Neurovascular Disease
Arterio-venous malformations
Abnormal connection between artery and vein without capillary bed causing right to left shunt
Can be seen anywhere in body
Neuro AVMs
Intra-axial lesions with majority being supratentorial
Typically fed by intraparenchymal artery (note AV fistula in brain is typically by extra-parenchymal feeding artery)
Spetzler-Martin Scale
Imaging
Back flow voids on MR
Typically has minimal to no mass effect
Pulmonary AVMs
Can only be treated with coils, beads can embolize and cause stroke
Associations
Osler-Weber Rendu (Hemorrhagic Hereditary Telangiectasia)
Hyperdense vessel
When vessel appears hyperdense (brighter) compared to background brain parenchyma on CT
Differential
Acute stroke with intraluminal thrombus (most common)
Polycythemia
Normal blood (normal blood in vessels is slightly hyperdense relative to normal brain parenchyma)
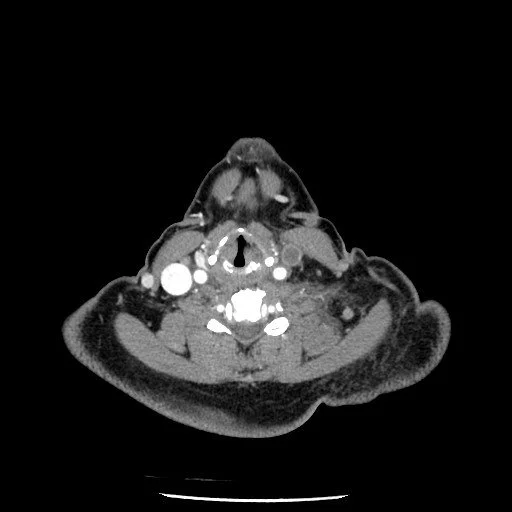
Lemierre Syndrome
Thrombophlebitis of internal jugular vein secondary to bacterial infection typically from pharyngitis
Presents few days after pharyngitis with trismus
Can cause septic emboli and abscess formation
>80% of cases associated with gram neg bacillus, usually Fusobacterium necrophorum
Posterior Reversible Encephalopathy Syndrome (PRES)
Basically posterior circulation is not able to respond to changes in blood pressure and symptoms result
Associated with high blood pressure (may seen in eclampsia/pregnancy)
Can also be seen with chemo use - specifically cisplatin and cyclosporine
Vision issues (hence posterior) and encephalopathy
Imaging Findings
Bilateral vasogenic edema of occipital & parietal lobes
T1 hypo, T2 hyper
Everything is vague - may restrict/but also may not, may enhance/ but also may not, may have microhemorrhages/ but also may not
MRA - vessel irregularities, vasoconstriction
Treatment - treat underlying cause, manage BP
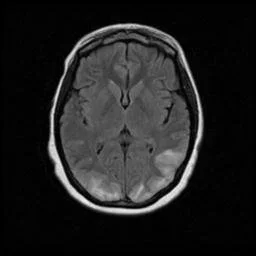
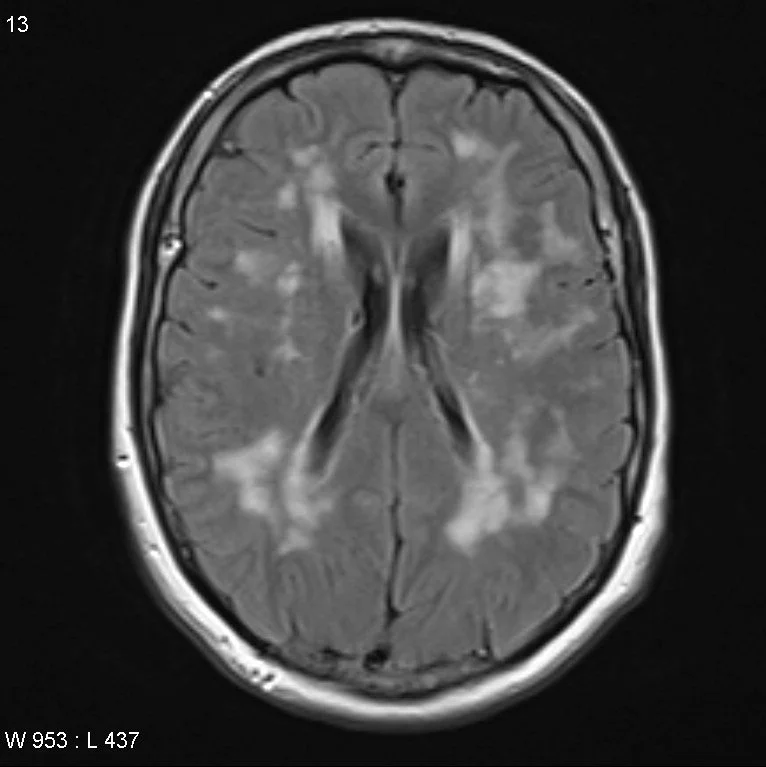
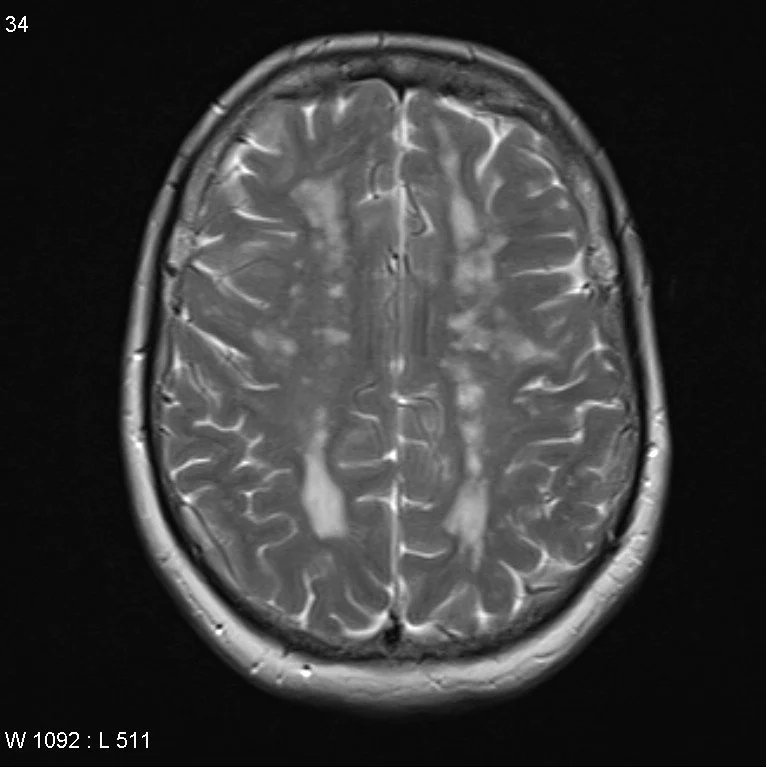
Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL)
Autosomal dominant mutation in NOTCH 3 gene causing vasculopathy which results in recurrent ischemic infarcts and eventually vascular dementia
This is basically early onset multi-infarct dementia
Presentation
Migraines
Recurrent TIA/stroke
Early onset dementia
Psychosis
Other vague non-specific neuro issues
Age 30-50 = TOO YOUNG FOR DEMENTIA AND RECURRENT STROKES
Imaging
Confluent white matter T2 hyperintensities
Temporal lobe and external capsule are classic locations
Occipital lobe and cortex are typically spared
Cortical Vein Thrombosis
Thrombosis of the superficial veins
Clinically relevant cortical veins:
Superficial middle cerebral vein
Inferior anatomotic vein (vein of Labbe)
Superior anastomotic vein (vein of Trolard)
Cord sign - hyperdense vein on non-con CT (commonly transverse sinus) (same shit as hyperdense vessel sign, just a venous structure)
Typically occurs with dural or deep cerebral vein thrombosis, very rarely can occur alone
Juvenile Angiofibroma
Males 10-25 years old
Primary arterial supply —> internal maxillary artery, a branch off of the external carotid artery
Complete surgical resection recommended, commonly with pre-surgical embolization to decrease blood loss during surgery
Capillary Telangiectasia
Seen with osler-weber-rendu
Classically seen after radiation treatment to the head
Looks like amyloid angiopathy on the SWI but in someone younger who shouldn’t have amyloid at that age
Vertebrobasilar Dolichoectasia
References:
Case courtesy of Safwat Mohammad Almoghazy, Radiopaedia.org, rID: 86127 (lemierre syndrome)
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 22131 (CADASIL)