Kidney
Xanthogranulomatous Pyelonephritis
RCC
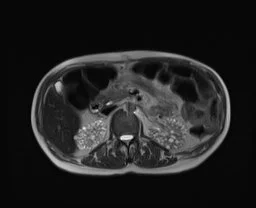
Lithium Nephrotoxicity
Basically multiple bilateral renal cysts
Duration of lithium therapy increases the risk of ESRD
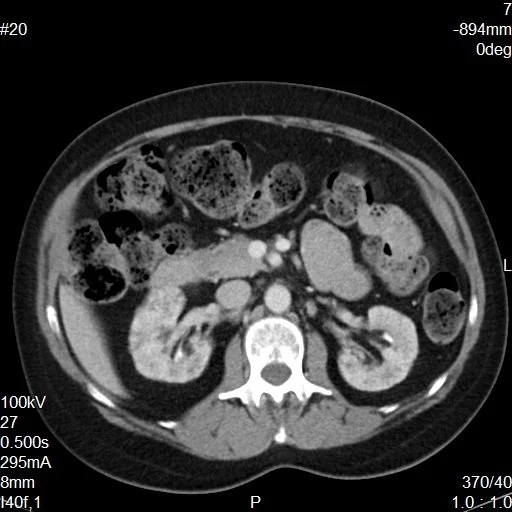
Renal Lipomatosis
Basically increased fat in the renal pelvis/hilum area, usually with cortical atrophy
Seen with age, obesity, etc.
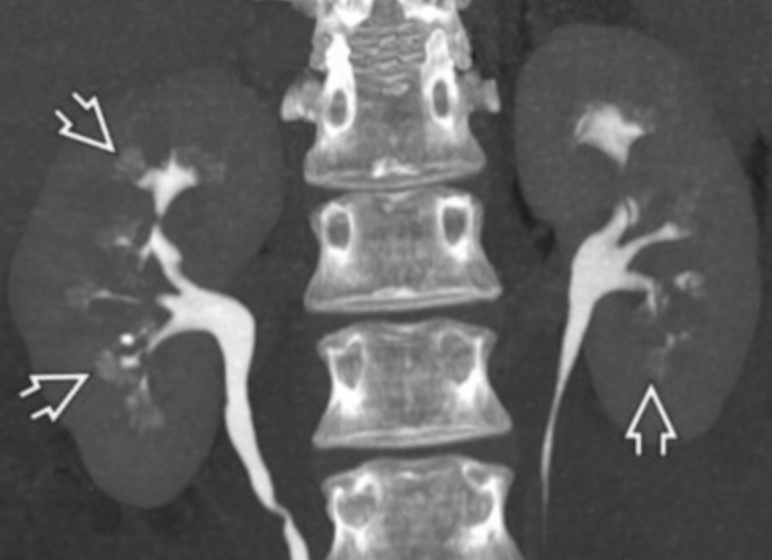
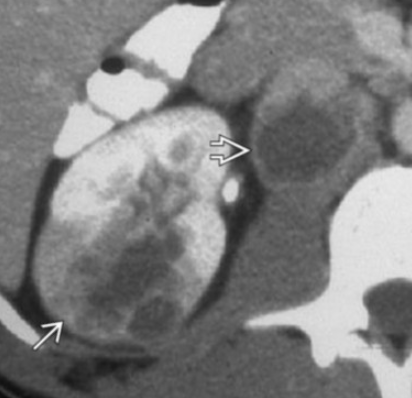
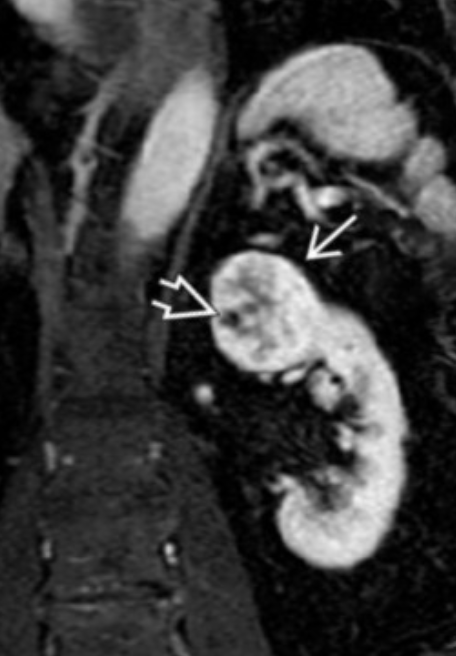
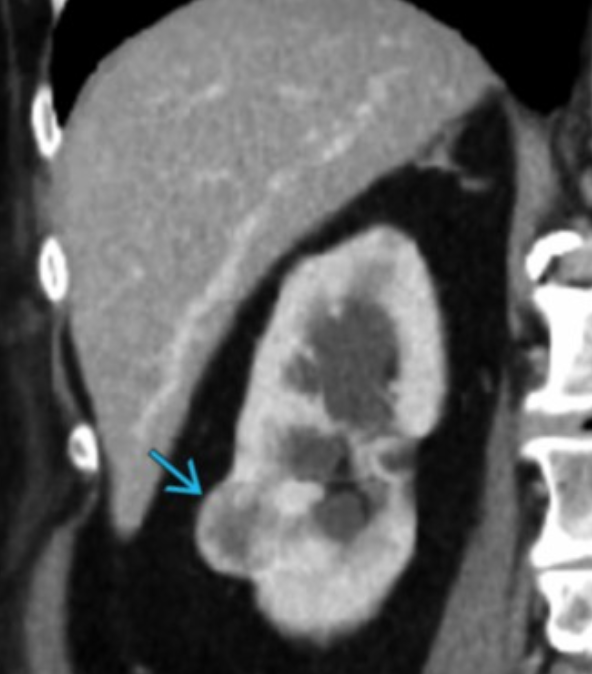
Medullary Sponge Kidney
Dilatation of medullary and papillary ducts
Commonly from tiny stones
Presents as recurrent renal colic/flank pain
In image below you see dilated ducts that the arrows point to and i guess normally you should not see them
Retroperitoneal Fibrosis
Literally fibrotic changes in the retroperitoneum typically for unknown cause/trigger although can be related to radiation, drugs, malignancy or pretty much anything else but vast majority of cases are idiopathic
Fibrotic changes results in compression of ureters and vasculature -
If there is displacement of the Aorta, IVC there should be concern for malignant etiology
Classically there should be encasement but no invasion of these structures
Maiden waist sign - medial deviation of the middle 1/3 of both ureters

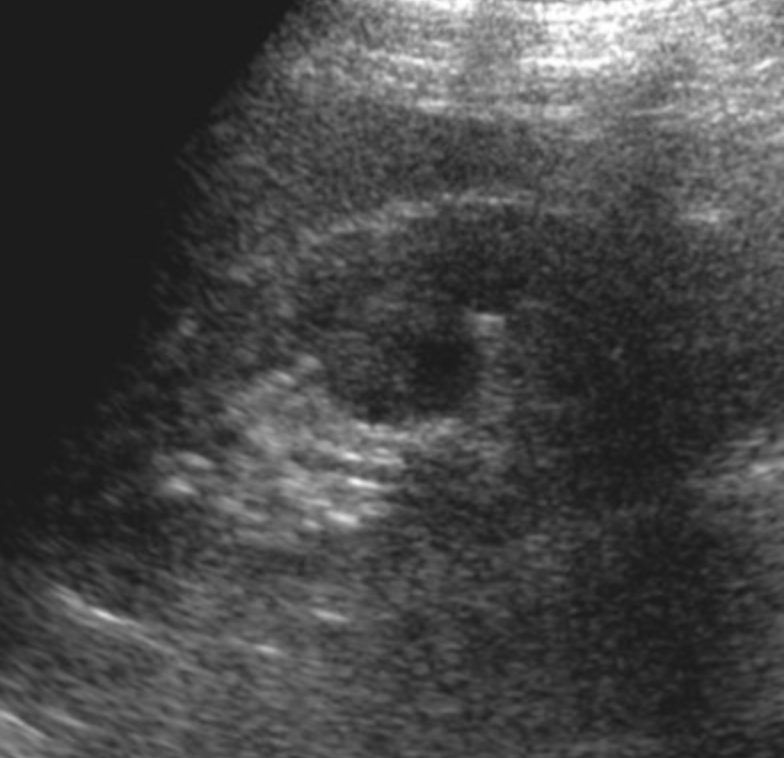
Hypertrophy of Column of Bertin
Refers to enlarged piece of renal cortex that protrudes through the medulla
Commonly mistaken for a renal mass
Isoechoic/Isointense/Isodense to renal cortex
Will show communication with the regular peripheral renal cortex
Usually unilateral and on the left
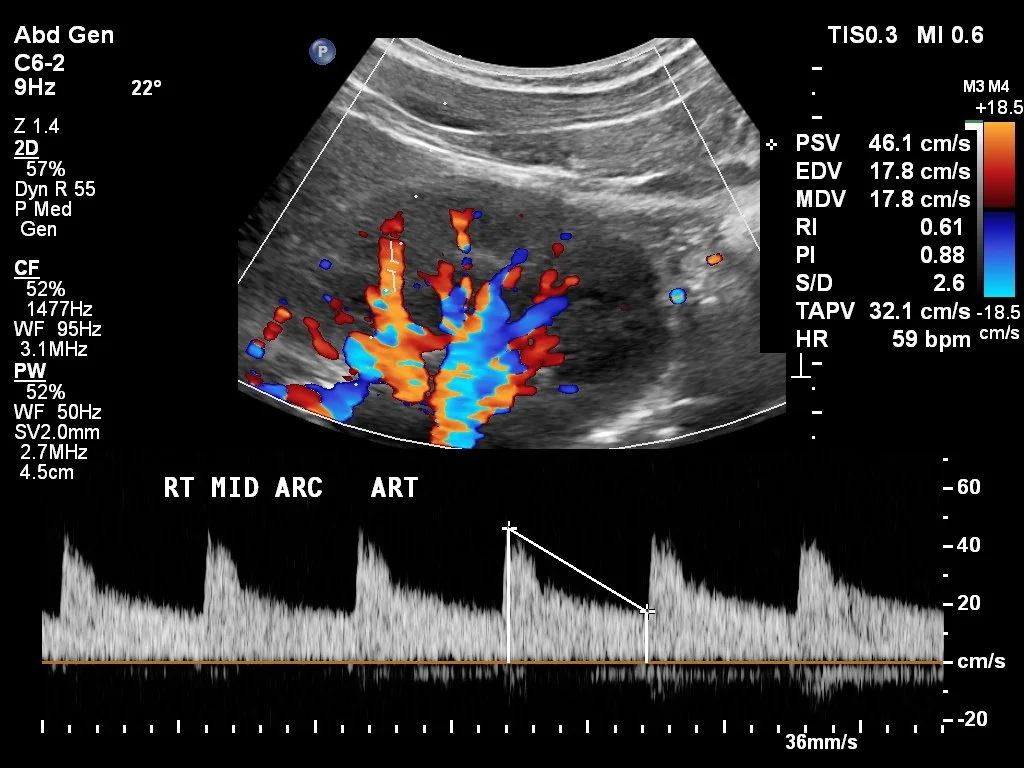

Renal Doppler

Ureterocele
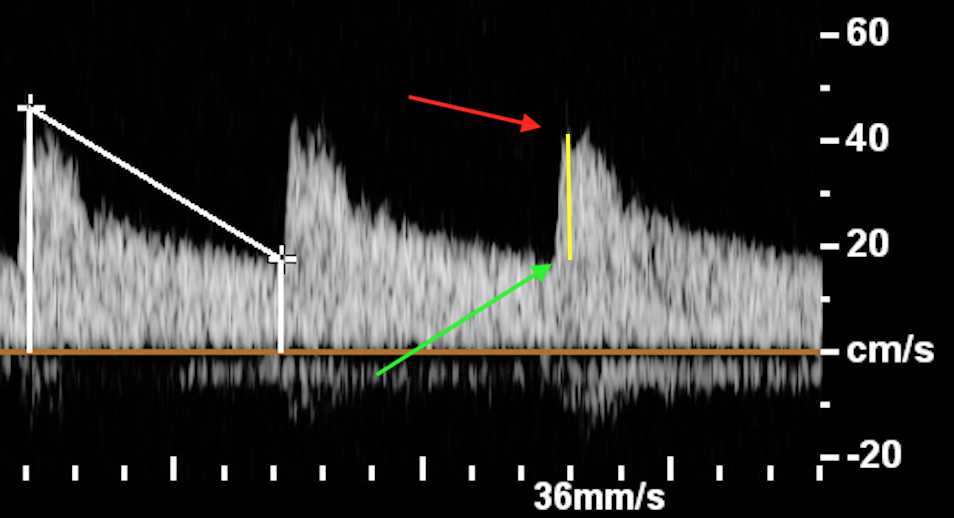
You need to check and make sure the “t” markers (as seen on first sequence in this photo) are at the top (red arrow) and bottom (green arrow) otherwise you will get wrong values.
The yellow line is the acceleration velocity and should be almost a straight line normally.
Renal Artery Stenosis US
Normal Values
PSV < 180 cm/s
Proximal renal artery to aorta velocity ration < 3.5:1
AT < 0.07
RI < 0.08 and <5% difference between the two kidneys
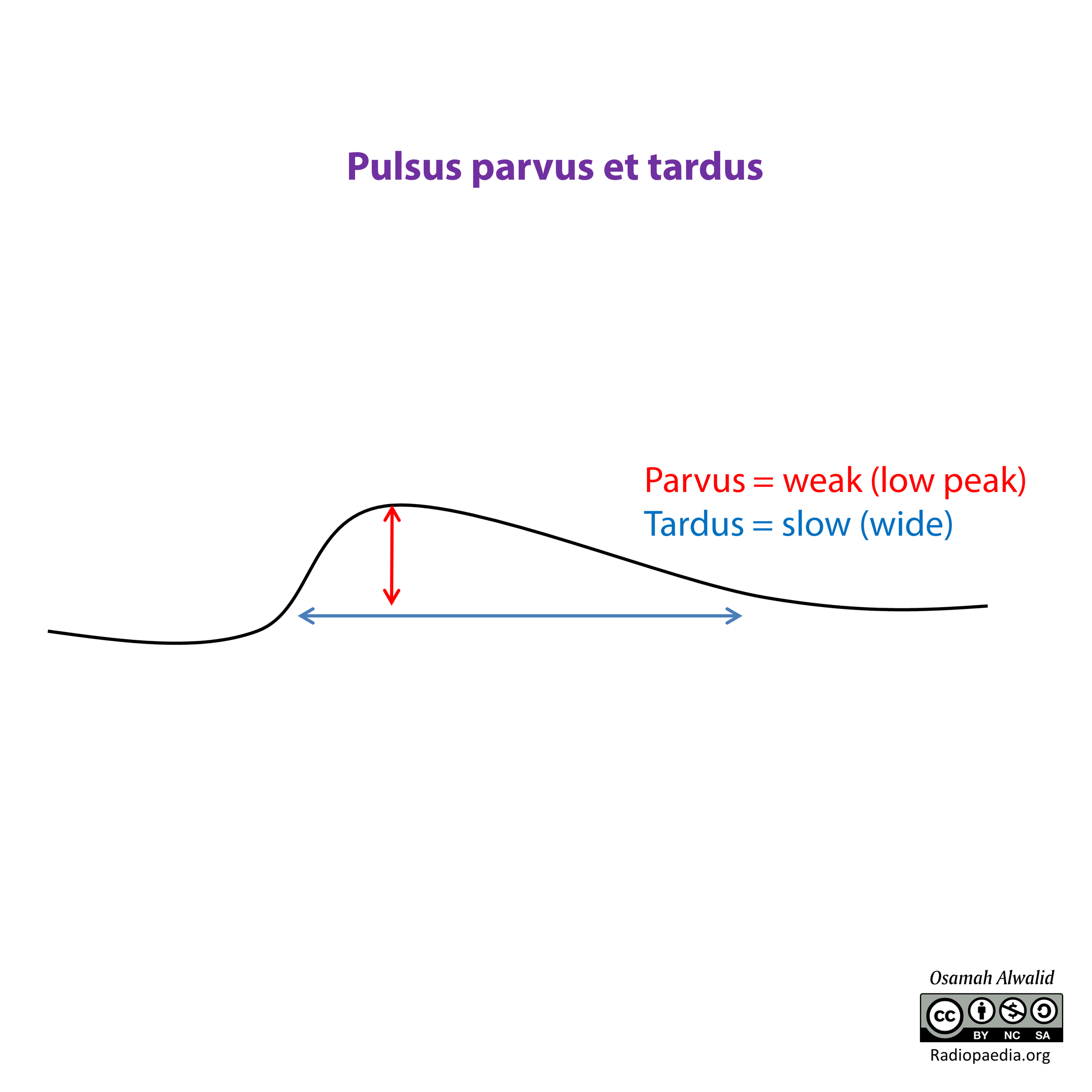
Waveform seen in arterial stenosis, including RAS.
There is a stenosis so it takes longer to reach the peak velocity as there is a huge roadblock.
It also takes longer to get back to baseline values simply because there is less flow overall.
Metabolic Disorders
Nutcracker Syndrome
Compression of the left renal vein between aorta and SMA
Can cause thrombosis, hematuria
Acquired Cystic Renal Disease
3+ cysts per kidney in patient with CKD
Typically in long term dialysis patients
Mildly increased risk of RCC - however the RCC that occurs tends to be less aggressive
Metastatic Disease
Bronchogenic carcinoma is one of the most common causes of metastatic disease to the kidney
Renal Masses
Renal Medullary Carcinoma
Aggressive cancer
Really only seen in young males with sickle cell trait
Looks like infiltrative mass/ill defined area of hypoattenuation on CT similar to how diffuse gliomas look where there is no actual focal mass just this amorphous shit infiltrating the organ
Oncocytoma
Benign mass
Central scar
No invasion of adjacent structures
No hemorrhage or necrosis (is seen in RCC)
Cannot definitively differentiate from RCC on imaging alone
Note that just because a biopsy shows oncocytes does not mean it is benign, malignant masses can have oncocytes too, don’t assume presence of oncocytes means it is an oncocytoma
References:
Case courtesy of Tom Foster, Radiopaedia.org, rID: 151112 (lithium renal disease)
Case courtesy of Pablo Lorenzzoni, Radiopaedia.org, rID: 70005 (lithium renal disease)
https://link.springer.com/article/10.1007/s00261-018-01890-4 (maiden waist sign)
Case courtesy of Bruno Di Muzio, Radiopaedia.org, rID: 27754 (column of bertin)
Case courtesy of Dennis Odhiambo Agolah, Radiopaedia.org, rID: 99867 (Renal Doppler)
Case courtesy of Osamah A. A. Alwalid, Radiopaedia.org, rID: 61414