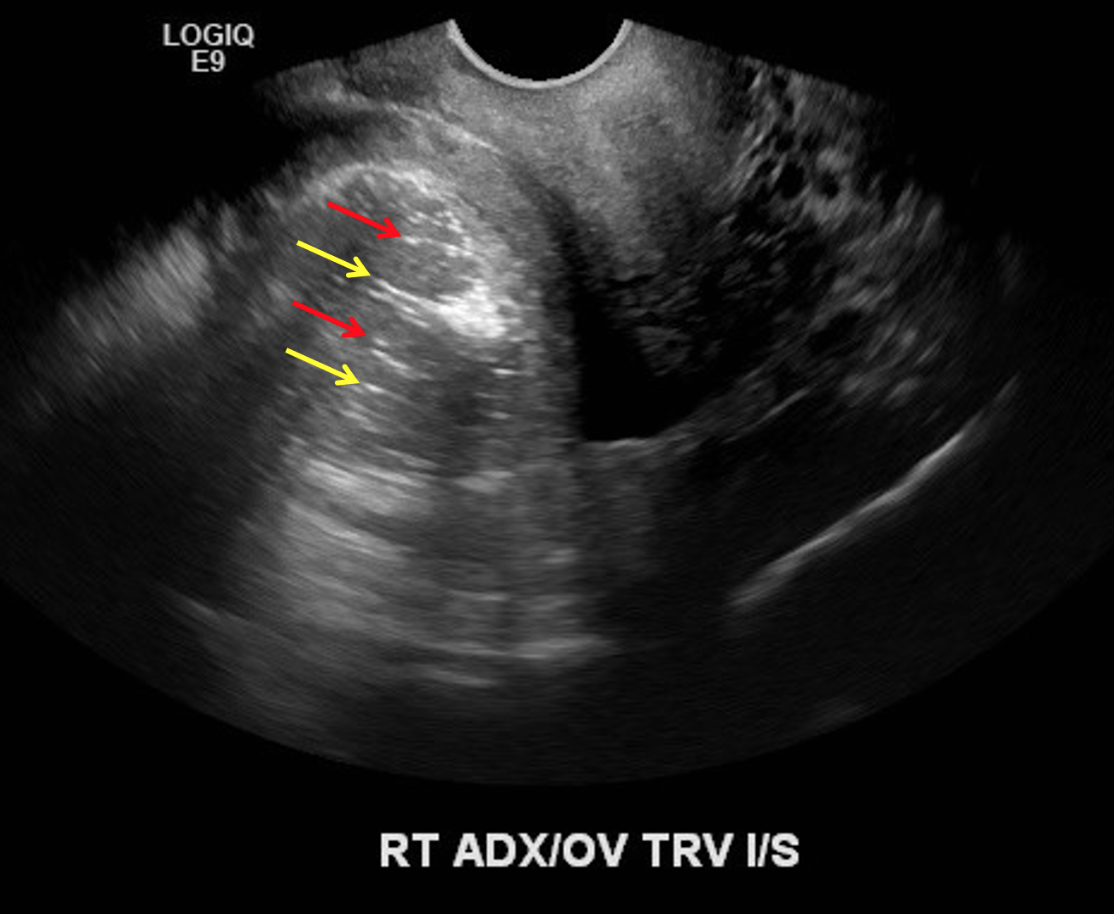
Dermoid cyst = most common mass to cause
Look for areas of increased echogenicity = fat
Look for dot-dash sign = alternating echogenic dots and dashes = represents calcifications and hair
Peripheralization of follicles and no internal doppler flow within the ovary
Flexion = Uterus
Ante-flexed uterus = uterine body located anterior toward the bladder
Retroflexed
Uterus will look like its coming from the left side of the image (normal human left) because the prob has to be placed in the posterior fornix
Dot-Dash sign seen with dermoid cysts
Ectopic Pregnancy
~95% of cases occur in fallopian tube (classically at ampulla)
Findings
No intrauterine gestational sac with correlating HCG as described below
Large volume free fluid? —> concern for rupture
Pseudogestational sac sign
Circular pocket of fluid within the endometrium may be mistaken for an early gestational sac
Note that a pseudogestational sac will demonstrate the following:
No yolk sac
Typically located centrally within the endometrial canal
May be more oval shaped with pointed edges
May contain internal debris
Tubal ring sign
Peripheral hypervascularity around the ectopic gestational sac
b-Hcg
HCG = <1500 = Not expected to be seen
HCG = 1500-2000 = Discriminatory Zone
Gray area where gestational sac really should be seen but is not definitively abnormal if not seen yet
HCG = > 2000 = Gestation sac should be seen
~100% should be seen if >3000
If gestational sac is not seen and HCG is >2000 = ectopic until proven otherwise
Note doubling rate (speed at which the HCG doubles)
Normal for HCG to double over 48 hours in early pregnancy
If HCG increases by less than 50% 48 hours —> concern for non-viable pregnancy (can be ectopic or not)
Said another way, the HCG should increase slower in non-viable pregnancy
Should recommend serial HCG if unsure
If patient got IVF and there is an intrauterine gestation and concern for ectopic, it is more likely in these patients to have concurrent viable intrauterine pregnancy and ectopic than it would be for a patient who conceived naturally
If concern for ovarian ectopic
See if ectopic and ovary move together on sine - if yes supports ectopic
If no IUP can use hcg as crutch to see if theres baby basically, but if concurrent IUP then cant really use because dont know where its coming from
Carefully evaluate the suspected gestational sac for a fetal pole or yolk sac - this is the best supporting evidence for an ectopic
References: