Pediatric Neuro
Pediatric Brain has different myelination pattern
Only myelinated structures at birth
Brainstem
Posterior limb of internal capsule
T1 should have normal adult pattern at age 1
T2 should have normal adult pattern at age 2
Opercularization = closure of the sylvian fissure
Has nothing to do with myelination just listed here
Sylvian fissure will be wide angled open at infancy and more narrow as you get older
Chiari 2
Myelomeningocele is present at birth and creates a suction on the CSF that then pulls the cerebellar tonsils down ward (how i think about it)
Therefore once the myelomeningocele is repaired surgically the patient will typically develop hydrocephalus because the vaccuum is gone and the body had gotten used to it and compensated accordingly
Concurrent findings
Dysgenesis of corpus callosum
Tectal beaking
Elongation of 4th ventricle
Stenogyria
Large mass intermedia
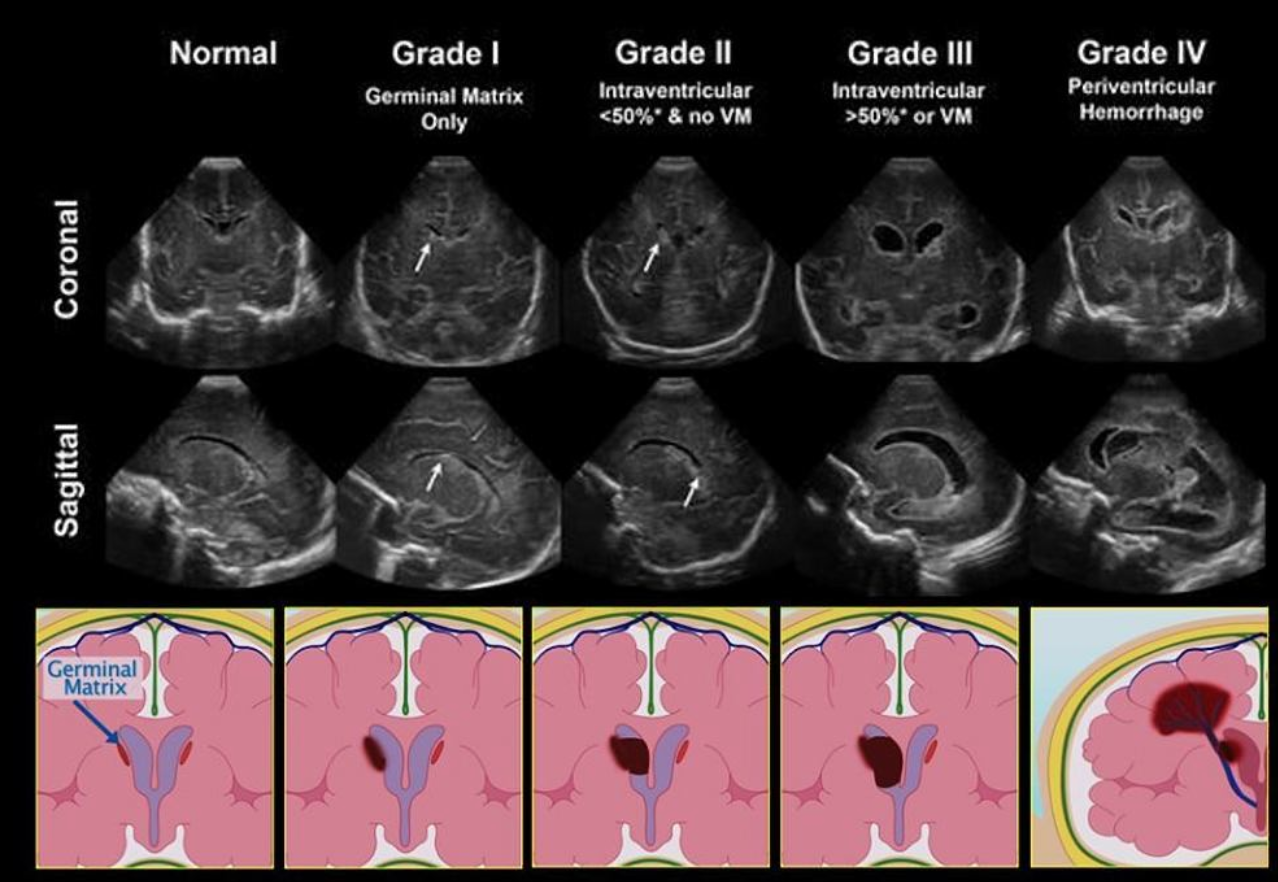
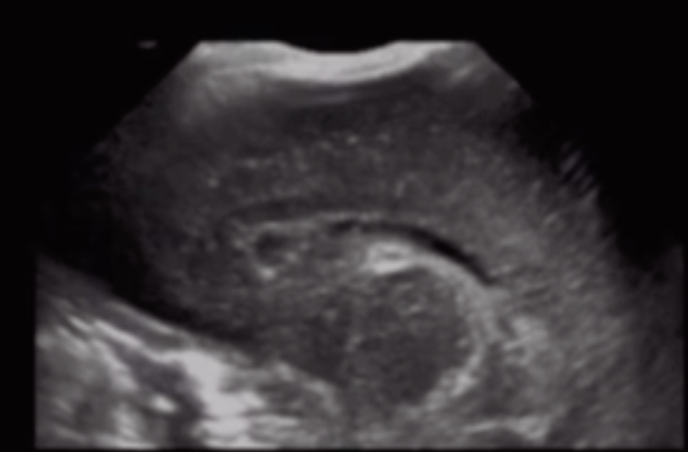
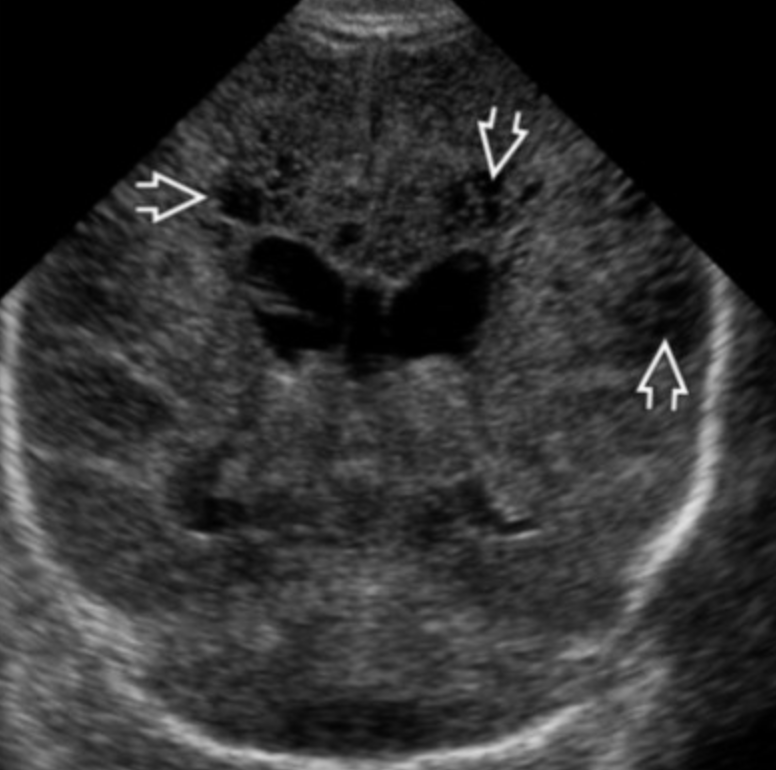
Germinal Matrix Hemorrhage
The choroid plexus should not extend past the caudothalamic groove
If you see bright stuff near there then suspect it is blood
Only seen until 32-34W gestation
You cannot have germinal matrix hemorrhage in a full term infant
There is normally some increased echogenicity in the periventricular white matter
So how do we know what is blood vs normal brain
If prominently asymmetric = likely blood
If area of increased echogenicity is as echogenic or more echogenic as the choroid plexus = likely blood
Normal peri-ventricular brain should be echogenic but not more than the choroid plexus
Can you identify borders of the echogenic area
If yes = likely blood
Normal brain will be more vague
Relevance of Grading
If grade 1 = can continue anti-coagulation (kids classically on AC for ECMO)
If grade 2 or higher = typically need to stop AC and therefore stop ECMO
Grading
Grade 1: Sub-ependymal hemorrhage
Can progress to grade 2
Can resolve or sometimes form a subependymal cyst
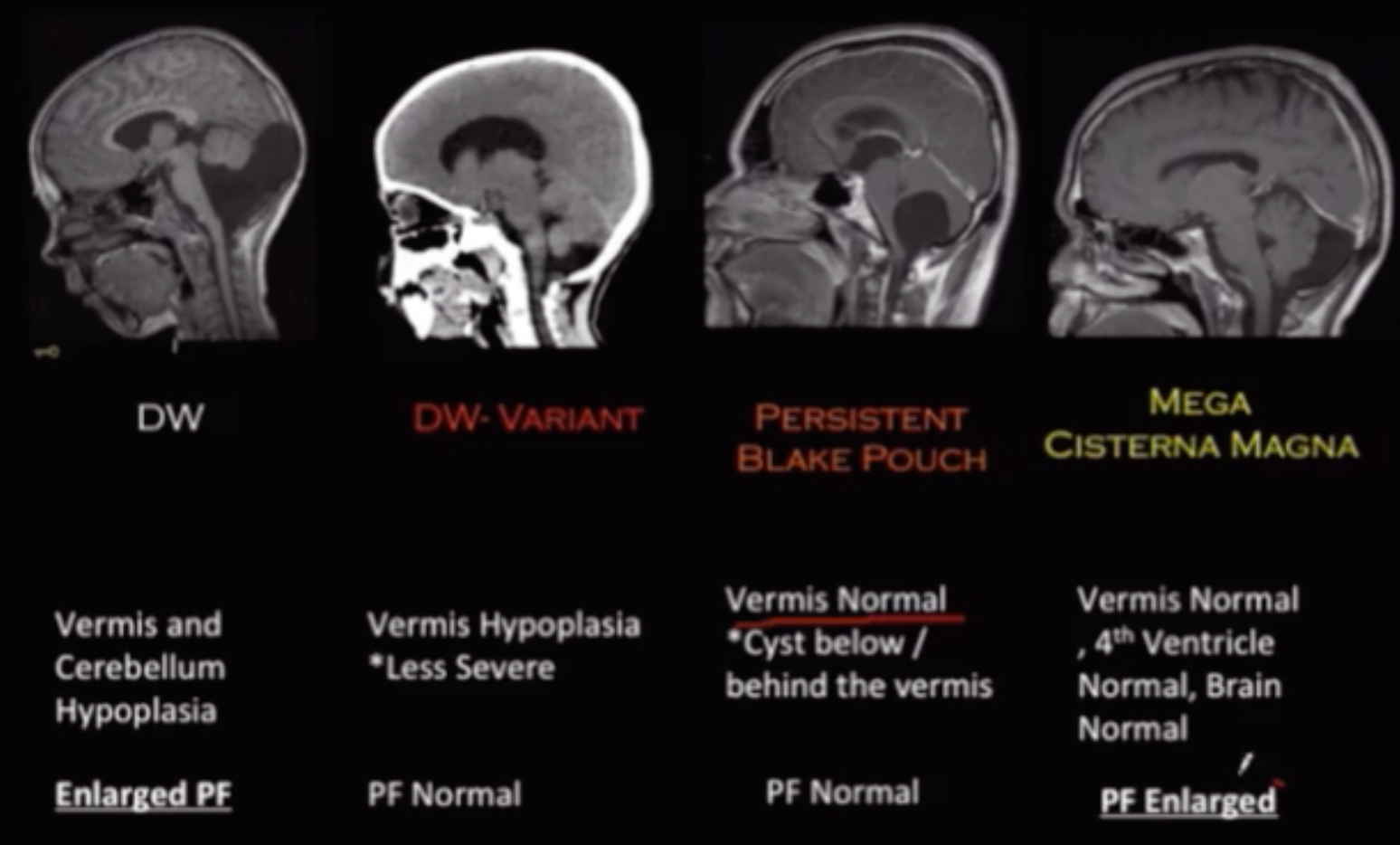
Dandy-Walker Malformation
Hypoplastic cerebellar vermis
Cystic dilation of the 4th ventricle
Torcular-lambdoid inversion - basically torcula gets pushed superiorly by the cystic shit and makes it higher than normal
Torcula = confluence of sinuses
Lambdoid = lambdoid suture
Associated with almost everything to some degree
Technically exists on a spectrum for cases that are basically DW but don’t meet all the criteria - termed Dandy walker variant
Meckel-Greuber Syndrome
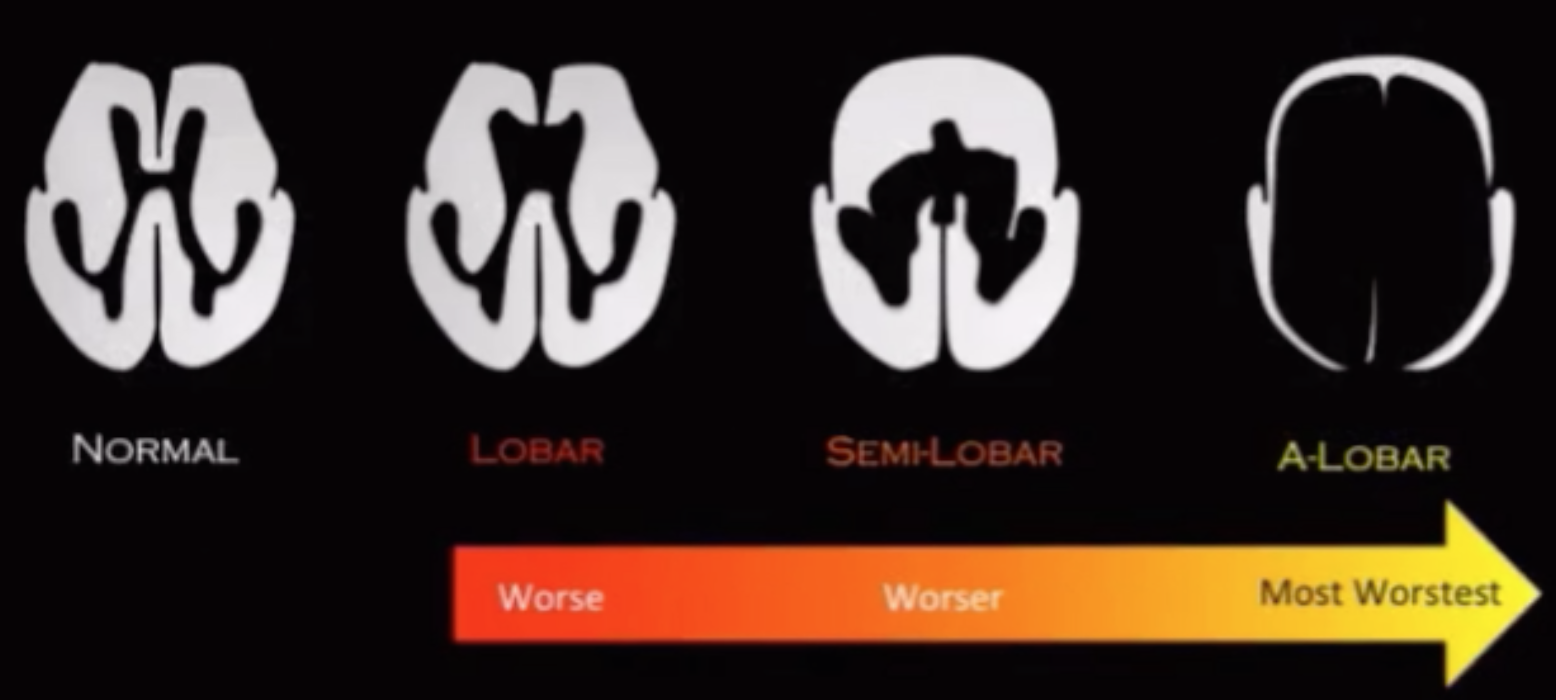
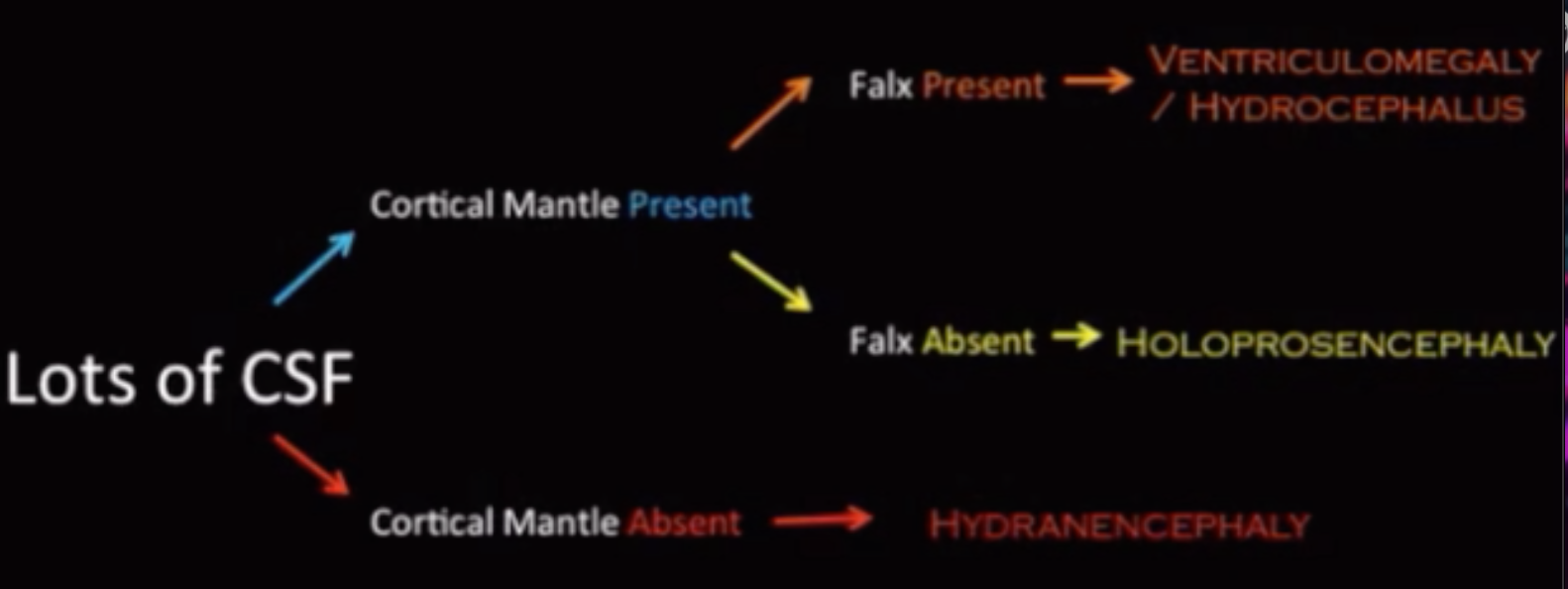
Holoprosencephaly
Renal cysts
Polydactyly
Blake’s Pouch Cyst
Failure of Blake’s pouch to regress because the foramen of Magendie does not open in development
Therefore no communication between 4th ventricle and cisterna magna
Remember magendie = allows 4th ventricle to drain into cisterna magna
Remember lushka = allows 4th ventricle to drain into cerebellopontine cistern
Hydrocephalus present (Arachnoid cyst will not have hydrocephalus)
Normal torcula (confluence of sinuses)
No cerebellar vermis malformations (DW will have these)
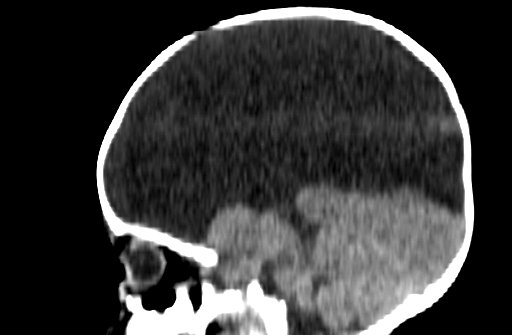
Hydrancephaly
Destruction of cerebral hemispheres and replaced with fluid
Basically bilateral large MCA infarcts
Absence (may have some small residual tissue) of the cerebral hemispheres
The thalami and posterior fossa are typically preserved
Falx typically present -it is an infarct not midline cleavage issue!
DDx - severe hydrocephalus, L1CAM disease, oters

The “Cephalys”
Lissencephaly
Incomplete separation of the two cerebral hemispheres
Holoprosencephaly
Incomplete separation of the two cerebral hemispheres
Lobar
Least severe
Thalami not fused
Absent septum pellucidum
Fusion of frontal horn of lateral ventricles
Inter-hemispheric fissure present
Normal/hypoplastic corpus callosum
Semilobar
Middle severity
Partially fused thalami
Absent septum pellucidum
Monoventricle - one weird shaped ventricle
Incomplete inter-hemispheric fissure
Agenesis/hypoplastic corpus callosum
Incomplete falx
Fusion of anterior part of cerebral hemispheres
Olfactory tracts are gone
Septo-Optic Dysplasia
Mildest form of holoprosencephaly
Small optic nerves
Associated with pituitary dysfunctions (midline structure again)
Hemi-megalencephly
Basically asymmetric enlargement of one cerebral hemisphere
Big brain parenchyma + big ventricle
If this was small side + big ventricle = atrophy (rasmussen encephalitis)
Can have focal or diffuse neuronal migration defects
Polymicrogyra
Pachygyra
Heterotopia
Gray matter heterotopia
Disruption of migration of gray matter from the ventricle to the cortex
Nodular form
Most common type
Basically gray matter clump next to lateral ventricles
Look for ragged borders of the lateral ventricles or focal plump masslike lesion with gray matter signal in the lateral ventricles
Diffuse form
Schizencephaly
Gray matter lines cleft in the brain
Open lip
the cleft walls are separated and filled with CSF
most common form in bilateral cases
Closed lip
the cleft walls are in apposition
most common form in unilateral cases
Associated with
Absent septum pellucidum
Heterotopic gray matter
Dysgenesis of CC
Alobar
Most severe
Fused thalami
Absent septum pellucidum
Monoventricle
Absent inter-hemispheric fissure
Absent corpus callosum
MCA & ACA replaced by tangled vessels
Severe facial malformations
Looks like huge cyst in skull with little brain tissue
Lissencephaly-Pachygyra Spectrum
Lissencephaly
Smooth brain surface
Type 1
Something about Miller-Dieker syndrome
Type 2
Cobblestone
Polymicrogyra
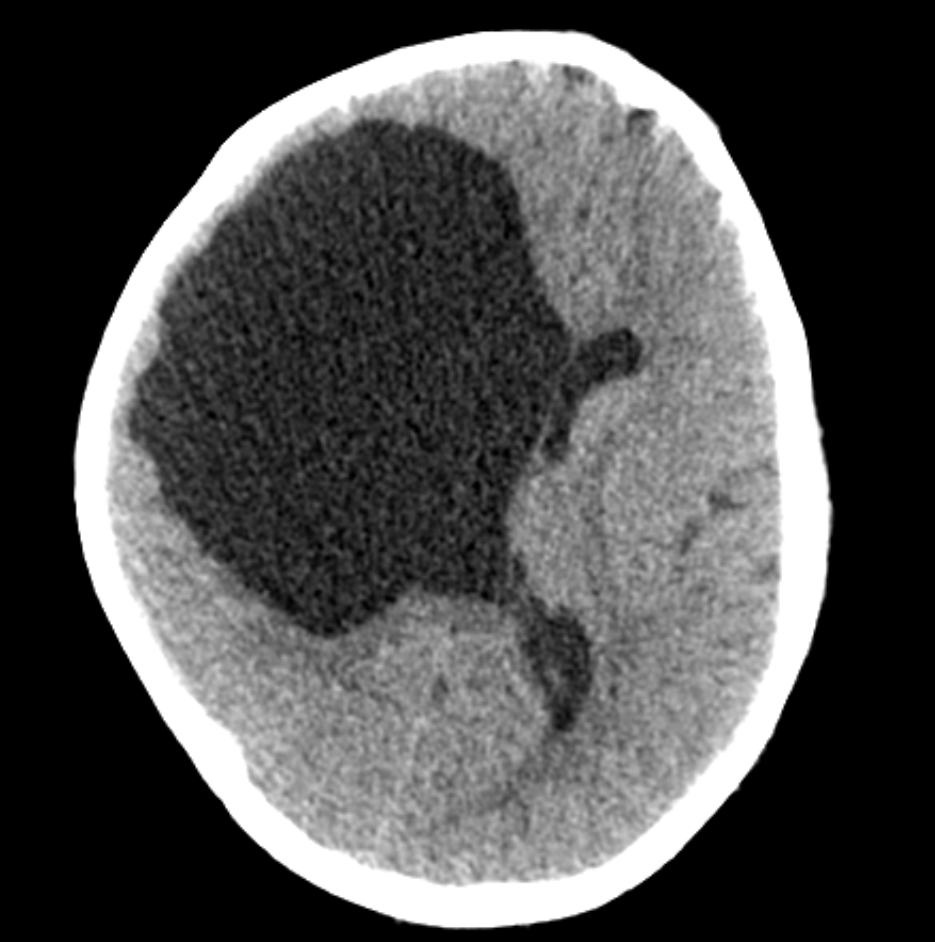
Porencephaly/Porencephalic Cyst
Considered less severe form of hydrancephaly
Agenesis of the Corpus Callosum
Corpus callosum formation
Forms from front to back
Rostrum is last thing to form
Partial agenesis (some corpus callosum is present) or complete agenesis
Corpus callosum does not develop
Cingulate gyrus typically will not form either and therefore the more peripheral brain gyri will extend from ventricles to skull
Bundles of Probst
White matter bundles that normally would make up the corpus callosum but not just go linearly along the lateral ventricles
Classic findings
Racecar sign appearance of ventricles (does not look like racecar)
Longhorn cattle appearance of ventricles (actually kind of looks like this)
Aicardi Syndrome
Agenesis of corpus callosum + retinal abnormalities
Only in patients with 2 X chromosomes
Associated with pericallosal lipoma
Many other associations and things that can be seen concurrently
Sharpiro syndrome - hyperhidrosis + hyperthermia + agenesis of CC
Rhomboencephalosynapsis
Vermis does not form so you get a single lobed cerebellum
Focal cortical dysplasia
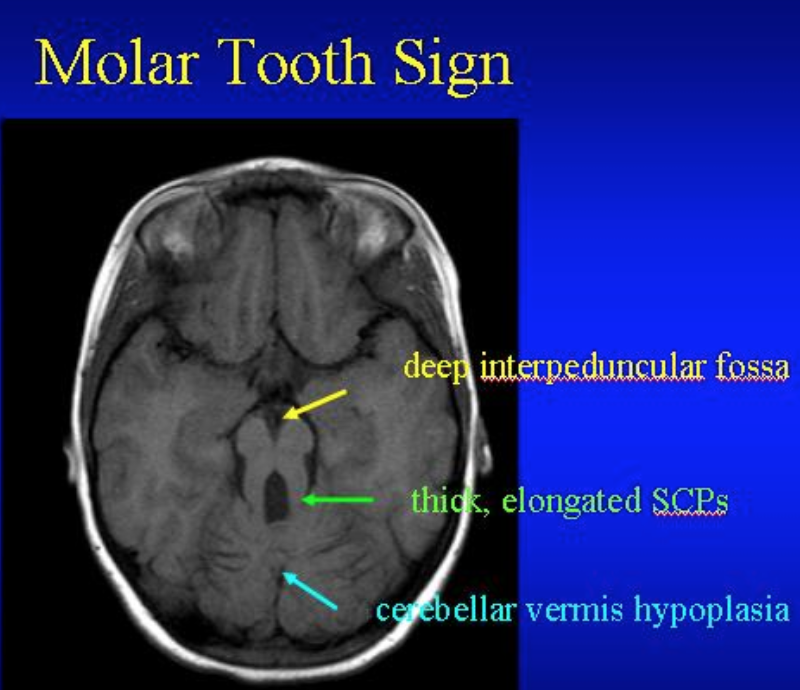
Joubert Syndrome
Small/aplastic cerebellar vermis
Absence of pyramidal decussation
Molar tooth sign
Strongly associated with
Retinal dysplasia
Multicystic dysplastic kidneys
General
Premature closure of skull sutures
Be sure the abnormal skull shape is not due to positional changes from always laying on the back to prevent SIDS
Normal suture closing times
Metopic: 3-9 months
Anterior fontanelle: 18-24 months
Sagittal: approximately 22 years
Coronal: approximately 24 years
Lambdoid: approximately 26 years
Squamosal: approximately 60 years
Scaphocephaly
Premature closure of sagittal suture
Elongation of skull in A-P diameter
Plagiocephaly
Asymmetric flattening of one side of the head
Positional
Laying on back too much to avoid SIDS
Nothing to do with suture closing just have the head which is a soft mush in the same position alot so it conforms to that shape
Ear on affected side will be more anterior
Parallelogram shaped head
Related to premature closure of
Lambdoid suture
Coronal suture
Harlequin eye sign
Looks like one orbital rim is pulled up and outward
Agyra
No gyri
Per-ventricular leukomalacia
More common in pre-mature babies
Believed to be result of hypoxic-ischemic injury in watershed areas, although could be related to vasculitis or infection
Look for history of prior bleed
Grading
US & MRI grading systems - Grading system radiopaedia
On US may look like many cystic areas alot of the time
Pachygyra
Broad gyri
Craniosynostosis
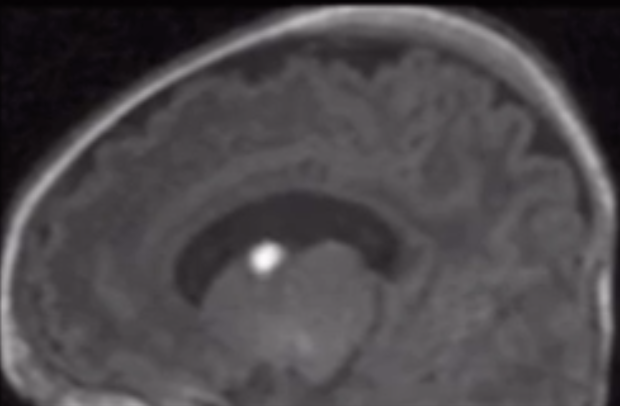
Ectopic posterior pituitary
Look for bright spot and see that it is not where it should be in posterior sella
Associated with pituitary dwarfism
References:
Case courtesy of Hidayatullah Hamidi, Radiopaedia.org, rID: 83386
Case courtesy of Naqibullah Foladi, Radiopaedia.org, rID: 83821