Musculoskeletal Metabolic Disease
Thalassemia
Extramedullary hematopoiesis
Prominent marrow expansion (appears as thick bones)
Generalized bone demineralization
Sarcoidosis
Lace-like/honeycomb appearance of the fingers
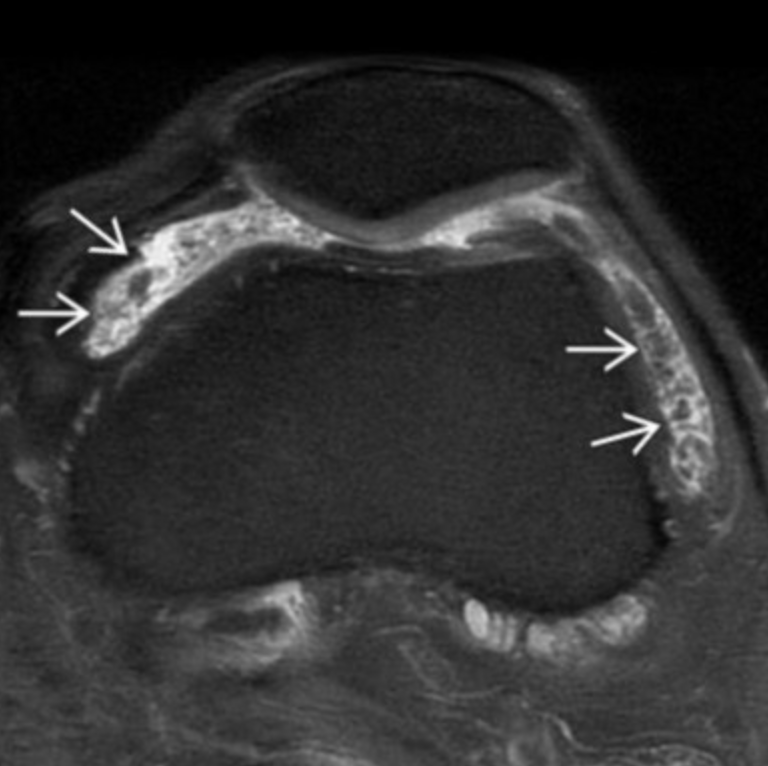
Synovial Osteochondromatosis
Primary (Reichel syndrome)
Monoarticular (70% in knee)
Seen in (relatively) younger patients (40-50s)
Intra-articular bodies
Many
Uniform in size
No joint degeneration
Synovial hyperplasia commonly present
Classically demonstrates blooming artifact on MR

Secondary
Intra-articular loose bodies secondary to pathology (OA, infection, others)
Seen in older patients
Intra-articular bodies
Many (but less than primary)
Multiple sizes and shapes
Associated with joint degeneration
Tx = remove the bodies and possible synovial membrane removal
Basically a bunch of intra-articular ossified loose bodies
Bizarre Parosteal Osteochondromatous Proliferation (Nora lesion)
Basically localized hypertrophy of the cortex, usually in hands and feet
Does not typically affect medulla
Benign, no treatment
Very similar to osteochondromas
Note: OC will connect with medulla and are typically oriented away from the nearby physis, both of which are not seen in Nora lesions
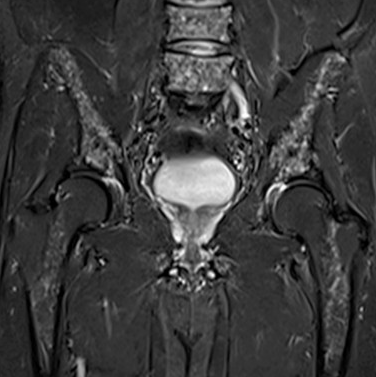
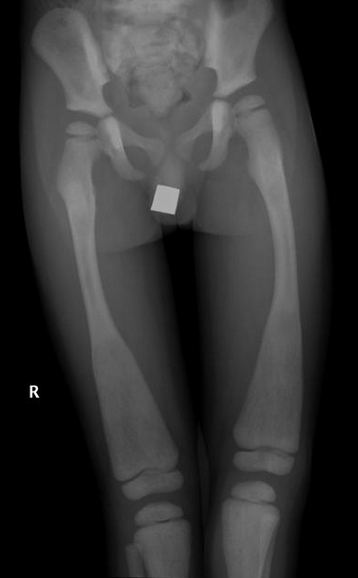
Mazabraud Syndrome
Fibrous dysplasia + intramuscular myxomas
Intramuscular myxomas are hypo T1, Hyper T2 and variable enhancement
Most commonly of the pelvis and lower extremity
More common on right side
GNAS1 gene mutation —> 20q13.2-q13.3
Associated with McCune Albright syndrome
Maffucci Syndrome
Multiple enchondromas
Soft tissue venous malformations - will be seen as phleboliths on plain films
Spindle cell hemangiomas
Infants, s&s usually by 1 year old
Hands & feet affected typically
Post Radiation Changes
Radiation induced osteitis
T2 hyperintense
Heterogenous enhancement
Increased uptake on bone scan and PET
Radiation induced osteonecrosis
Mixed lytic and sclerotic appearance without cortical break through
Decreased uptake on bone scan and PET
Radiation induced growth deformity
Basically getting radiation before skeletally mature and results in defect
If you radiate the spine can get defect resulting in scoliosis
Typically whatever is radiated will become short
Radiation induced sarcoma
Lipoma Arborescens
Frond like fat, will be fat signal on all sequences
Honesty looks like mild PVNS

Multiple Hereditary Exostoses
Basically looks like a wavy and thickening cortex
Does not have to be the pedunculated ones you typically think of
Hypophosphatasia
Osteopenia + fractures + bowing + metaphyseal widening (key)
POEMS Syndrome
Polyneuropathy
Organomegaly
Endocrinopathy
Monoclonal gammopathy
Skin changes
To diagnose must have 2 mandatory criteria, one major and one minor
Mandatory
Polyneuropathy
Monoclonal plasma cell proliferation
Major
Sclerotic bone lesion
Elevated VEGF
Castleman disease
Minor - basically anything that fits in the category of POEMS abbreviation
Bone lesions are typically SCLEROTIC multiple and small (<1 cm) (some say can be lytic with sclerotic border)
Fibrodysplasia Ossificans Progressive
Calcium Pyrophosphate Disease (Pseudogout)
Arthritis + concurrent CPP deposition in cartilage
The deposit should enhance
Presents clinically the same as gout
Amyloid Spondyloarthropathy
Aka multilevel spondylosis from hemodialysis
Essentially is just degenerative shit in the spine but because they are on dialysis they need a new name for it
Sickle Cell
Bone infarcts
Multiple Myeloma
Lytic lesion taking up entire medullary canal with expansion and thinning of cortex
Can have cortical breakthrough and soft tissue mass
Diffuse osteopenia, advanced for patient age
Salt and pepper appearance of some bones
Should include risk of impending pathologic fracture
MR Findings
Diffuse marrow infiltration
Enhancement seen in both active and treated lesions
T2 bright in both active and treated lesions
Plasmacytoma is the related mass
Honestly just looks like mets + salt and pepper + advances osteopenia

Jaffe-Campanacci Syndrome
Multiple NOFs
Cafe au lait spots
Mental retardation
Eye, genital, heart malfomations
I think of this as NOF + neurofibromatosis basically
Ollier Syndrome (enchondromatosis)
Multiple enchondromas, typically metaphyseal
Increased risk of chondrosarcoma later in life
Bilateral but asymmetric
Hands and feet most commonly

Pigmented Villonodular Synovitis (PVNS)
Monoarticular (70% in knee, 10% hip)
Synovial proliferation
Large subchondral cysts
Osteomyelitis
Acute osteomyelitis
Looks like what you think of with osteo, aggressive, cortical destruction, edema
Chronic osteomyelitis
Doesn’t really look like osteo
Cortical thickening
Abscesses
Enhancement of the marrow
Osteogenesis Imperfecta
Osseous demineralization + gracile bones + fractures
Hypervitaminosis D
Looser’s zones are seen
Enthesopathy
Osseous fragility, fractures
Hyperparathyroidism
Decreased bone density
Brown tumors
Usually seen a multiple lytic lesions with additional lesions that look like they are healing concurrently
Subperiosteal resorption along radial aspect of phalanges
Subperiosteal reaction is basically resorption of bone under the periosteum and really looks like subtle inward curve (concave) appearance on the affected side, not very obviously unless very asymmetric on each side
Acro-osteolysis
Salt & pepper skull
Superior and inferior rib notching may be seen - only this & rarely NF-1 that do both superior and inferior notching
Bunch of other nonspecific shit that is basically all centered around bone being resorbed

Retinoid Associated Hypertrophic Bone
Basically taking retinoids causes increased bone deposition i guess so you get enthesopathy and bone deposition
Predominantly in axial skeleton
Hydroxyappetite Deposition Disease
Shoulder is most common site of deposition, typically supraspinatus
The deposit does not enhance
Milwaukee shoulder
Destructive arthritis essentially secondary to HADD
Gout
Sodium urate deposition
Deposit is round rather than linear (HADD)
Deposit enhances
Random Named Conditions
Gaucher Disease
Most common lysosomal storage disease
Autosomal recessive
Accumulation of lipids in bone marrow, spleen and liver
Erlenmeyer flask deformity (metaphyseal flaring)
Undertubulation
Bone infarcts with collapse
Hepatosplenomegaly
References:
Lipoma Arborescens
Frond like fat, will be fat signal on all sequences
Honesty looks like mild PVNS