Demyelinating Disease
Conditions Discusses
Marchiafava Bignami
ADEM
PML
PRESS
CDIP
Neuromyelitis Optica
Multiple Sclerosis
Central Pontine Myelinolysis
Marchiafava Bignami
Demyelination of corpus callosum, most commonly secondary to alcoholism (M-B was an alcoholic to remember)
Nonspecific presentation
Imaging findings
Hyperintense corpus callosum (looks like it crosses midline but not masslike)
Starts in body of CC —> genu —> splenium (typically spares posterior aspect until late)
Affects central fibers and spares the dorsal and ventral fibers
So prefers center
Center of CC (body), and central fibers
T2 hyperintensities within the corpus callosum, T1 hyperintensities
Sandwich sign - central layers of corpus callosum affected first which will be T2/FLAIR hyperintennse, so you will have peripheral areas of hypo-intensity with a middle layer which is hyperintense and resembled a sandwich or just stripes I suppose
Acute Disseminated Encephalomyelitis (ADEM)
Acute inflammation and demyelination of white matter
Seen after viral infection or recent vaccination due to immune cross reaction, anti-MOG (myelin oligodendrocyte glycoprotein) IgG may be positive
Imaging findings are typically identical to MS
Full recovery common, sometimes persistent neuro deficits
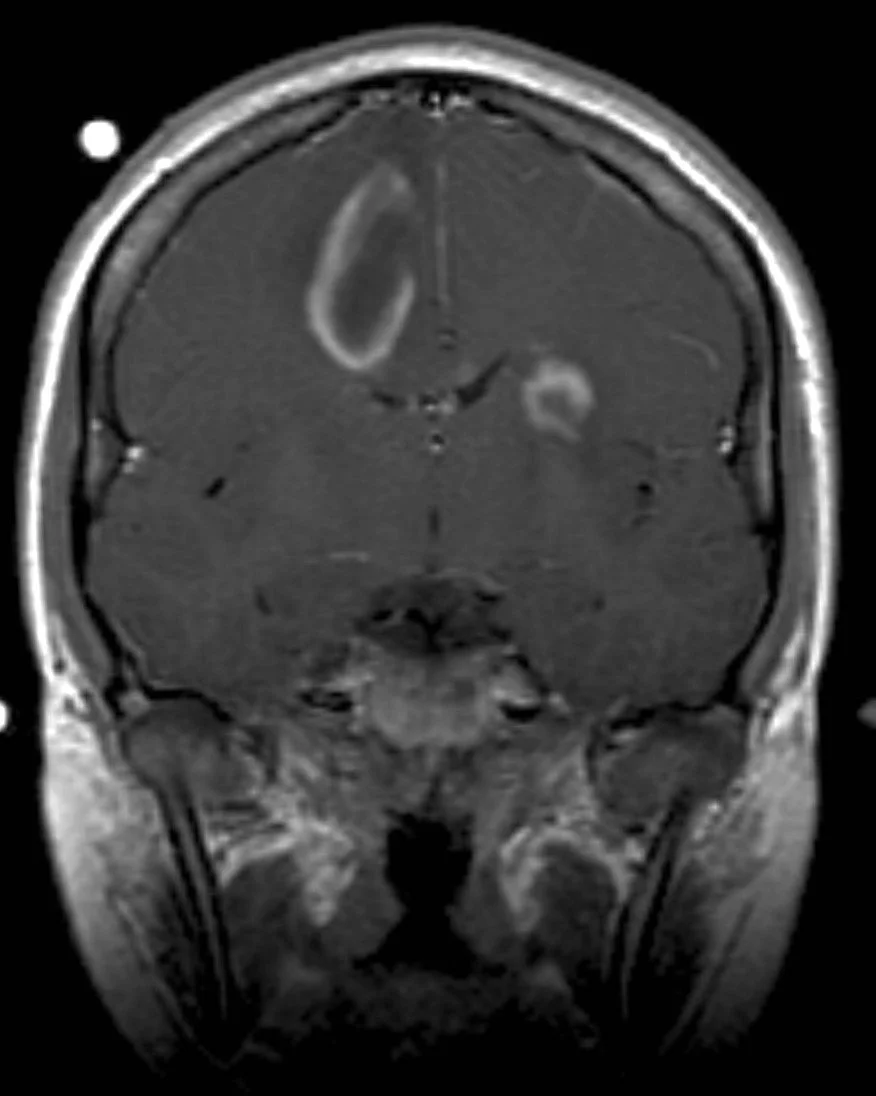
Imaging findings
Incomplete ring enhancing lesion
Typically large lesion (especially compared to MS)
Typically has surrounding edema - remember this is from acute demyelination from vaccination/viral illness so almost like a brain infection that is being self attacked so edema should be easy to remember
Asymmetric lesions
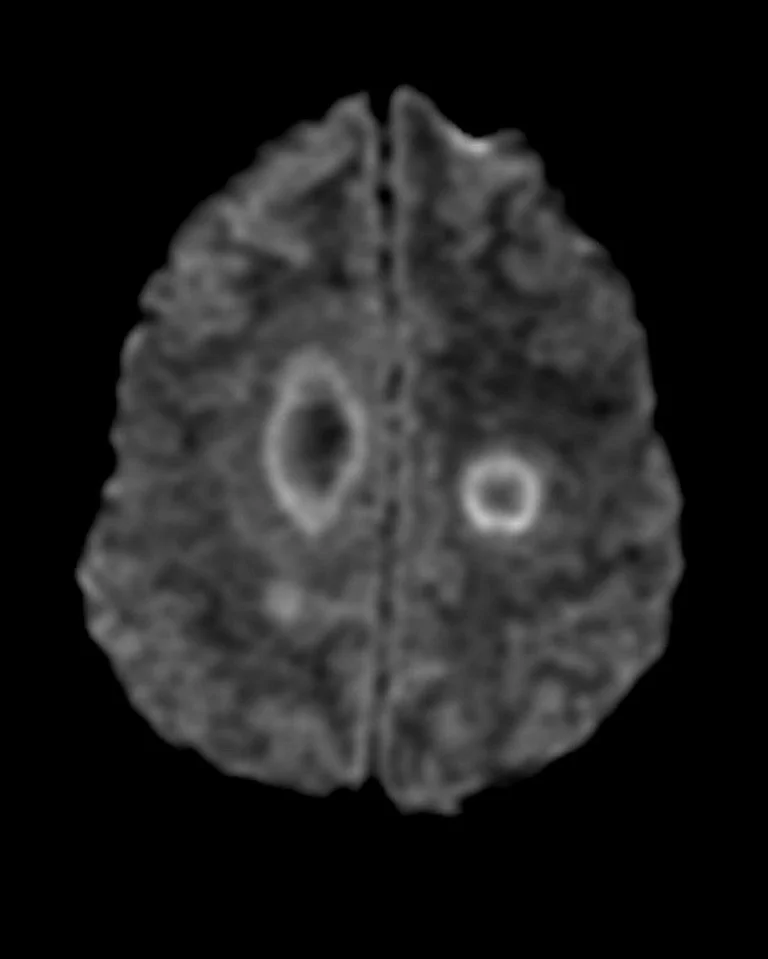
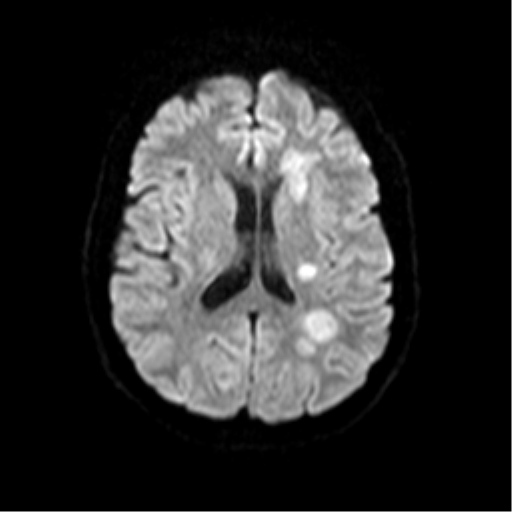
DWI - peripheral restricted diffusion but not centrally
Hurst variant (acute hemorrhagic leukoencephalitis) - rapidly progressive form with death within days
T2 hyperintensities + multiple hematomas
Open ring sign
DWI showing peripheral restriction without central restriction
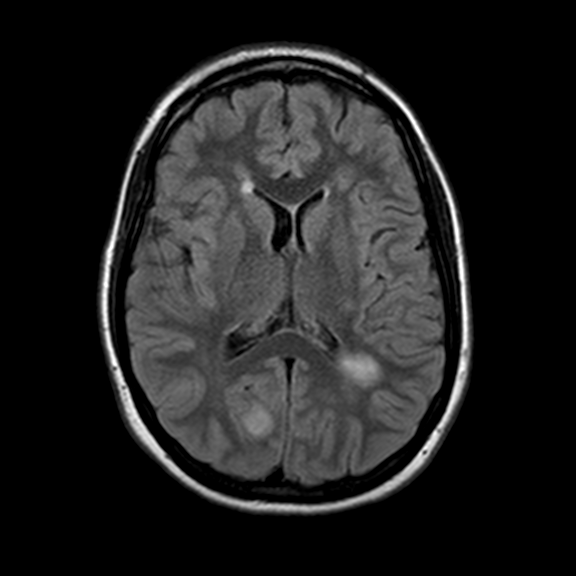
Bilateral asymmetric FLAIR hyperintensities
Peripehral open ring restriction on DWI not always seen as evidenced below
Progressive Multifocal Leukoencephalopathy (PML)
Demyelination after reactivation of JC virus which infects oligodendrocytes
Seen in immunocompromised patients (AIDS < 200 CD4)
Imaging findings
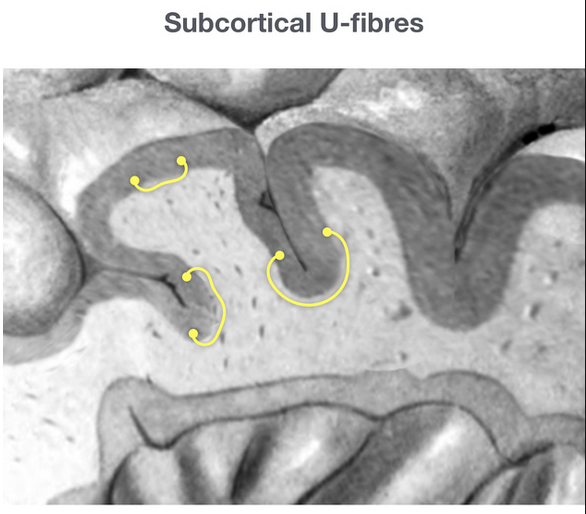
Asymmetric, multi-focal, bilateral lesions - really anywhere but key place is subcortical U fibers
T1: hypointense
T2: hyperintense
No enhancement on contrasted studies
Patchy areas of restricted diffusion
Milky way sign - multiple clustered punctate T2 hyperintense lesion (not to be confused with galaxy sign!)
Eh, not sure i really see this one, and no great examples online
Barbell sign - parieto-occipital lesions which crosses the splenium
Shrimp sign - T2 hyperintensity of the cerebellar white matter but which spares the dentate nucleus
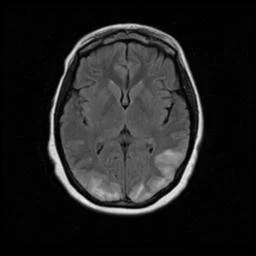
Barbell sign
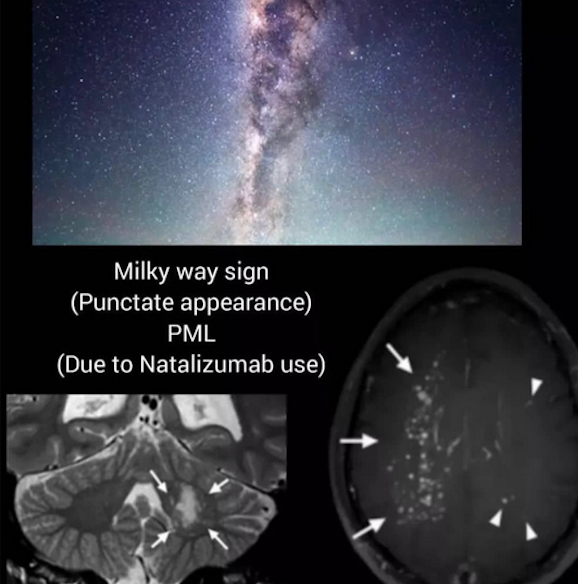
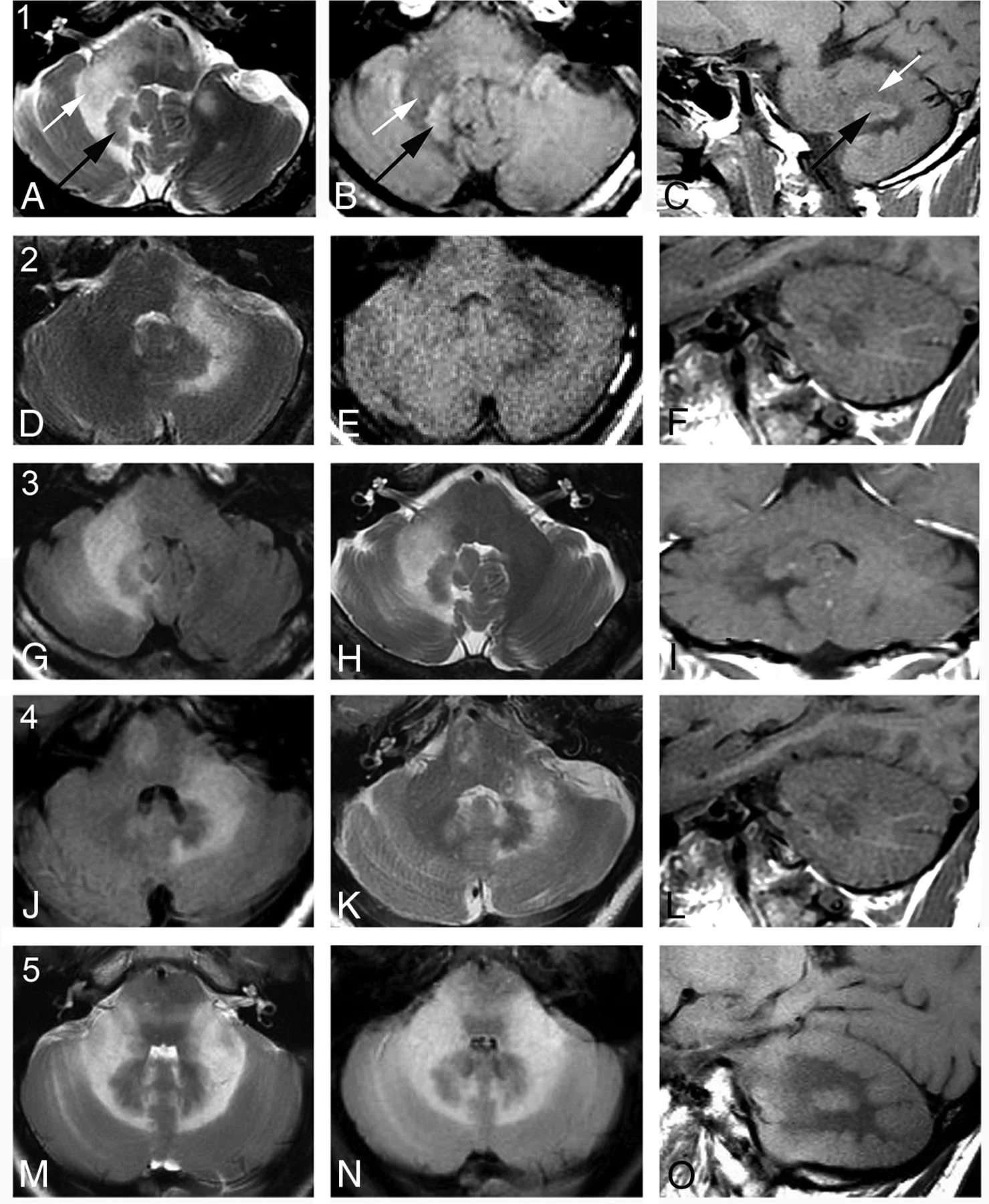
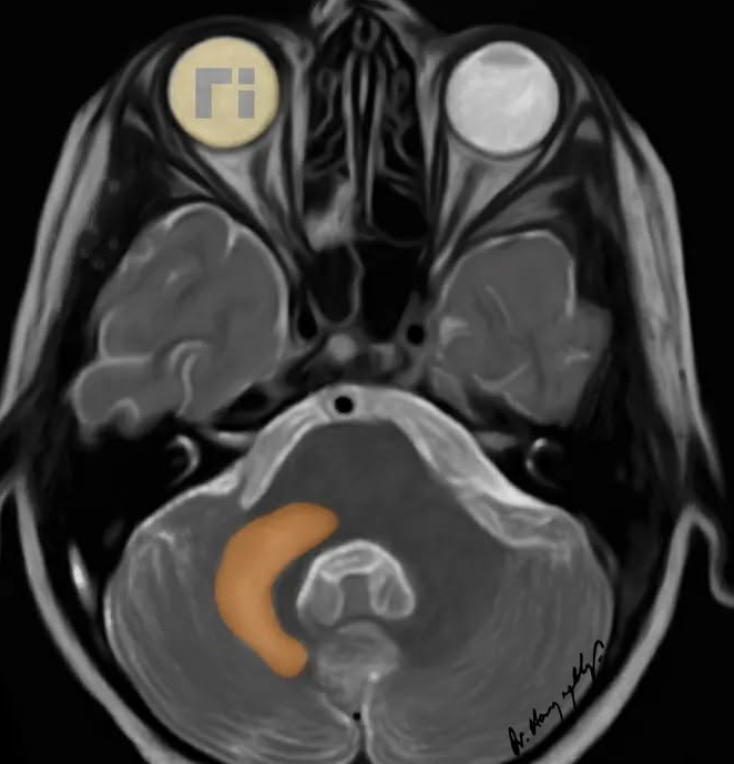
Image showing abnormally hyperintense dentate nuclei.
Note: This image is not PML it just shows anatomy of dentate nuclei well since they are so abnormally bright here,
Posterior Reversible Encephalopathy Syndrome
Basically posterior circulation is not able to respond to changes in blood pressure and symptoms result
Associations
High blood pressure (may seen in eclampsia/pregnancy)
Pregnancy
Chemotherapy use
Vision issues (hence posterior) and encephalopathy
Imaging Findings
Bilateral - asymmetric - posterior lesions
Lesions typically of cortex and subcortical white matter
T1 hypo, T2 hyper
Everything is vague - may restrict/but also may not, may enhance/ but also may not, may have microhemorrhages/ but also may not
MRA - vessel irregularities, vasoconstriction
May have vasogenic edema
Treatment - treat underlying cause, manage BP
Chronic Demyelinating Inflammatory Polyneuropathy (CDIP)
Affects spinal nerves
Repeated demyelination and remyelination leads to concentric rings looking like onion bulb
Neuromyelitis Optica (Devic Disease)
Triad
Abs to aquaporin-4
Bilateral optic nerve disease
T2 hyper, enhancing
Long segment spinal cord myelitis
T1 hypo, T2 hyper, enhancing
Does not affect the brain (well it can, but textbook is not to)
Multiple Sclerosis
Demyelinating disease
Lesions
Many different types
Can restrict diffusion in ACUTE phase
Perpendicular to the corpus callosum - dawson fingers
Involvement of callosal-septal interface is HIGHLY specific
Infratentorial plaque - very rare (although may be seen in kids)
Lesions will change location with time
If occurs in the cord will be short segment demyelination (1-2 vertebral bodies long)
Relationship with EBV
What looks similar
Vasculitis
Typically spares callosal-septal interface
Tends to preferentially affect basal ganglia
Lymes disease
Classically causes cranial nerve enhancement
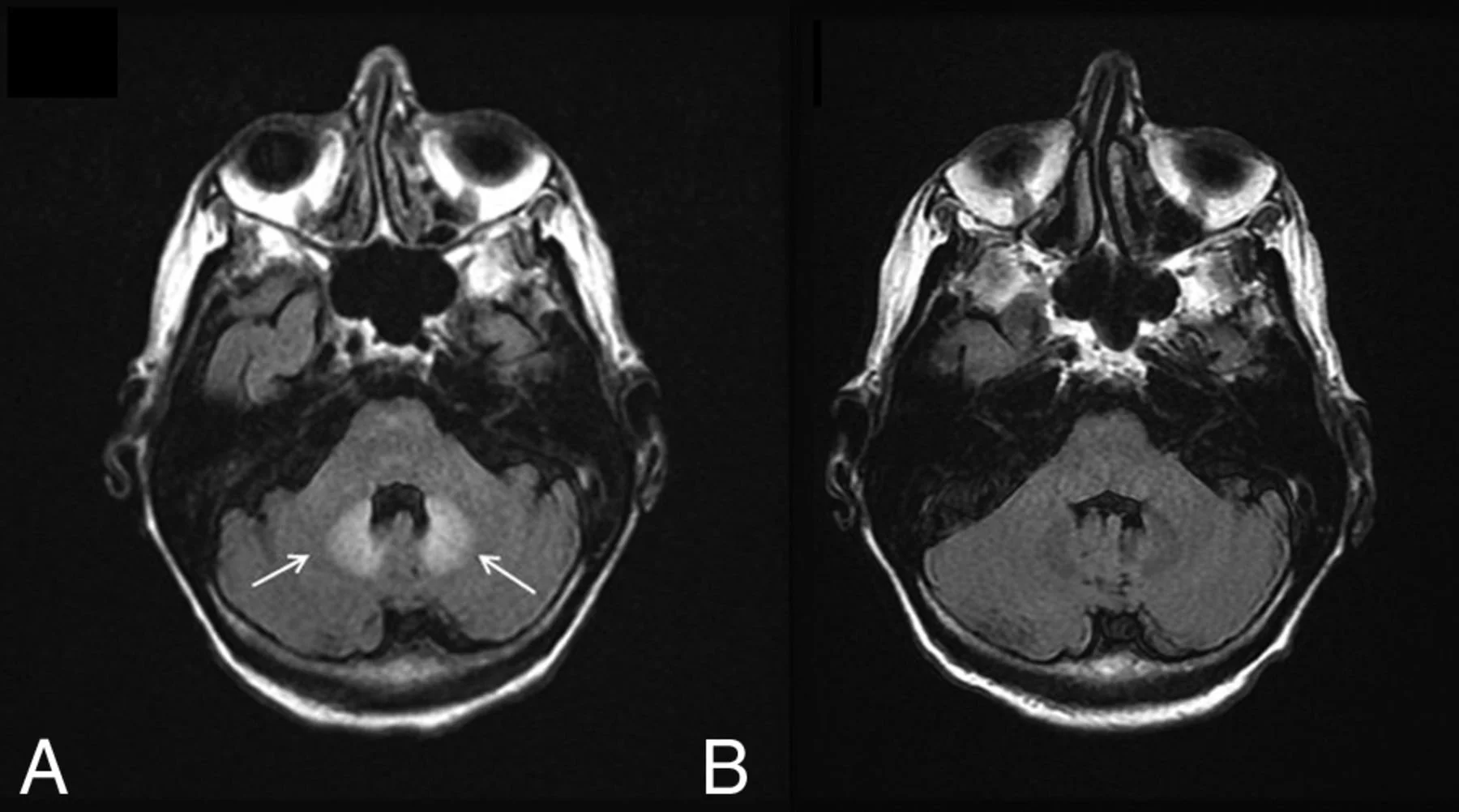
Central Pontine Myelinolysis
Location is key to diagnosis - look for lesion at center of pons
Seen with rapidly corrected hyponatremia
Almost always will see restricted diffusion
Central Pontine Myelinolysis
Location is key to diagnosis - look for lesion at center of pons
Seen with rapidly corrected hyponatremia
Almost always will see restricted diffusion
References:
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 2576 (ADEM)
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 39817 (ADEM)
Case courtesy of Arthur Daire, Radiopaedia.org, rID: 31030 (PML)
N. Adra, A.E. Goodheart, O. Rapalino, P. Caruso, S.S. Mukerji, R.G. González, N. Venna, J.D. Schmahmann, MRI Shrimp Sign in Cerebellar Progressive Multifocal Leukoencephalopathy: Description and Validation of a Novel Observation American Journal of Neuroradiology May 2021, DOI: 10.3174/ajnr.A7145 (PML shrimp)
K.M. Bond, W. Brinjikji, L.J. Eckel, D.F. Kallmes, R.J. McDonald, C.M. Carr, Dentate Update: Imaging Features of Entities That Affect the Dentate Nucleus, American Journal of Neuroradiology Aug 2017, 38 (8) 1467-1474; DOI: 10.3174/ajnr.A5138 (dentate nuclei)
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 58883 (subcortical U fibers)
Case courtesy of Paul Simkin, Radiopaedia.org, rID: 30476 (PRES)