Knee MRI
Ligaments
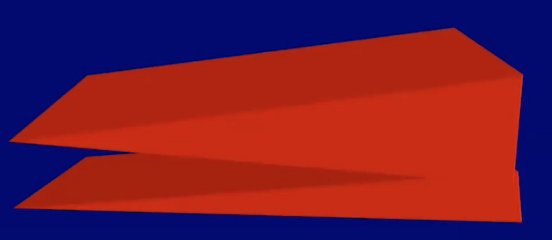
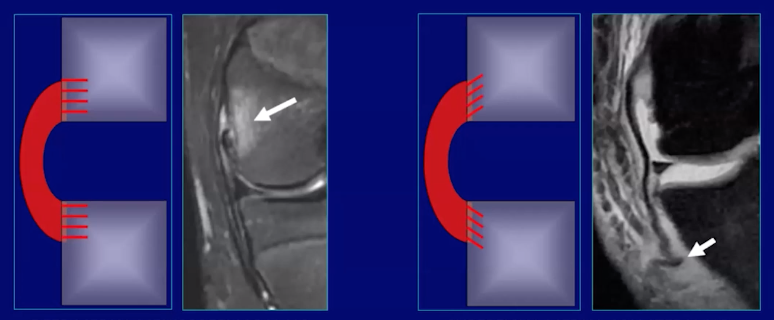
Direct insertion (left)
Ligament attaches to cortex of bone at right angles
Will result in marrow edema with injury
i.e. MCL femoral attachment, ACL tibial attachment
Indirect insertion (right)
Ligament attaches to cortex at oblique angles
Tend not to have marrow edema with injury
i.e. tibial insertion of MCL
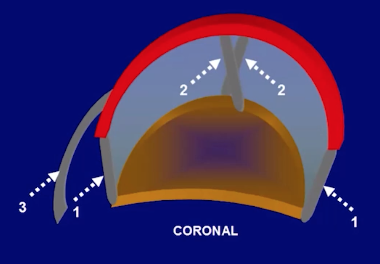
Primary capsular ligament (1)
Accessory intra-capsular ligaments (2)
Accessory extra-capsular ligaments (3)
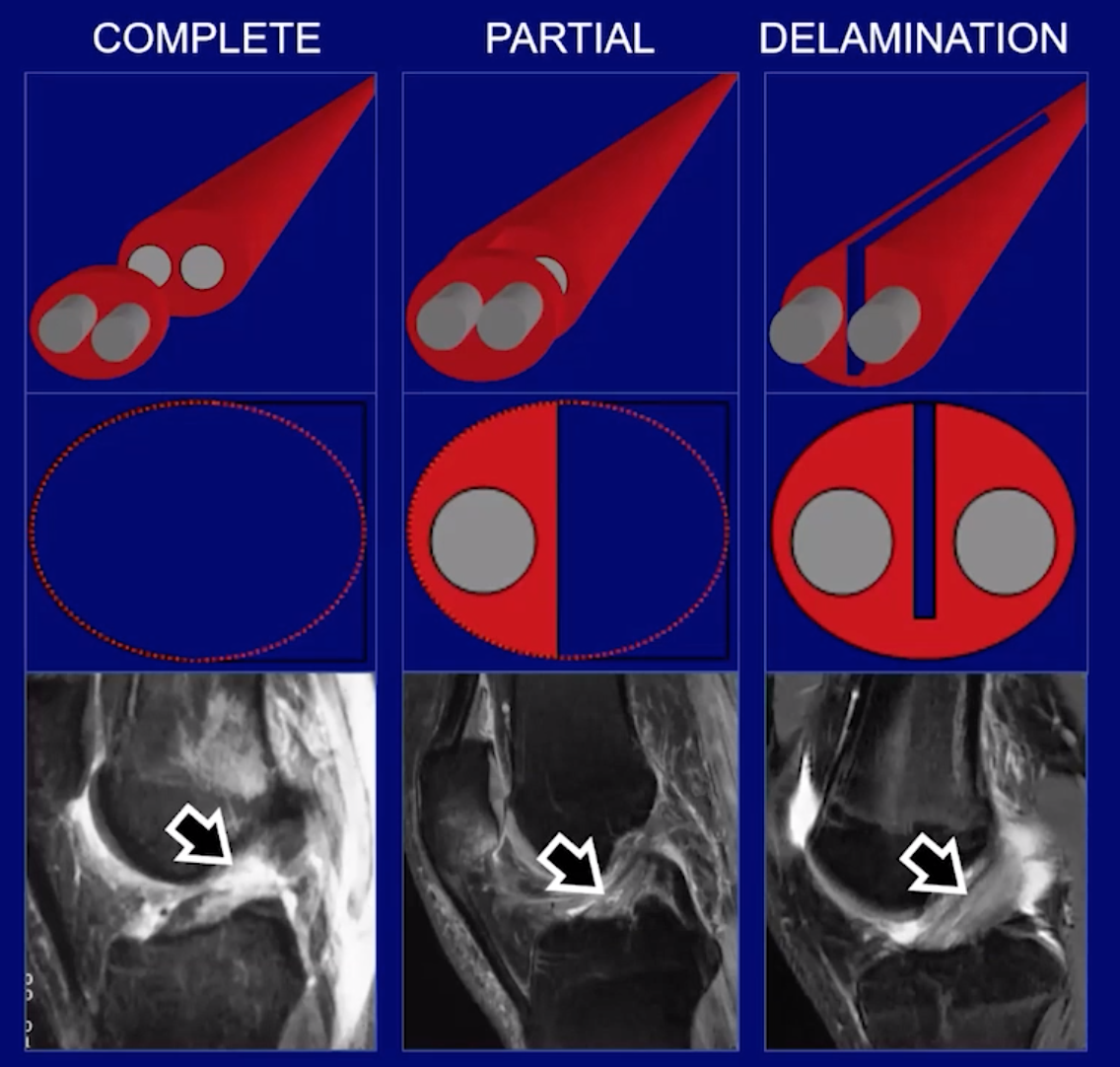
Ligament Injury
Complete
Partial
Delamination
PCL
Anteriomedial bundle
Posteriorlateral bundle
Injury mechanism
Posterior force to the tibia (dashboard injury)
Hyperflexed knee
Posteriorly directed force on a hyperextended knee
When you get injury via one of the mechanisms listed above you will commonly have injury to the posterior-lateral corner of the knee so look for
Reverse segond fracture
Avulsion fracture of medial meniscotibial ligament
PCL injury
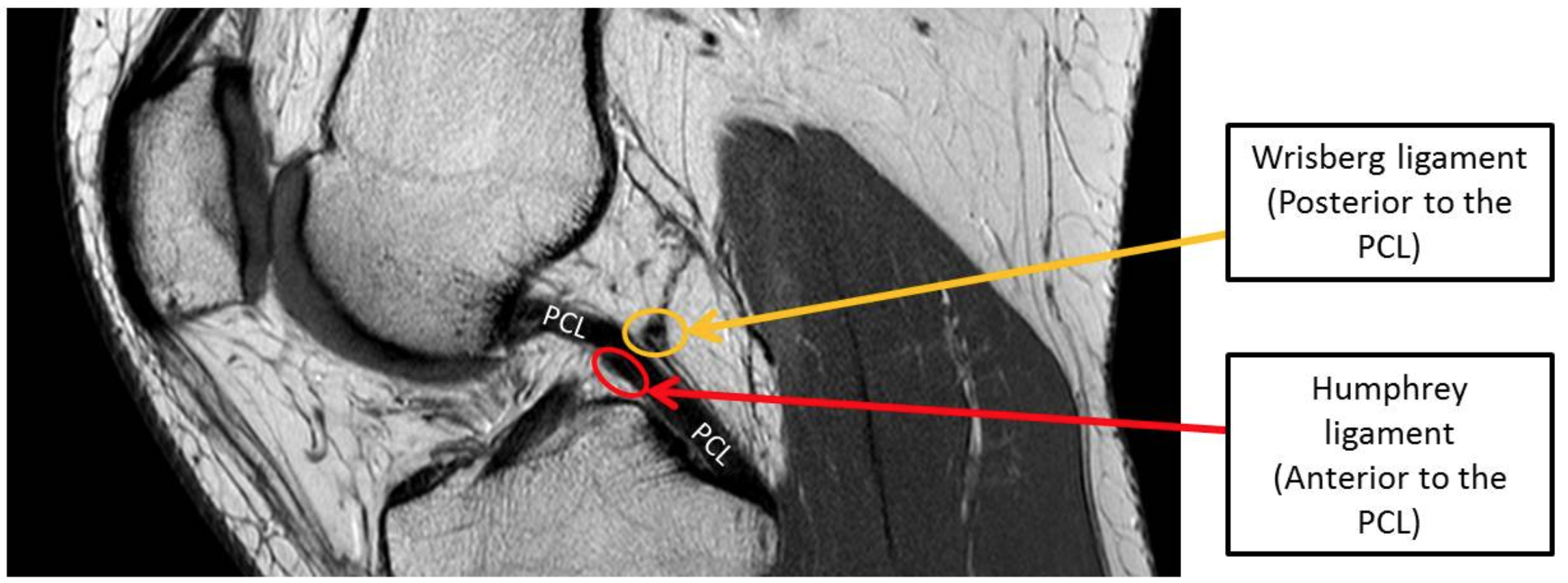
Posterior meniscofemoral ligament = Wrisburg = posterior to PCL
Can have bifurcation that looks like a tear but is not
Can have it terminate at mid portion of PCL and makes PCL look like it has a hump
Anterior meniscofemoral ligament = Humphrey = anterior to PCL
Posterior Lateral corner
Popliteal-femoral ligament
Arcuate ligament
Posterior to popliteal femoral ligament
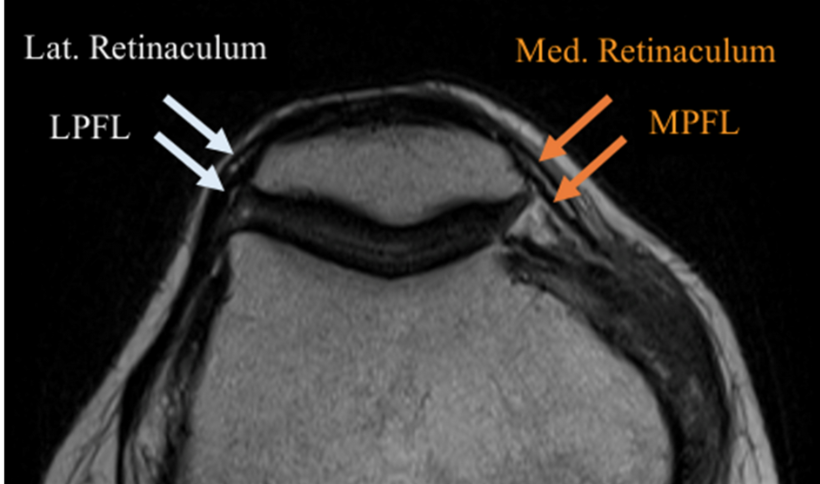
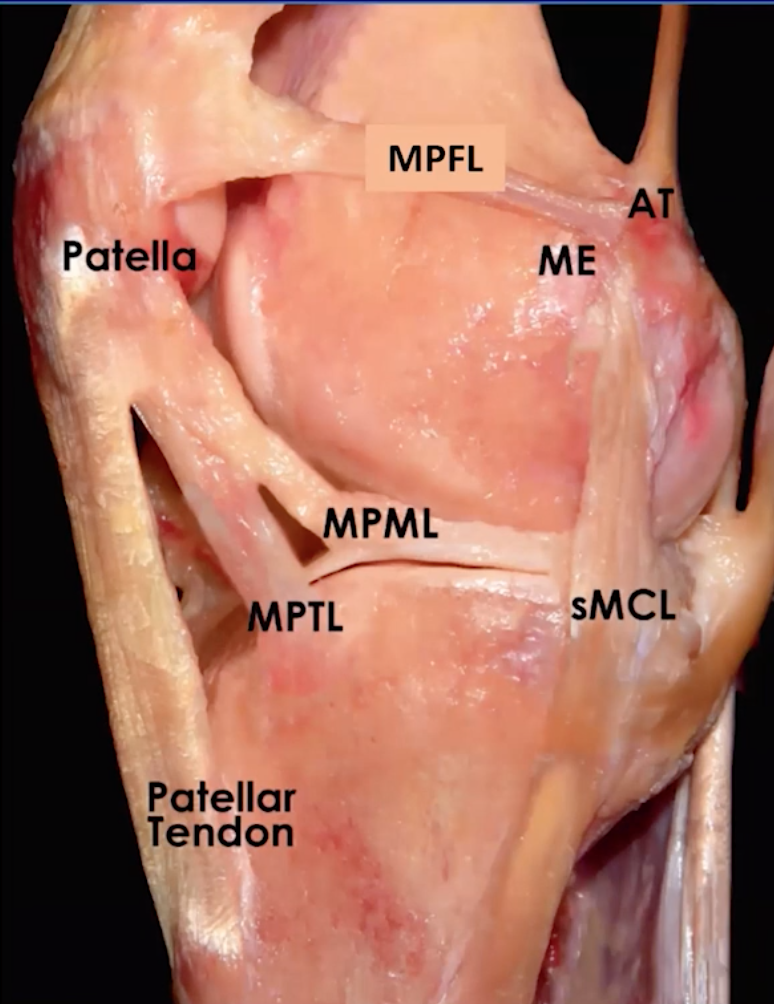
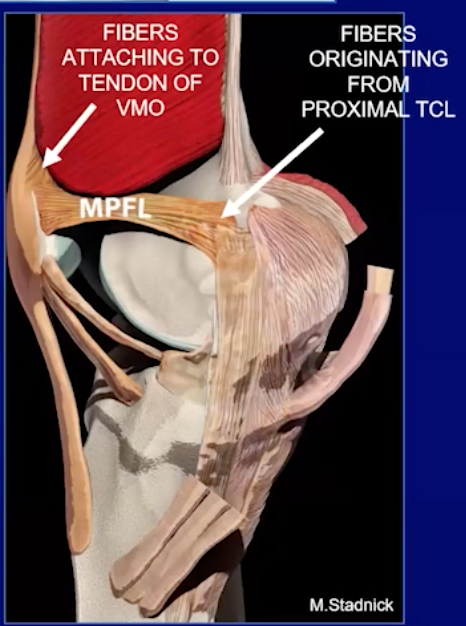
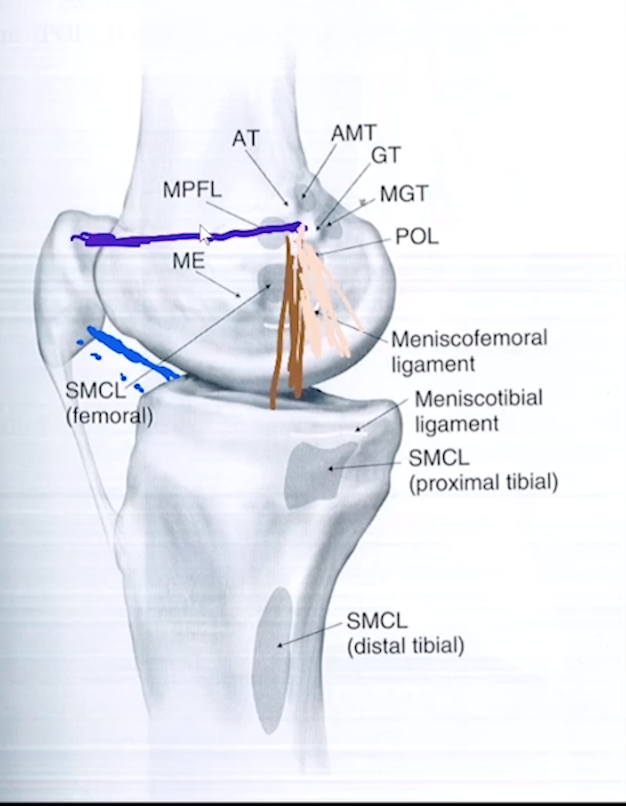
Medial Patellofemoral ligament (MPFL)
Thicker deeper dark line
The more superficial, thin and whispier line is the medial retinaculum
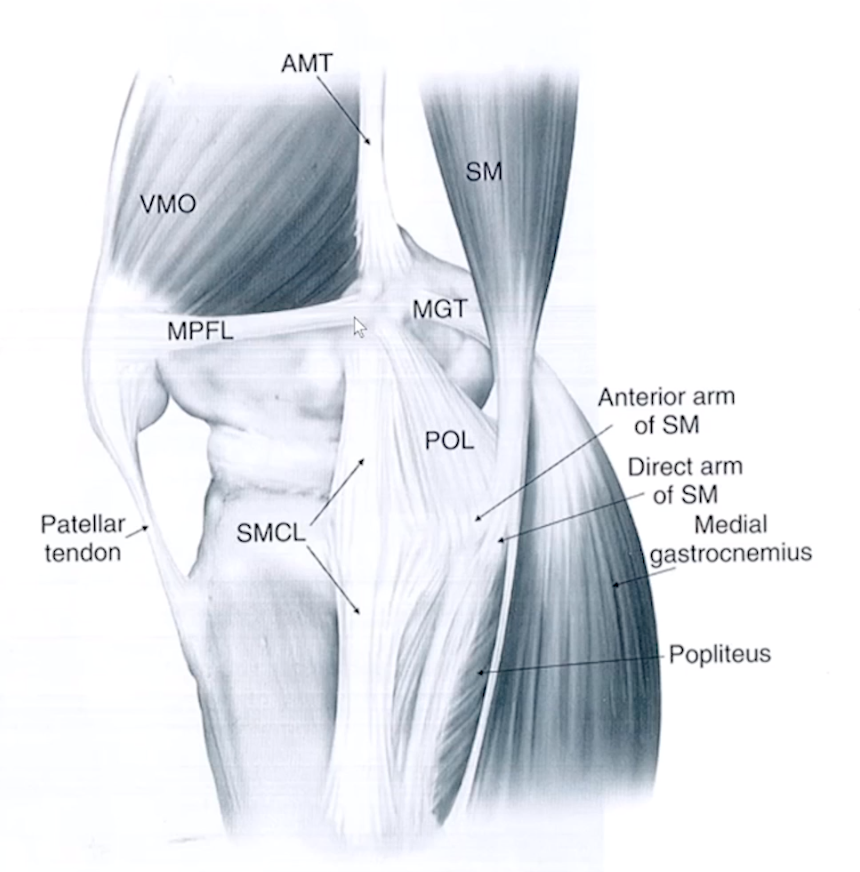
Posteriormedial corner of knee
5 parts
Posterior oblique ligament = major player
Oblique popliteal ligament
Meniscotibial ligament
Semimembranosus tendon
Medial meniscus
Posterior Oblique Ligament
3 Parts
Superficial
Most anterior
Tibial/Central
Largest and thickest portion
May attach to meniscus
Capsular
Most posterior
Medial Collateral Ligament (MCL)
3 Layers
Superficial layer -
fuses with medial retinaculum of patella
Middle layer -
aka tibial-collateral ligament
fuses with MPFL
Deep layer (2 parts)
Menisco-capsular attachment to femur
Curves up from meniscus to attach on distal and lateral edge of femur
Menisco-tibial ligament
Curves down from meniscus to proximal and lateral edge of tibia
Special Considerations in Kids
FOPE
ACL
Anteriomedial bundle
Posteriorlateral bundle
Mucinous Degeneration
In a delamination injury the space can become filled with mucinous shit and thats how we get the mucinous degeneration of the ACL
Mucinous degeneration tends to affect the posterior-lateral bundle
Aka celery stalk appearance
Can have cystic changes at bone attachment site or paracruciate ganglion cysts
ACL Injury
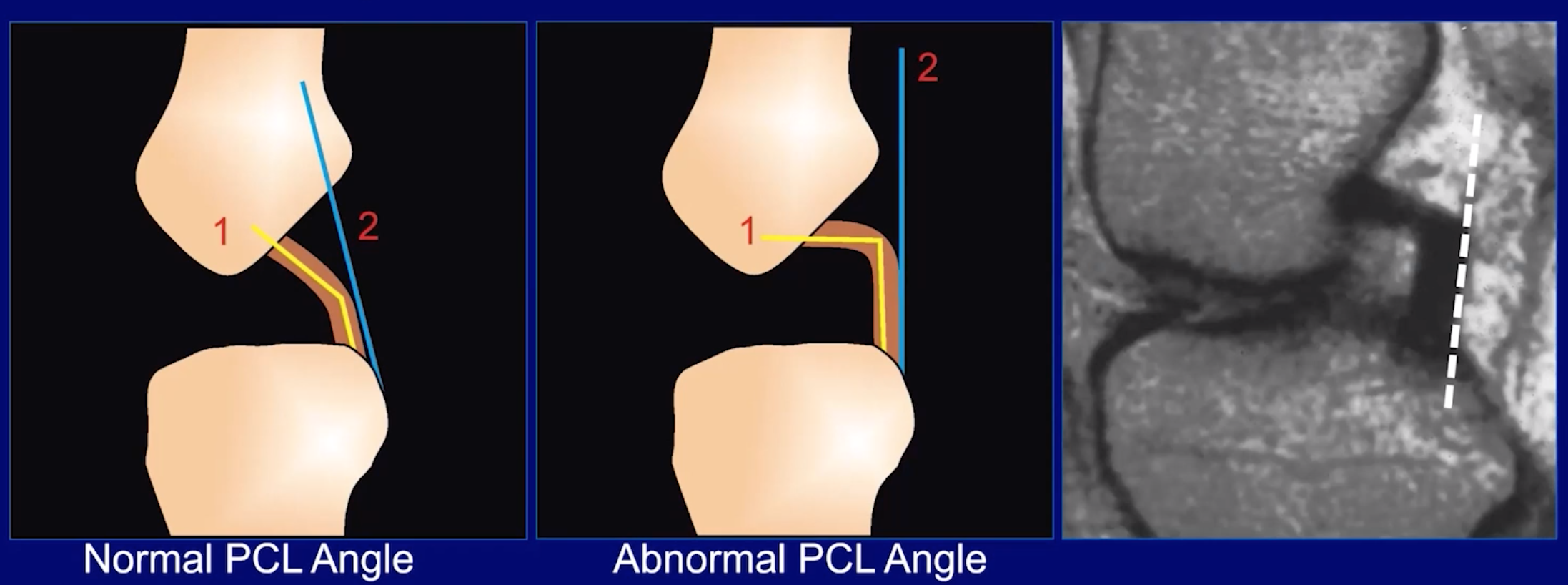
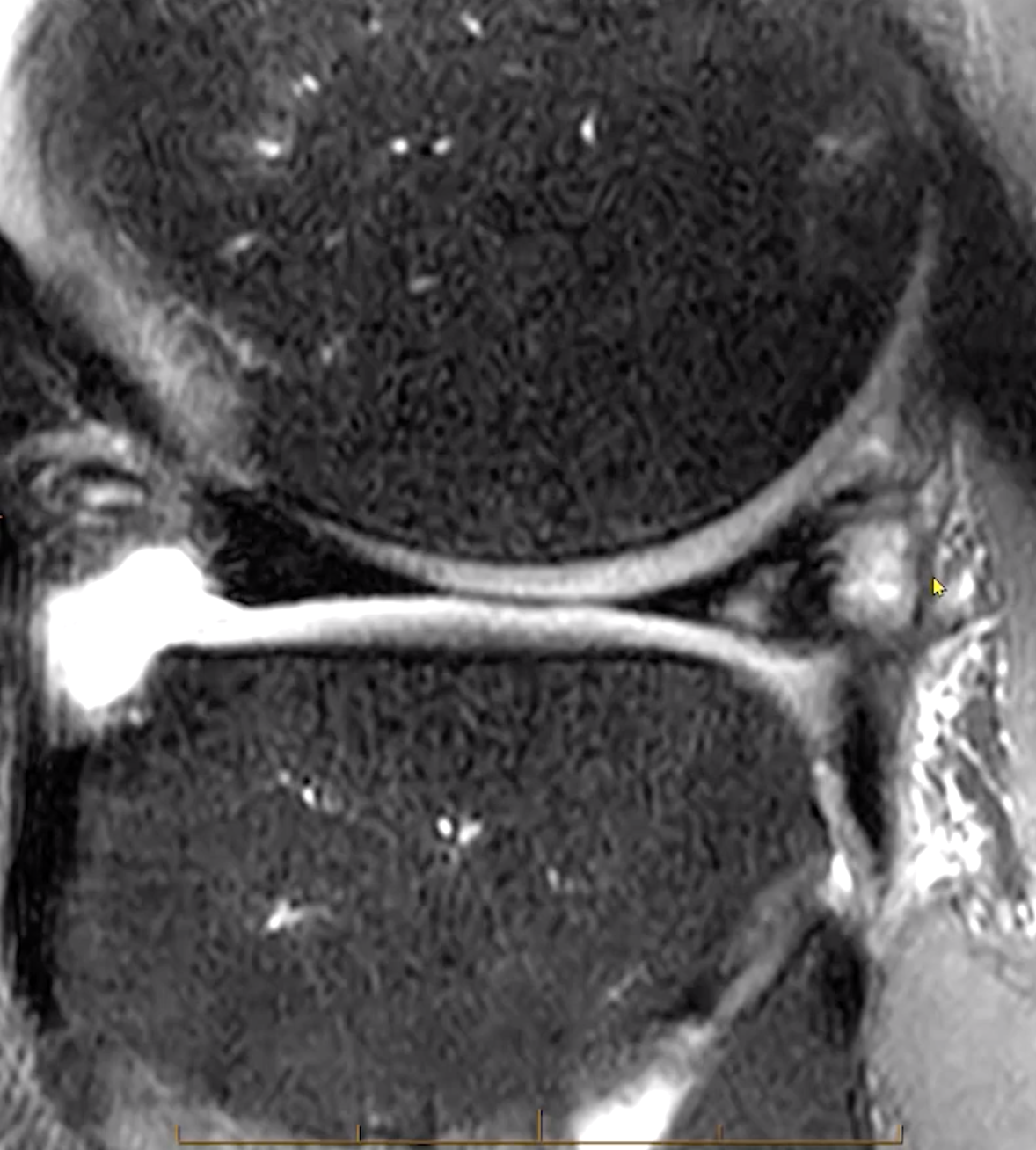
Abnormal PCL sign
ACL tear causes PCL to become lax and lose normal configuration and now does not have the normal slope it should have which is a sign of ACL injury
Anterior tibia translation
Look for uncovering of lateral meniscus
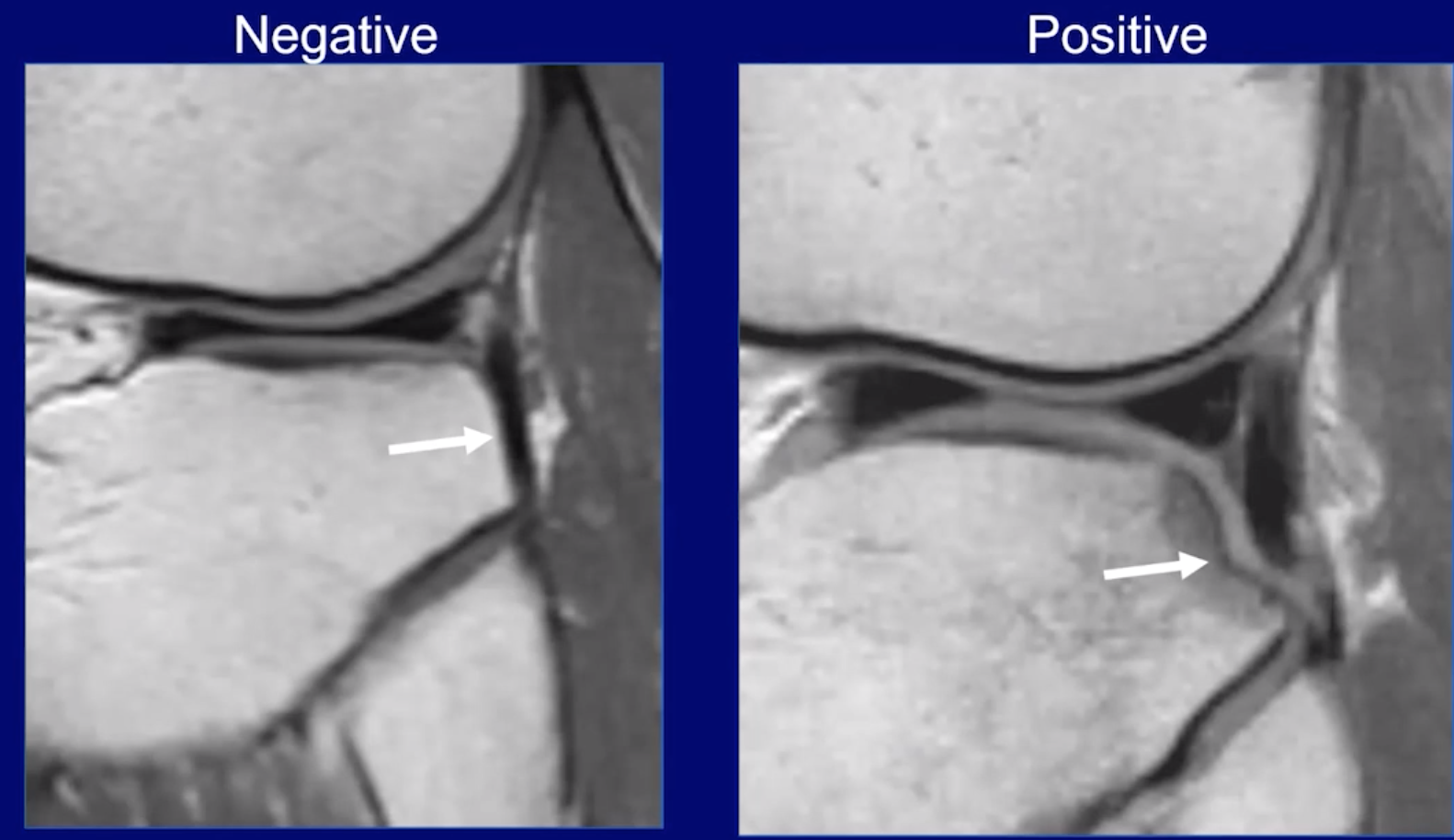
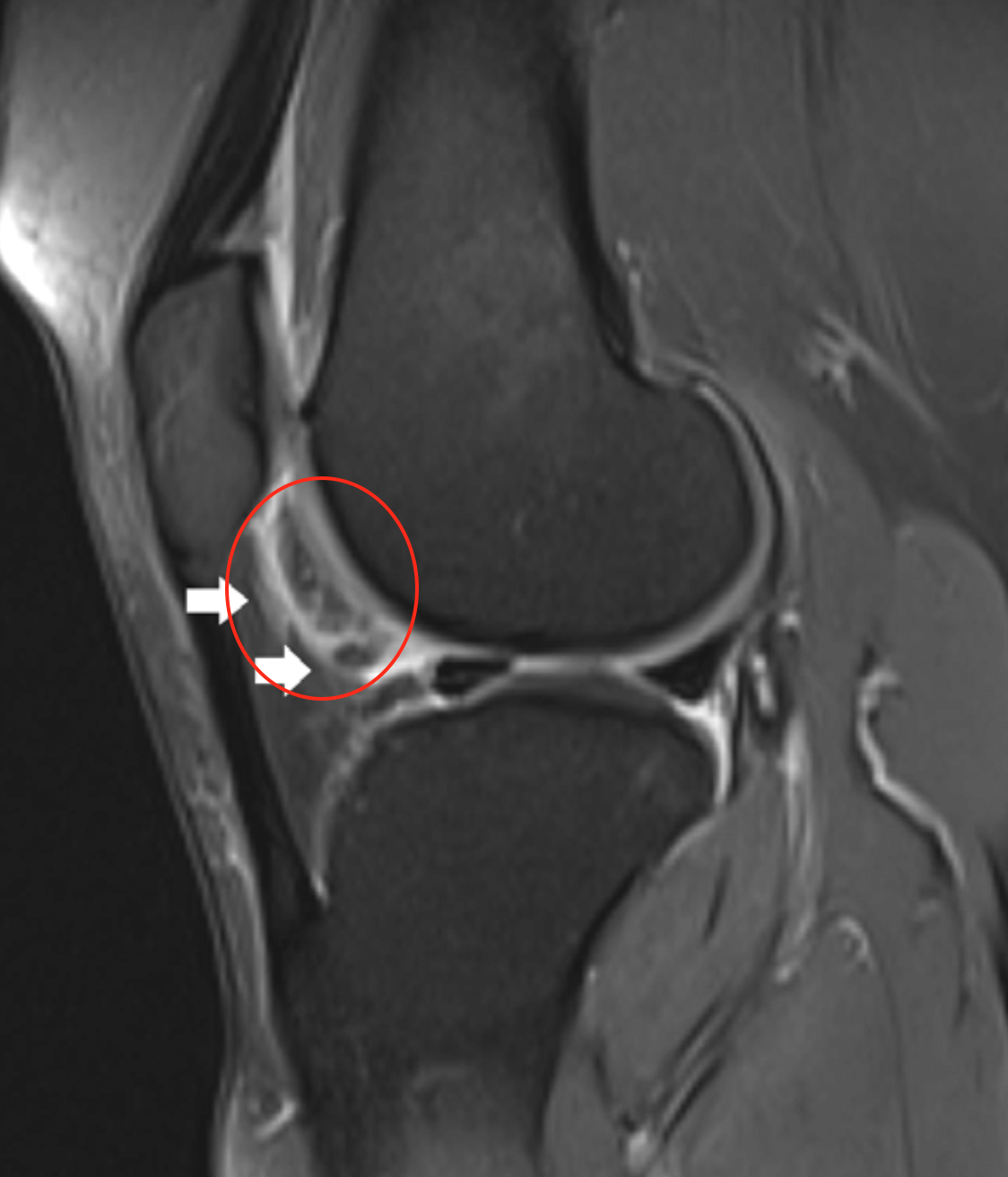
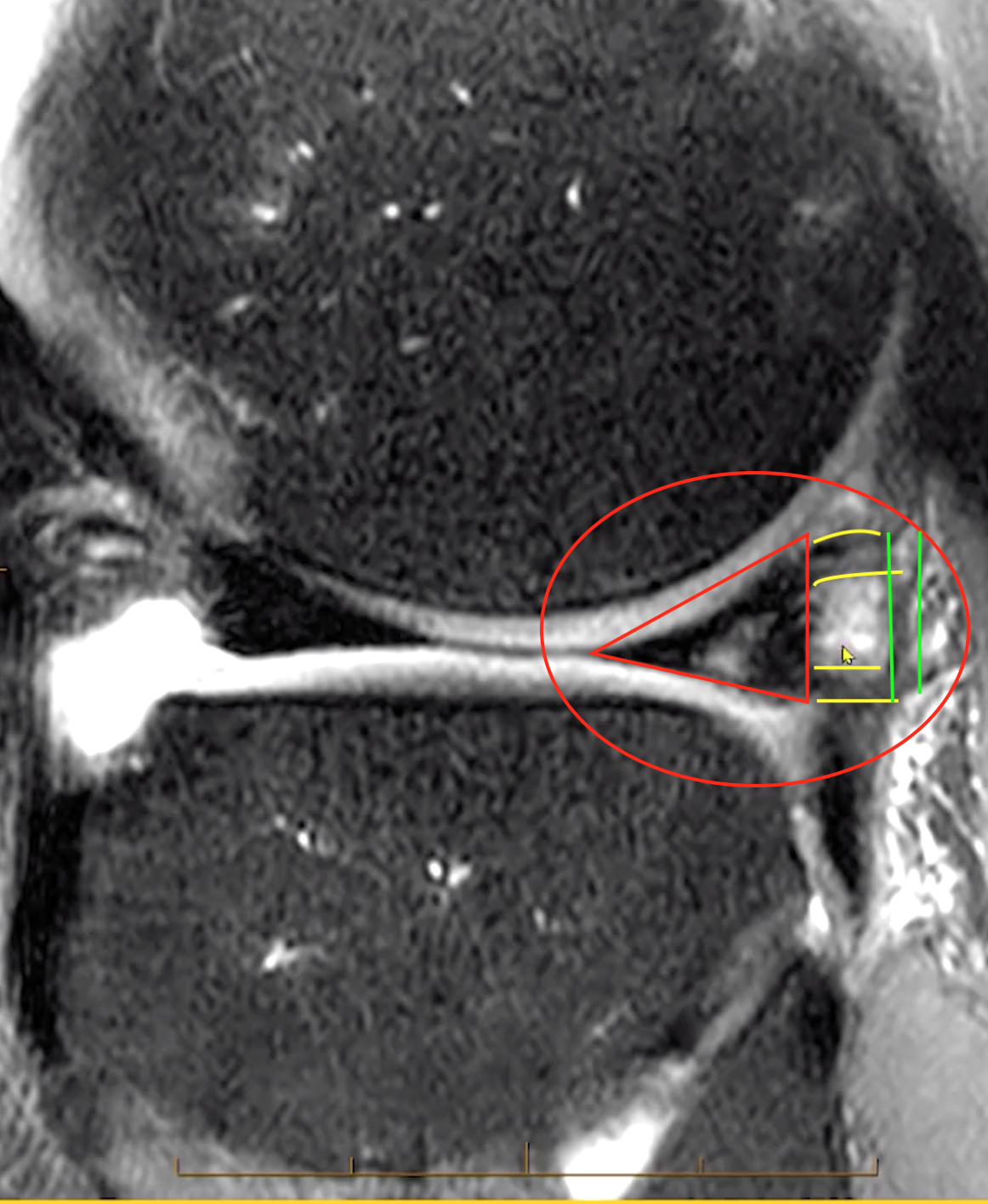
Ligamentum mucosa injury (red circle)
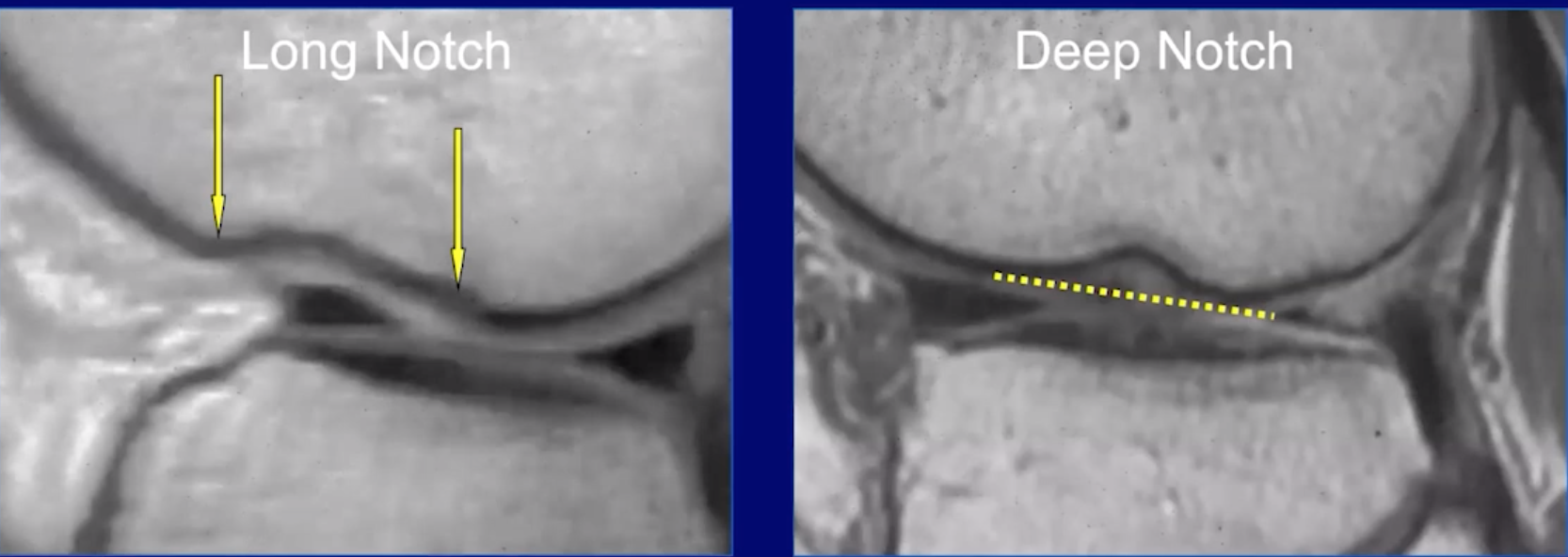
Notch sign
Deepening of the normal groove in the lateral femoral condyle
> 2mm is diagnostic of acute or chronic tear
Wrinkled tibia sign
Fracture of posterior aspect of the lateral tibial plateau
Avulsion fractures that should raise high suspicion for concurrent ACL injury
Semi-membranosus avulsion fracture
Tibial eminence (Meyers/McKeever classification system)
Segond fracture
Injury
Comment on if root ligament is affected
Axial
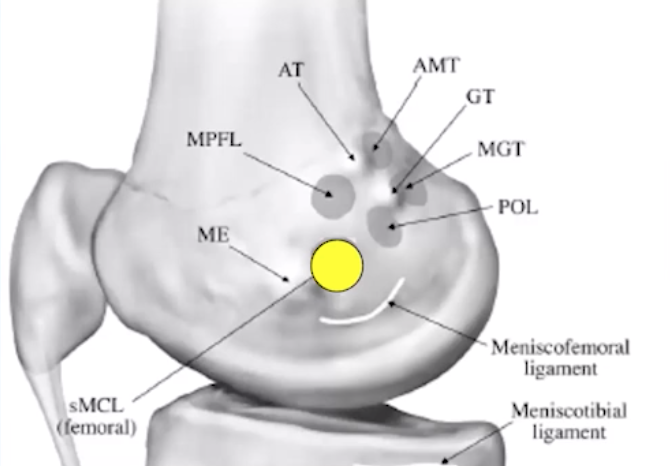
Medial Knee Stabilizers
Posterior Medial corner
Semimembranosus tendon (5 arms)
Knee Capsule
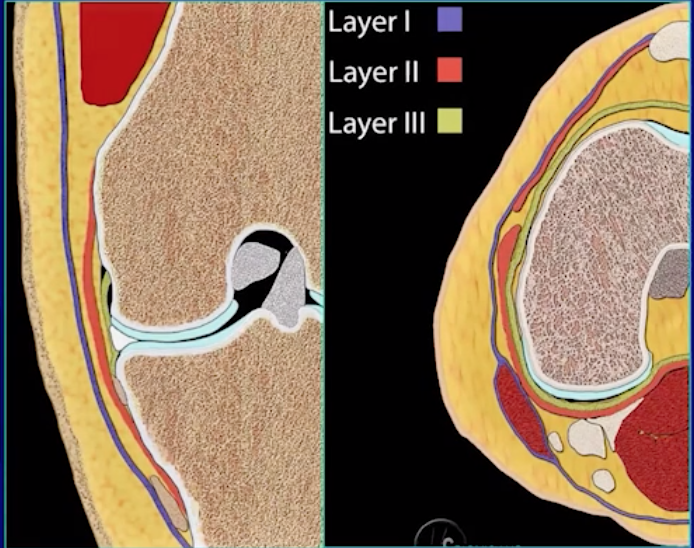
Medial Knee Stabilizers
Can be thought of in 2 ways, layers or thirds
Layers
Layer 1 = fascia
Layer 2 = Superficial MCL
Layer 3 = Deep MCL and capsule
Issue here is that many of these will fuse
Anteriorly layers 1 & 2 fuse to medial retinaculum
Posteriorly 2 & 3 fuse to posterior oblique ligament
Thirds
Anterior third = Medial retinacular ligaments + Pes Anserinus
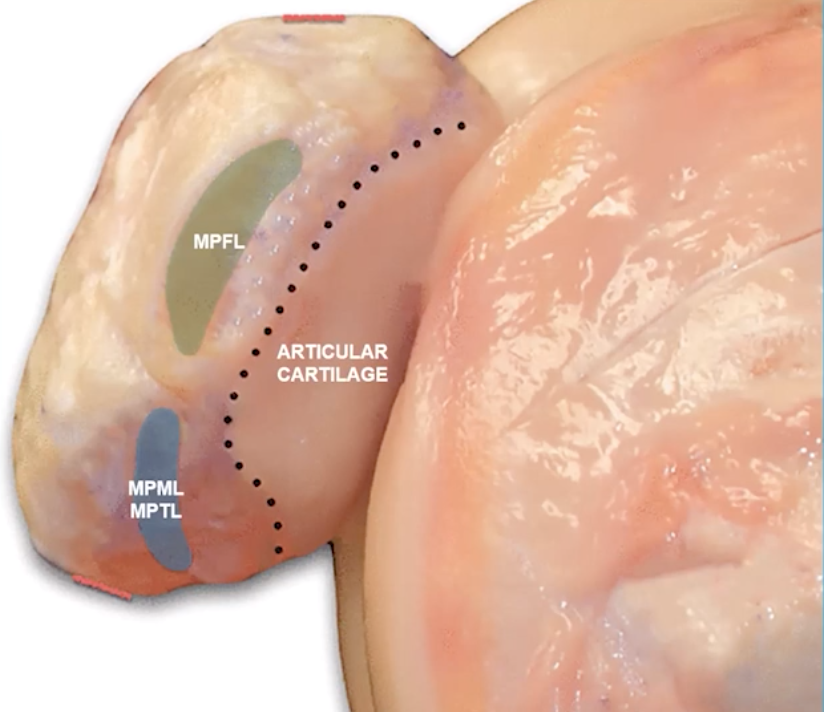
Medial patellofemoral ligament
Attaches from medial patella to the tibial collateral ligament (TCL) (medial collateral ligament)
Fibers attach to the inferior aspect of the vastus medialis muscle
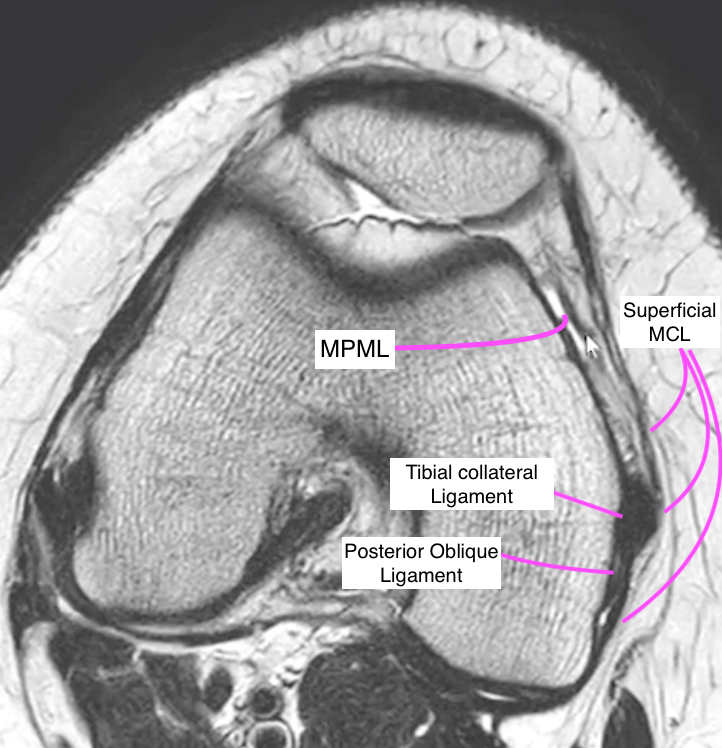
Medial patellomeniscal ligament
Extends from medial patella along an inferior-oblique path to the anterior horn of the medial meniscus
Medial patellotibial ligament (MPTL)
Extends from medial patella along an inferior-oblique path to the anterior surface of the medial tibial plateau
Pes Anserinus = goose foot
SAGS = from superior to inferior
SArtorius
Gracilis
Semotendinosis
There is a pes anserine bursa located deep to these tendons
Middle third
Superficial & Deep MCL
Medial capsular ligament
Posterior third
Posterior oblique ligament
Oblique popliteal ligament
Semimembranosis complex
Lateral Collateral Ligament
Fibular collateral ligament will merge with tendon of biceps femoris to form the conjoint tendon
Popliteus tendon also stabilizes lateral knee
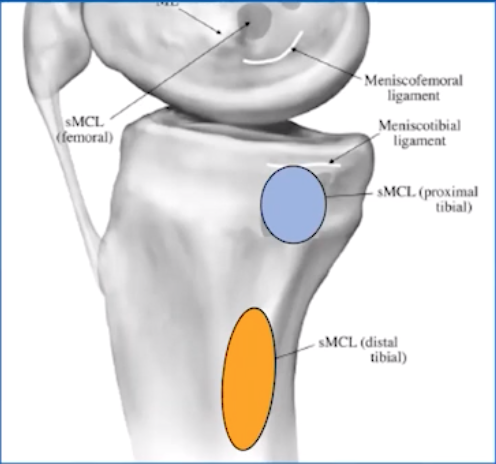
Medial Portion
Tibial collateral ligament (MCL)
One femoral (yellow) & 2 tibial attachments (blue and orange)
O’Donogue Triad
Complete ACL tear
Complete MCL tear
Medial meniscus tear
Tetrad? —> tear of medial patello-femoral ligament
Pentad? —> lateral meniscus tear
Caused by external rotation + flexion (valgus)
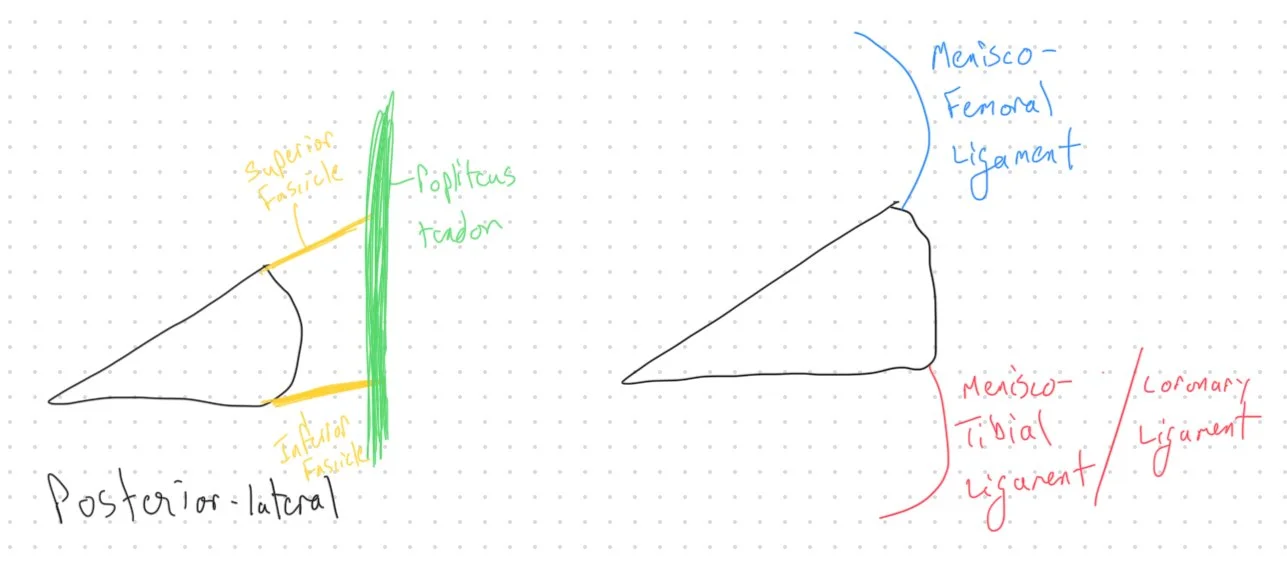
Deep Medial Capsular Ligament
Deep to the tibial collateral ligament
2 Parts
Meniscofemoral ligament
Meniscotibial ligament (coronary ligament)
Posterior Portion
Oblique Popliteal Ligament
Arises from semimembranosus tendon
Semimembranosus Tendon Complex
5 parts, who cares
Hoop stress
We need to think of the meniscus as a tub of toothpaste with a person squeezing the center of the toothpaste container
When we do this the toothpaste with clump up and push out on either side of the force pushing on the center
If the toothpaste container has the lid on then no toothpaste will spill out
This is the same thing as the meniscus
With the meniscus we have a piece of tissue that has a force being applied to the center of it resulting in clumping on the edges
The central force is the femoral condyle
The clumps of toothpaste within the jar are the meniscal triangles
The meniscus does not get forced out of the knee joint because we have ligaments keeping it in place (the toothpaste does not get spilled out because the cap is on)
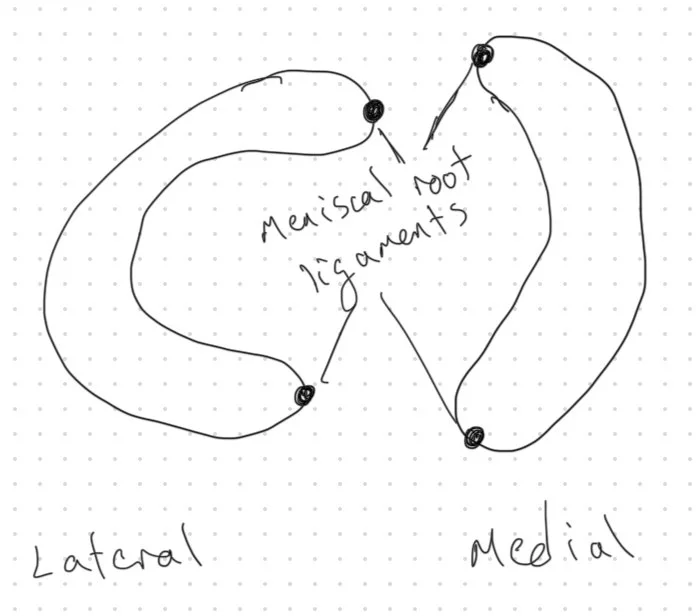
The root ligaments keep it in place medially
The menisco-femoral ligament and coronary ligament keep it in place laterally
If these ligaments are torn then the meniscus can float around and be unstable (the toothpaste lid is off and the toothpaste has fallen out of the container)
Lateral Meniscus
C shaped
Attachments are looser
Anterior-lateral meniscus has interdigitations of the fibers which look like linear bright lines and are normal appearance of the fibers and commonly over called as a tear
Segond Fracture
Avulsion fracture of the lateral tibial plateau
Associated with ACL tears
Stener like Lesion
Tear of distal fibers of superficial MCL which are then displaced proximally relative to the pes anserine tendon
Has implications for delayed healing
Meniscus
Medial Meniscus
Banana shaped
Attachments are tighter —> more commonly injured
Meniscal ligaments
These ligaments below are easily seen on medial side and poorly seen on lateral side
Meniscofemoral ligament -
Attaches to superior corner of meniscus and moves superiorly to attach on femur
Can also attach to the capsular ligaments instead of directly to the femur
Meniscotibial ligament (coronary ligament) - attaches to inferior corner of meniscus and moves inferiorly to attach on tibia
Lateral
Posterior meniscotibial ligament injury is what causes a RAMP lesion
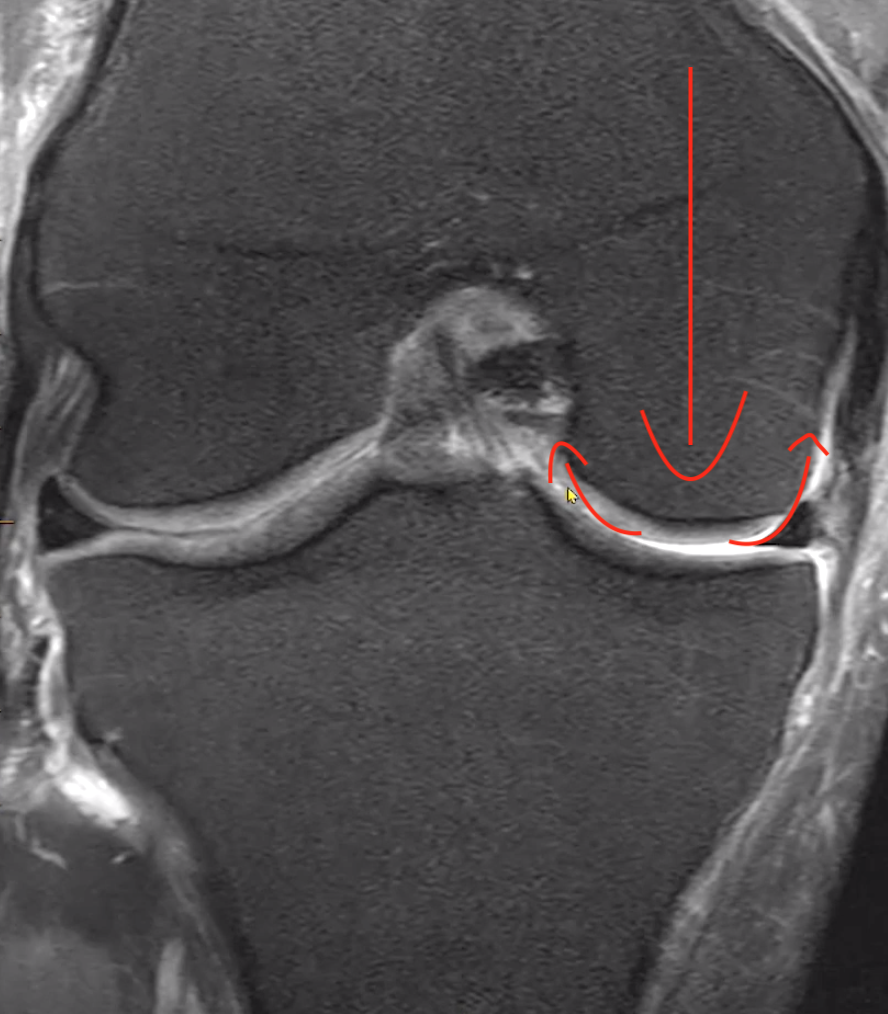
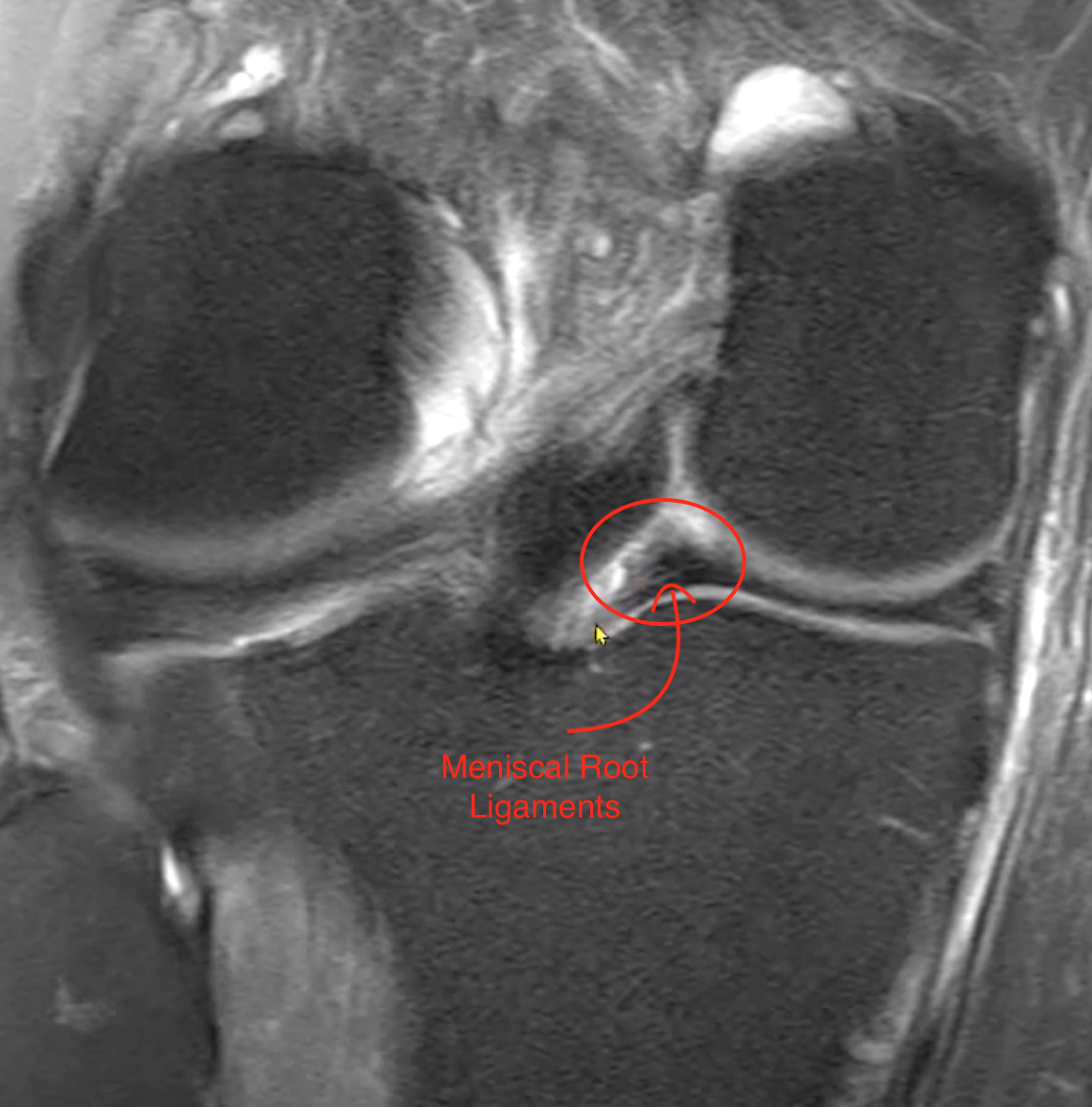
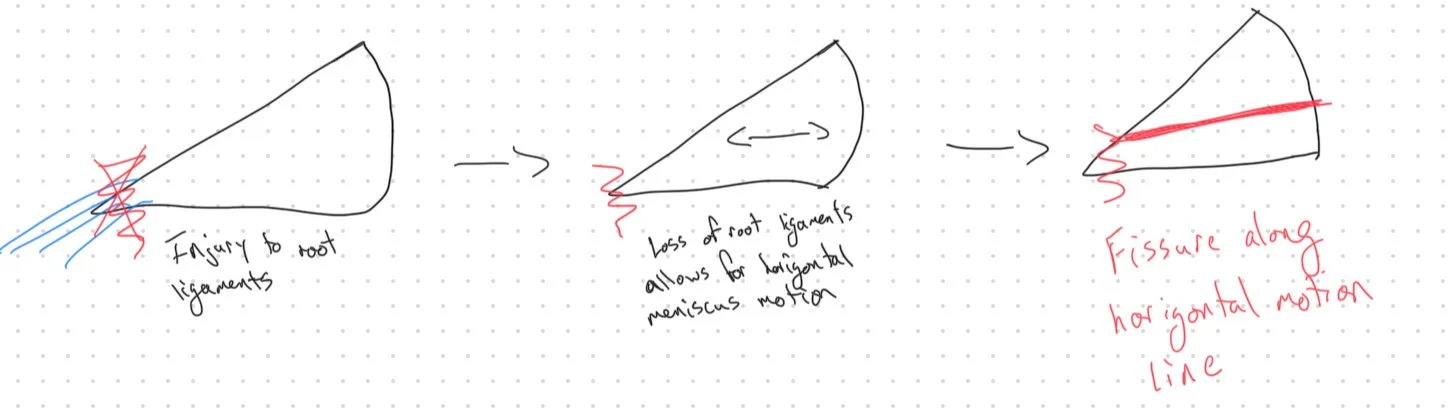
Meniscal root ligaments
Attach on anterior aspect of meniscus
Attach on posterior aspect of meniscus
Injury/tear of root ligaments can be from 3 major causes
Destruction of the ligaments themselves
Destruction of the medial tip of the meniscus where they attach
Destruction of underlying bone which basically avulses
When this happens the meniscus medial attachment will be lost and will allow the meniscus to sway medial and laterally which can result in protrusion
Additionally the recurrent sway medial and lateral causes a horizontal fissure within the meniscus which may they extend to the medial border where the original injury to the root ligament started
Discoid Meniscus
Coronal width >14 mm or
3+ sagittal 5mm images
Lateral > medial
More common
Horizontal tears
Single/double radial tears
Central hole tears
Roman candle/firework sign
Meniscus Extrusion
Meniscal extrusion is diagnosed as the mensicus relative to the tibia, not the femur
Medial meniscus
The meniscus and tibia should be directly in line an any extrusion of the meniscus past the lateral aspect of the tibia is abnormal
Lateral meniscus
Can have minimal (1 mm or less) beyond the lateral tibial plateau and be normal
CPPD
Punctate calcs within the meniscus
Correlate with radiographs
Gout
MSU crystals like
Popliteus tendon
Cruciate region
Extensors
Deposition in meniscus will be along the border of meniscus and tibia like a line of icing
Called “icing” the meniscus
Meniscal Tears
Look for two things to determine if there is meniscal injury (assuming no prior surgery)
Abnormal meniscal shape/contour
Abnormal meniscal signal
Two slice touch rule
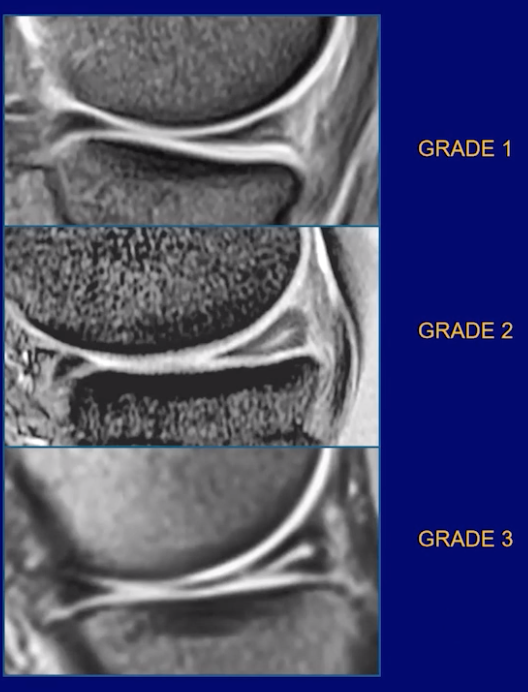
Need abnormal signal contacting the meniscal surface on 2 slices in one or more planes
Not all signal is pathology —> the intensity of the signal matters too —> see image
Grade 1 —> likely normal
Grade 2 —> likely degenerative shit
Grade 3 —> likely tear
If you see increased signal, these findings would make you think it is more benign
Fades by the middle and near complete absent in the inner third
Horizontally oriented
Ok if it extends to the capsular surface = lateral edge of triangle (not ok if it extends to the articular surface = top and bottom)
Not as bright as hyaline cartilage
Is there adjacent swelling, bone contusion
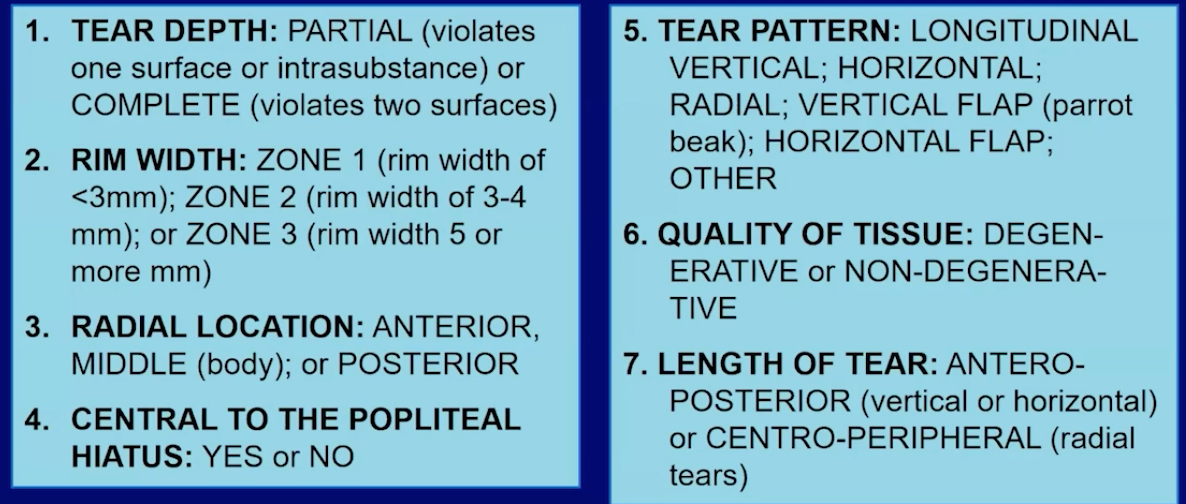
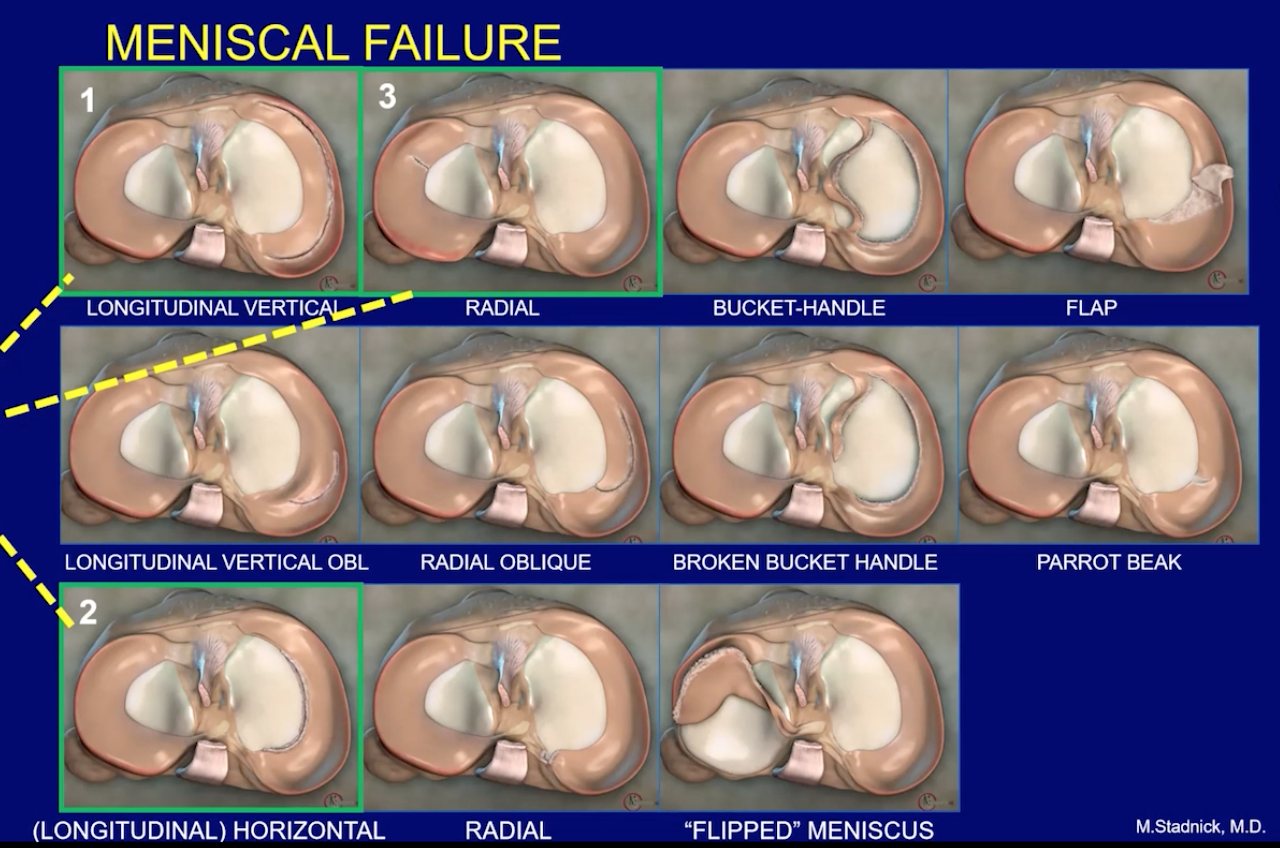
Longitudinal Vertical Tears
Up and down tear
Note, they can have some angulation to them
And the up and down orientation really applies to the sagittal view, they may look horizontal on the coronal view
Will be in the same location as your scroll through
If the tear moves in the anterior-posterior direction as your scroll through it is considered a longitudinal oblique
Longitudinal Vertical tear of Posterior horn of lateral meniscus
Especially important because near the popliteal hiatus this area of meniscus does not have a red zone
So worse healing i guess? idk
Longitudinal Vertical tear of Posterior Horn of medial Meniscus = RAMP lesion
2 Major findings
Irregularity of posterior horn of medial meniscus
Fluid filling between posterior horn of medial meniscus and capsule
Look for marrow edema in the tibia adjacent to the posterior horn of the medial meniscus
Highly associated with ACL injury
Meniscal Flounce
Longitudinal Horizontal Tears (Circumferential horizontal, aka Horizontal tear, aka Cleavage tears)
More commonly seen in older people from meniscal degeneration
Starts along the medial aspect of the meniscus and cuts the triangle horizontally into two triangles that are connected at the lateral most aspect (unless later on it fucks that up too) and creates a fish mouth appearance —> looks like duck beak more to me
Highly associated with parameniscal ganglion cyst (middle pic)
More likely seen on medial sign
Can erode bone when they get large
Note: Can have a cyst without meniscal tear
Note in kids
Parameniscal ganglion cyst at the anterior horn of the lateral meniscs with additional inflammatory changes in Hoffa fat pad has been well described in kids WITHOUT an associated meniscal tear
Central cavitation
Looks like a tube of fluid within the meniscus almost
This is a longitudinal horizontal tear seen in discoid menisci (pic all the way to right)
Truncated Meniscus
Meniscus does not have normal triangle shape and likely has a flattened medial aspect instead

Bucket Handle Tear
Double PCL sign
Double meniscus sign
Pseudo-bucket handle lesions
Anomalous meniscal ligament
Ruptured ACL

Arcuate Sign
Avulsion fracture of the fibular head by the LCL (fibular collateral ligament) or biceps femoris tendon
Associated with PCL > ACL tears
Pelligrini-Steida Lesion
Post-traumatic calcification at the medial femoral condyle
Calcification may be of
MCL
Adductor magnus tendon
Patellofemoral disorders
Mildly increased edema within Hoffa fat —> sign of patellar maltracking
Patellar Dislocation & Auto-Reduction
Osseous contusions of the medial patella & lateral femoral condyle
Look for concurrent medial patellofemoral ligament and medial patellar retinaculum injuries
Comment on osteochondral defects
Look for loos osseous bodies in the joint space, may be small and subtle
Comment on depth of trochlear groove, if shallow likely will happen again
Valgus Injury
Force directed to lateral aspect of knee
Bone contusion on lateral aspect of knee
MCL is primary injruy
ACL & PCL are secondary injuries
Patterns of Injury
Resources: