Musculoskeletal Masses
General
Man characteristics to determine what makes a mass look benign or malignant, only one that really matters is zone of transition
Zone of transition
Basically how does the border between the mass and the surrounding normal bone look
Narrow = well defined borders - sclerotic rim - benign
Wide = ill defined borders - fades into surrounding bone - aggressive (but not always malignant, i.e. infection, eosinophilic granuloma, etc.)
Only applies to lytic lesions
Can only be used on plain films
Non-Ossifying Fibroma
Metaphysis
Commonly lucent lesion with thin sclerotic margins
Typically not seen after age 30 (fully ossify and don’t see them)
Don’t touch lesion
Quick way to differentiate from FD is to see if lesion is only near cortex/periphery, if yes then likely NOF, if involves middle may be FD as those are intramedullary


Bone Infarct
Can really look like anything, classically has serpentine sclerotic borders
May look similar to enchondroma but note that enchondroma should not have sclerotic borders on radiograph
Epiphyseal Equivalents
Basically areas of the body that don’t have typical epiphysis like long bones do but where the epiphyseal differential applies
Calcaneous
Patella
Trochanters
Carpal & Tarsal bones
Epiphyseal Lesion >40 yo
Giant cell tumor
Infection
Mets
Myeloma
Geode
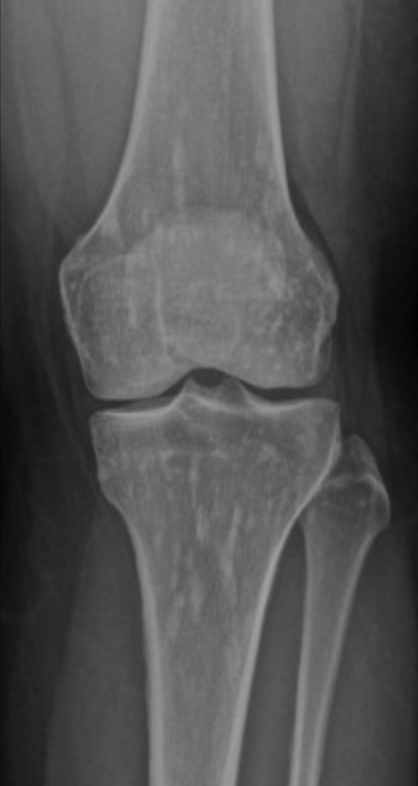
Giant Cell Tumor
Age 30-60
Criteria
Physis must be closed
Non-sclerotic border
Abuts articular surface
60% at knee
Eccentrically located (not central)
Typically metaphysis
Lytic lesion on radiograph
Quasi-malignant - have pulmonary mets
Look for epiphyseal mass + lung mass in patient <40!, if >40 then mets
Giant cell tumor of tendon sheath a little different
Ewing Sarcoma
Permeative lesion with onion skin periostitis - bone may look essentially normal!!!!
Age <10
Rare in african americans
Diaphysis & flat bones (scapula)
Large soft tissue component
Mets to lungs
Near indistinguishable from osteomyelitis but if the following are present they would favor osteo:
Sinus tracts
Air in soft tissues

Synovial Sarcoma
Misnomer as does not actually arise from synovium or in the joint but typically adjacent to joint
Strong predilection for the extremities
Relatively young 15-40 yo
Slow growing and does not have to be painful
Calcifications about 1/3 of the time
Not required but commonly located next to a neurovascular bundle (popliteal space, anterior shoulder for example)
Triple sign
3 different densities
Looks like teratoma in the soft tissue, sometimes, other times just looks like a fucked up mass
Split fat sign
Very thin line of fat along periphery of mass, very subtle
Heterogenous on MR with internal necrosis
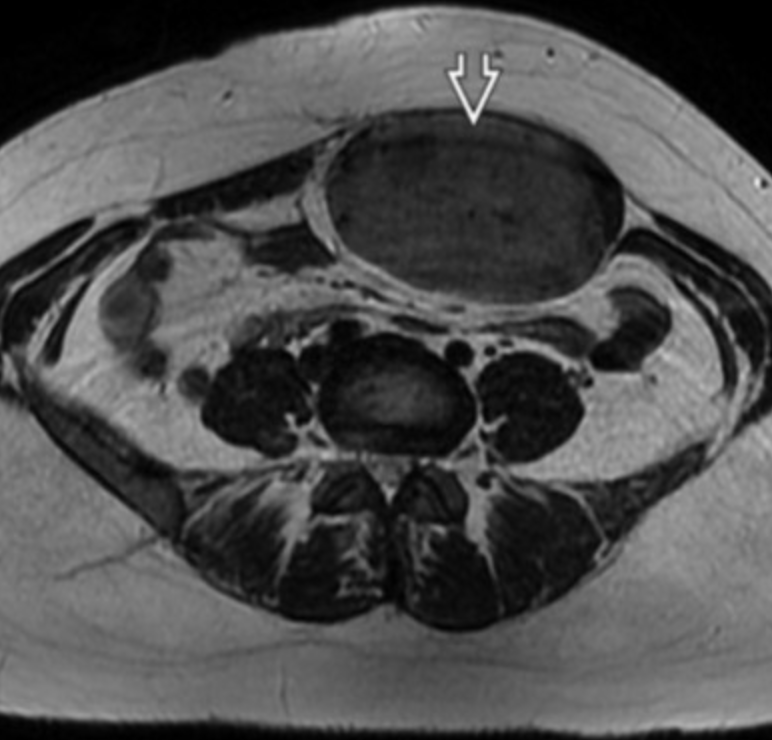
Liposarcoma
Fat containing mass
Retroperitoneal mass containing fat
Larger and deeper favors liposarcoma over lipoma
Myxoliposarcoma
T2 bright
Respond well to radiation
Mutlilobulated
Sarcomatous transformation
Look for interval growth
Enhancing septa
Dermatofibrosarcoma Protuberans
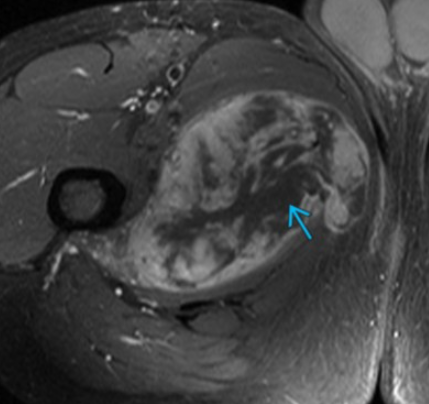
Rhabdomyosarcoma
Pelvic RMS
Peak incidence in childhood at age ~2-6 years
Can occur from anywhere including bladder, uterus, vagina, etc


Enchondroma
Arcs and rings - chondroid matrix
Really just looks like thick sclerotic mass with little lucent areas in it
Endosteal scalloping
No periostitis
Will appear as just a cystic lesion in the phalanges not as the typical chondroid matrix described above
Most common cystic lesions in phalanges
Non-painful
Findings concerning for chondrosarcoma
Painful
If internal matrix changes appearance
Ollier’s Syndrome
Multiple hand enchondromas
No increased risk of cancer
Maffucci Syndrome
Multiple hand enchondromas
Multiple hemangiomas (look like phleboliths)
Increased risk of cancer

Osteoma
Basically a calcified ball
Commonly seen in sinuses
Associated with Gardner syndrome
Pagets Disease
Expansion of bone with thickened trabecula
Multiple lesions
Pelvis most commonly affected
Almost never in fibula
Blade of grass —> pointed appearance of lesion within the bone
Secondary osteosarcoma can occur —> very bad
Classic Osteosarcoma
Age 10-20 yo
Osteoid matrix (cloud like)
Metaphysis typically
Femur and humerus typically
Mets to lungs
Spontaneous pneumothorax
Skip lesions
Mets within the bone
Resection with chemo for micromets
Second worst prognosis of the osteosarcomas (secondary OS in pagets is worst)
On plain film may look like osteomyelitis but need mri, don’t really know how to tell the difference tbh

Fibrous Dysplasia
Intramedullary expansile lesion with well defined borders
Multilobulated
Long lesion in long bone with ground glass matrix
Endosteal scalloping (irregular resorption of inner layer of cortex adjacent to medullary cavity)
Lucent or sclerotic or mixed
Ribs (monostotic) and femur (polyostotic) are common sites
If in pelvis then also in ipsilateral femur (not vice versa)
Shephard crook deformity of femur
McCune-Albright
Fibrous dysplasia in multiple bones
Cafe au lait spots
Precocious puberty
Mazabraud syndrome
Fibrous dysplasia in multiple bones
Soft tissues myxomas


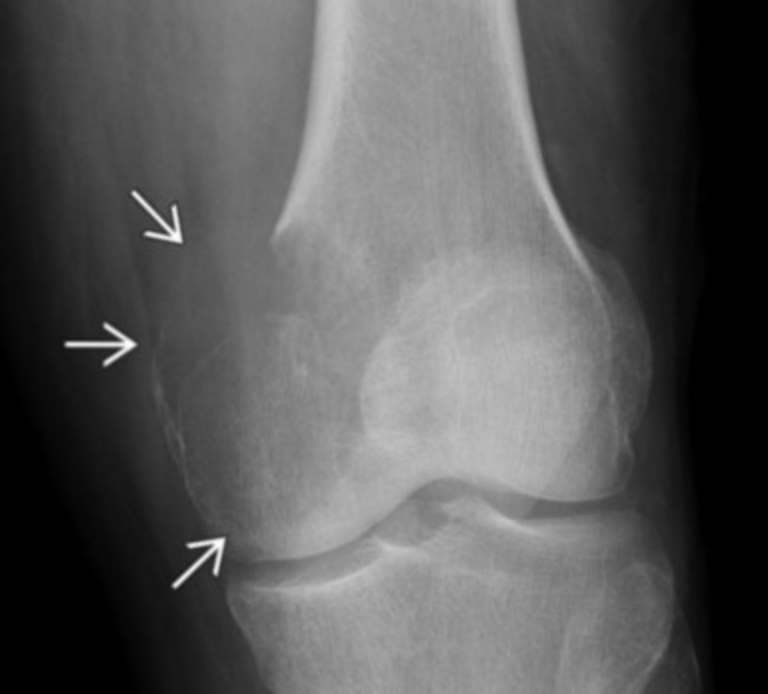
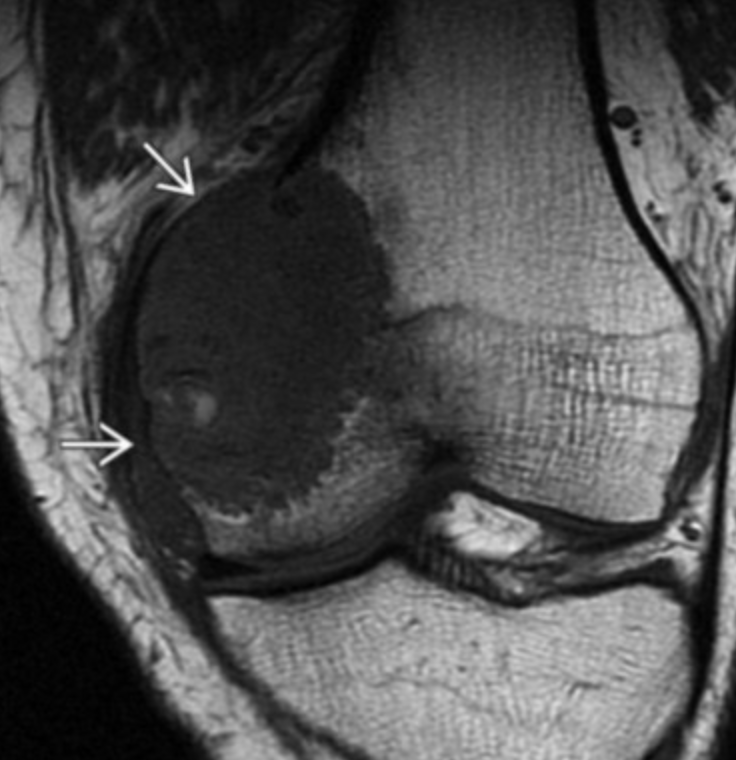
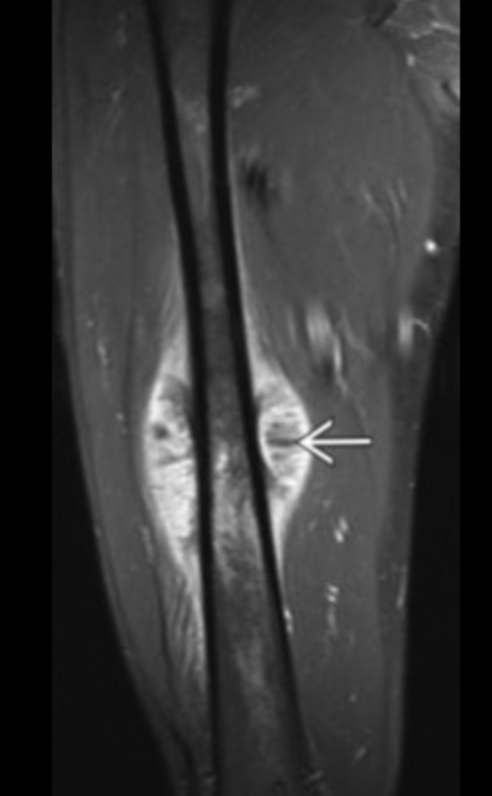
Fibroxanthoma
Well-defined, eccentric, bubbly lucent lesion in the metaphysis of a child with deep sclerotic margin, overlying cortical interruption, and no periosteal reaction are essentially diagnostic of a fibroxanthoma (or nonossifying fibroma). The mixed signal of the lesion on MR is also typical of a fibroxanthoma.
Epiphyseal Lesions
Epiphyseal Lesion <40 yo
Giant cell tumor (epiphysis must be closed)
Infection
Chondroblastoma
ABC
EG
Chondroblastoma
Epiphysis
Humerus > tibia > femur
Age 10-25
Lytic
Calcify

Fluid-Fluid Level Masses
ABC
Telangiectatic Osteosarcoma
Giant cell tumor
Osteochondroma
Same thing as exostosis
Contiguous with intramedullary cavity
Osseous looking things that grow away from the joint space
Multiple hereditary exostosis
Multiple lesions
Hyaline cartilagenous cap >2 cm = malignant transformation to chondrosarc
Must be skeletally mature for this to apply as cartilage cap is expected to be bigger in kids
Also, if you have more lesions, each has a small risk of becoming cancer, so having more means increased risk of cancer
Can arise after radiation treatment
Trevor disease
Osteochondromas that point toward the joint
Chondrosarcoma
Adults
Flat bones
Ribs
Chondroid matrix
Really just looks stippled
Popcorn appearance
Can be completely lytic on radiograph, does not have to have chondroid matrix
Common in sacrum
Surface Bone Sarcomas
Peri & Para, not the other osteosarcs
PAR-osteal Osteosarcoma
Age 20-50 yo
Looks like densely calcified mess of shit
Metaphysis
Posterior distal femur
String sign
Lucent line separates calcific mass from the cortex of bone
Lower grade
Best prognosis of the osteosarcomas
Reverse Zonal Ossification
Central area of calcification that over time will have increased and progressively calcification grow around it
Opposite of zonal ossification seen in myositis ossificans which has a peripheral ring of calcification which then fills in with calcifications moving inward
Plasmacytoma (MM)
Can basically look like anything
Plasmacytoma = mini-brain
Diffuse osteoporosis
Large solitary expansile lesion
POEMS syndrome - will be sclerotic instead of normally lytic
Bakers Cyst
Seen between medial head of gastrocnemius and semimembranosis
Elastofibroma
Soft tissue, fat containing mass
Mildly enhance
Classically between scapular and chest wall
Osteopathic Striatica
Linear lines in bone
Means nothing
Fibrotic Conditions
Sacrococcygeal teratoma
Usually identified by 5th week of gestation
Not really seen after neonate period (not expected in kids >1 year or even a few months tbh)
Typical teratoma look with cystic and mixed density
shit
Unicameral/Solitary Bone Cyst
Usually <30 yo
Commonly in arm & calcaneous
Lytic lesion, commonly with fracture
Fallen fragment sign
Osteoid Osteoma
Basically looks like a target
Central sclerotic area with peripheral lucency
Hot on bone scan

PERI-osteal Osteosarcoma
Age 15-25 yo
Looks more ill defined and lucent
Diaphysis
Medial distal femur
Wraps circumferentially around bone
Intermediate prognosis
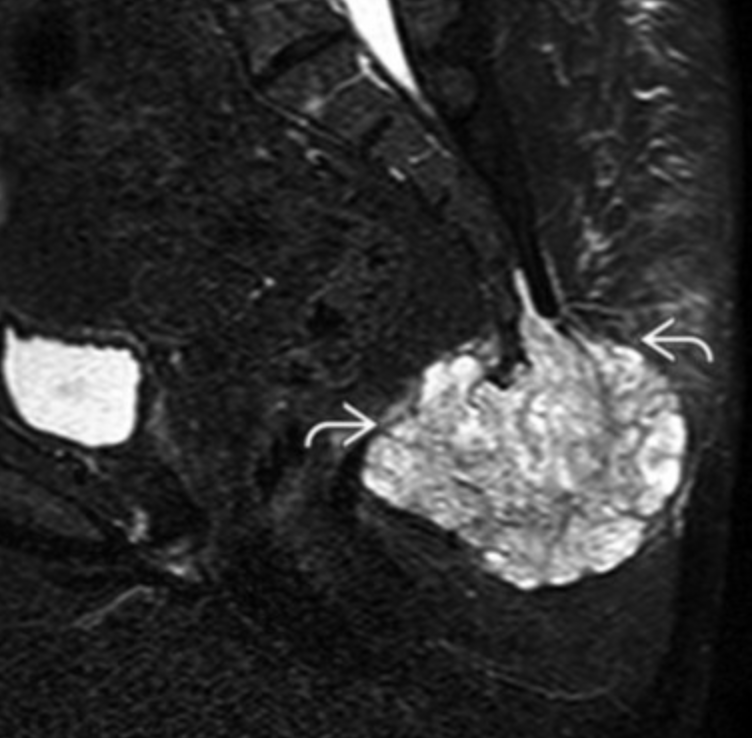
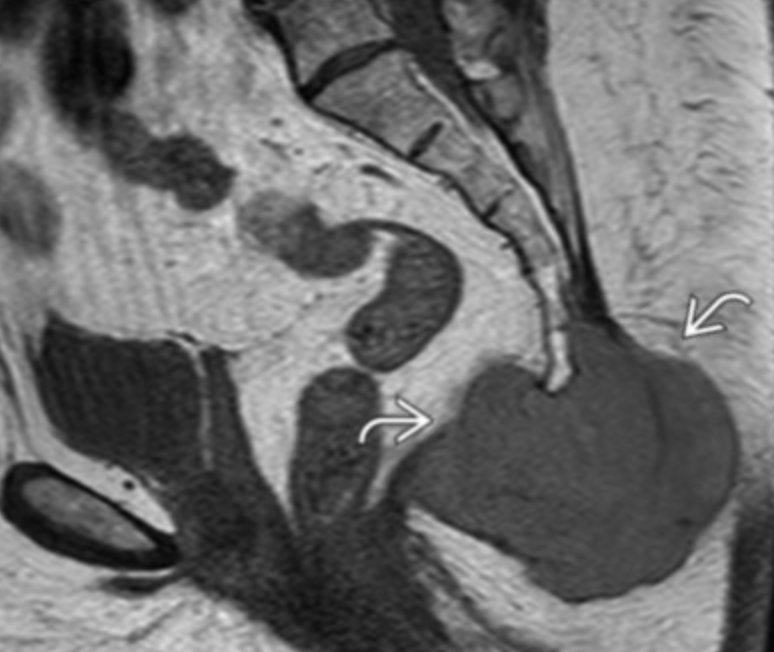
Chordoma
Embryologic remnant of notochord
Only occurs at midline
Sacrococcygeal (50%)
Clivus (30%)
C2 vertebral body
T2 bright & heterogenous
Age 40-70
Locally aggressive
Mets possible in late stage
Malignant Fibrous Histiosarcoma
Aka Pleomorphic Undifferentiated Sarcoma
Central thigh or upper arm
Age 60s
RF
Pagets
Radiation
Osteopoikilosis
Clustered bone islands
Centered around joint
Looks like mets
If you see just a cluster of shit that looks like mottled bone the way metsatasis does but it is only in one area and spares the areas away from the joint (diaphysis for example)
Spares axial skeleton
Not in spine !
Schwannoma
Target sign
T1 hypo
T2 hyper or heterogenous
Strong enhancement
Desmoid type tumor
Low signal on T2
Homogenous enhancement
Commonly in rectus muscles
Classically enlarge in pregnant women
Otherwise slow growing
Spine Masses of Bone
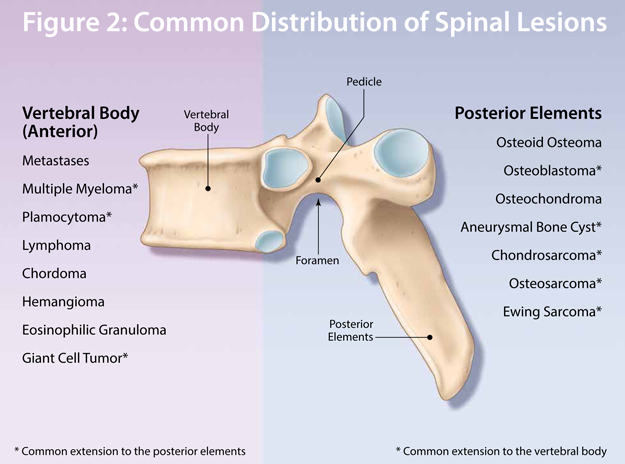
Osteoblastoma
Posterior elements
Superficial Fibromatosis
Benign but locally aggressive
Osteoid Osteoma
Posterior elements
Densely sclerotic
Conditions

References:
Case courtesy of Yi-Jin Kuok, Radiopaedia.org, rID: 17974