Neurocutaneous Disorders
Tuberous Sclerosis
Autosomal dominant Mutation in TSC1 or TSC2
Cutaneous findings
Ash-leaf spots
Malar angiofibromas
Shagreen patch
Neurologic findings
Sub-ependymal nodules - nodules in lining of ventricles
Sub-ependymal giant cell astrocytoma - mass at inter-ventricular foramen
Mass near foramen of monro in a patient with suspected TS = SEGA
Can cause hydrocephalus and increased ICP
Cortical tubers
Seizures, intellectual disability, autism, behavior issues
Cardiac rhabdomyomas (RC)
Renal angiomyolipomas (RA)
Radial Bands Sign (RB)
How to Remember - RA + RB + RC + TC + sub-ependymal giant cell astrocytoma
Cortical Tubers
Benign hamartomas
Triangular shaped lesion
80% are in frontal lobe
T1: low signal,
T2/FLAIR: high signal
Can be iso-intense in neonatal period
Enhancement is rare
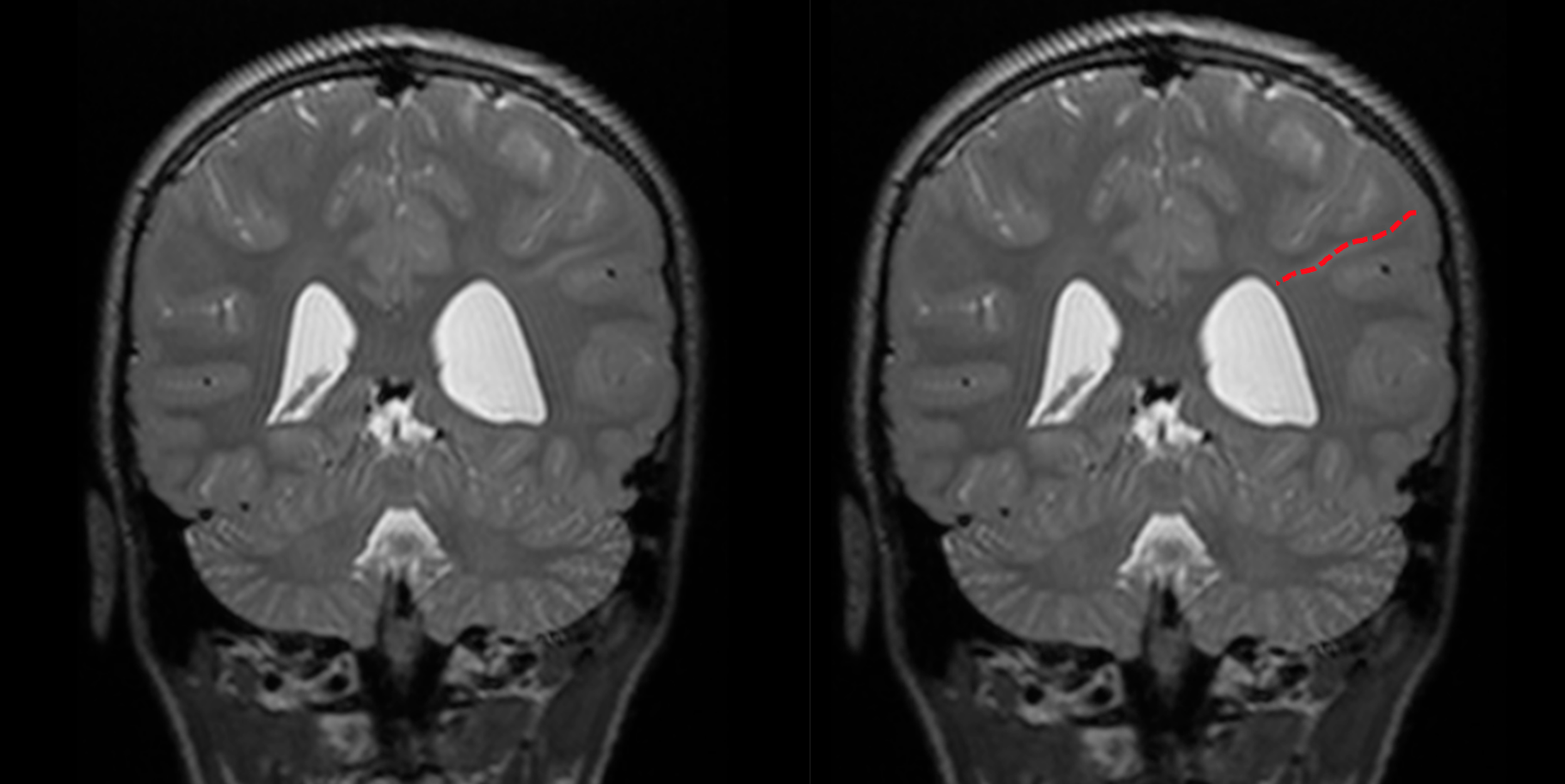
Radial Bands sign
Linear bands radiating from periventricular white matter to the subcortical region
MRI finding specific for Tuberous Sclerosis
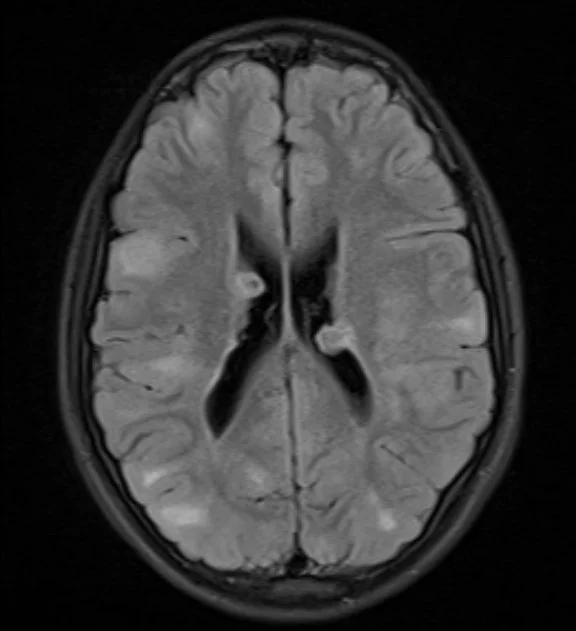
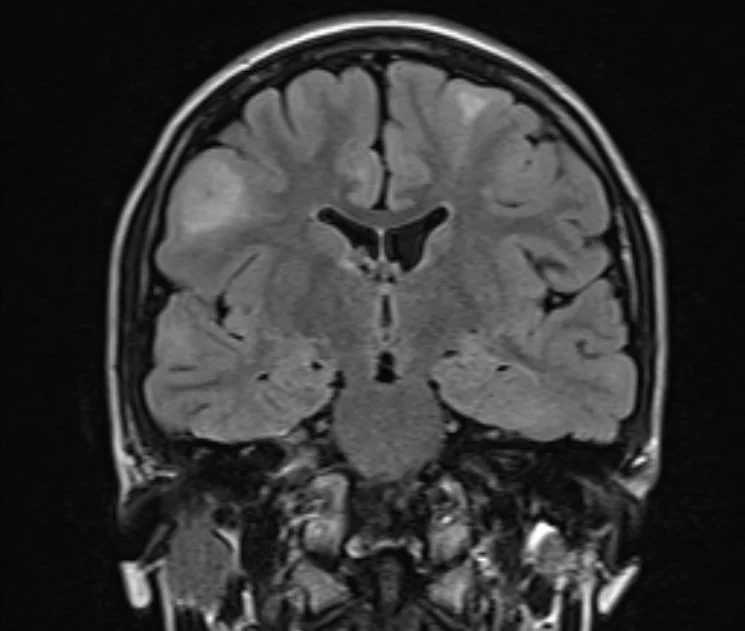
FLAIR:
Showing obvious ventricular lesions which are iso-intense on T2 and FLAIR and demonstrate heterogeneous enhancement. This is a sub-ependymal hamartoma.
Multiple hyper-intense subcortical (peripheral) lesions. These are cortical tubers.
Encephalocraniocutaneous lipomatosis (Haberland syndrome)
Multiple weird findings all put together - multiple associations and stuff, id just know that this exists and what it is composed of
Nevus psiloliparus
Scalp alopecia with underlying lipomatous hamartoma
Intracranial and intradural spinal lipoma
Periorbital tumors
Jaw tumors
Coarctation of aorta
Neurocutaneous Melanosis
Leptomeningeal melanosis + cutaneous nevi
Increased T1 & Decreased T2 signal in the bilateral amygdalae
Makes sense because melanin is T1 bright
Neurosarcoidosis
Affects meninges
Affects optic nerves and hypothalamus
NF-1
Optic nerve glioma, classically pilocytic astrocytomas of optic nerve
Anterior-medial tibial bowing
Lateral meningoceles
Renal vascular stenosis
Sphenoid dysplasia
Affects optic nerves and hypothalamus
Plexiform neurofibromas
Random areas of hyperintensity, classically of basal ganglia
Represents areas of vacuolization
Tend to wax and wane and go away by adulthood
Tuberous Sclerosis
Subependymal nodules
T1 hyper, T2 hypo
Cortical tubers
T2 hyper
SEGA
Intraventricular tumor
AML of kidney
LAM
Cowden Syndrome
Hamartomas (typically GI)
Breast cancer
L’hermitte duclos
Cerebellar mass with striated/corduroy appearance
Leigh Syndrome
aka Subacute necrotizing encephalomyelopathy
Progressive neurodegeneration —> death in kids
Random neurologic symptoms
Scattered T2 hyperintensities classically in basal ganglia and brainstem
NF-2 (MISME)
Schwanomas
Meningiomas
Ependymomas
Does not have neurofibromas
VHL
Hemangioblastomas of brain and spine
Endolymphatic sac tumor
Abdominal masses
Bilateral RCC - clear cell
Pheochromocytoma
Pancreatic tumors
islet cell tumors, serous cystadenomas, regular cysts
Mitochondrial Disorders
Kearns-Sayre Syndrome
Triad of
Symptom onset <20 years old
Pigmented retinopathy
Chronic progressive external opthalmoplegia (CPEO)
Subcortical T2 hyperintensities and calcifications
References:
Case courtesy of Bouhouche Abdeldjalil, Radiopaedia.org, rID: 172673 (radial bands sign)
Case courtesy of Mostafa Elfeky, Radiopaedia.org, rID: 56513 (TSC images)