HIV Neurologic Disease
Cryptococcus
Infection in immunocompromised patients, 2/3 of cases in patients with HIV
Seen when CD4 < 100
Clinical Presentation - Headaches is most common symptom, basically can present with any neuro issues, would suspect in HIV+ pt with new neuro symptoms
3 major findings - each affecting a different space
Cryptococcomas -
Basically small fungus balls - affects parenchyma
T1 - hypointense
T2 & FLAIR - hyperintense
T1 C+ & DWI - varies too much, can see multiple things
Meningitis - affects meninges
Affects both leptomeninges and pachymeninges
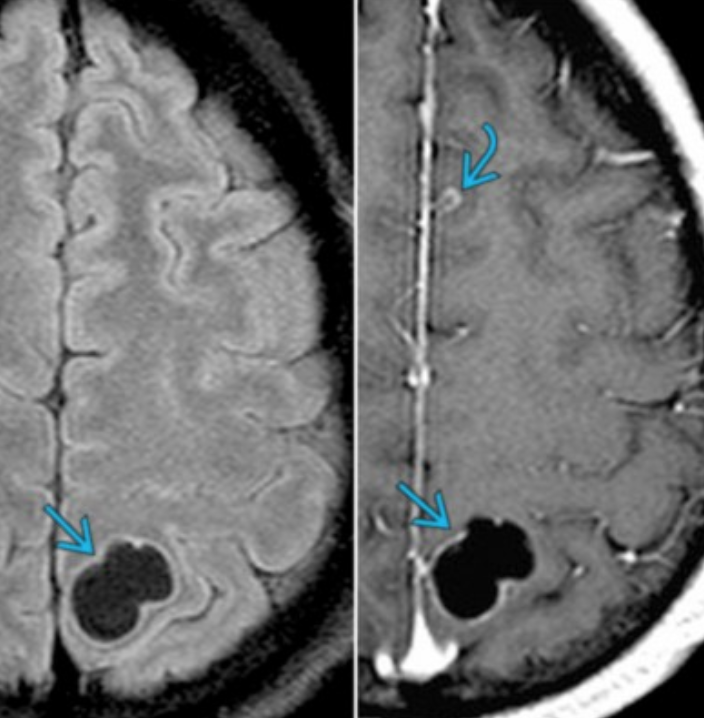
Dilation of Peri-vascular spaces
Dilation of perivascular spaces allows for them to merge and form large empty spaces that can then form gelatinous pseudocysts
These gelatinous spaces are what gives the classic soap bubble finding
Can result in infarction
T1 - hypointense
T2 & FLAIR - hyperintense
T1 C+ & DWI - varies too much, can see multiple things
Historically - non-enhancing lesions seen -ART drugs were bad - immune system was destroyed
Recent times -Enhancing lesions seen - ART drugs are better - immune system can make a comeback
HSV Encephalitis
Caused by HSV-1
Imaging findings
Asymmetric lesions, prefers limbic system and temporal lobes
Spares basal ganglia (note MCA infarct may look similar but will affect basal ganglia)
T1 C+ - patchy enhancement, gyriform enhancement later
T2 - cortical/subcortical hyperintensities with white matter sparing
DWI - restricted diffusion (may see findings on DWI before other sequences)
Treatment - IV acyclovir immediately
Neurocysticercosis
Caused by Taenia solium
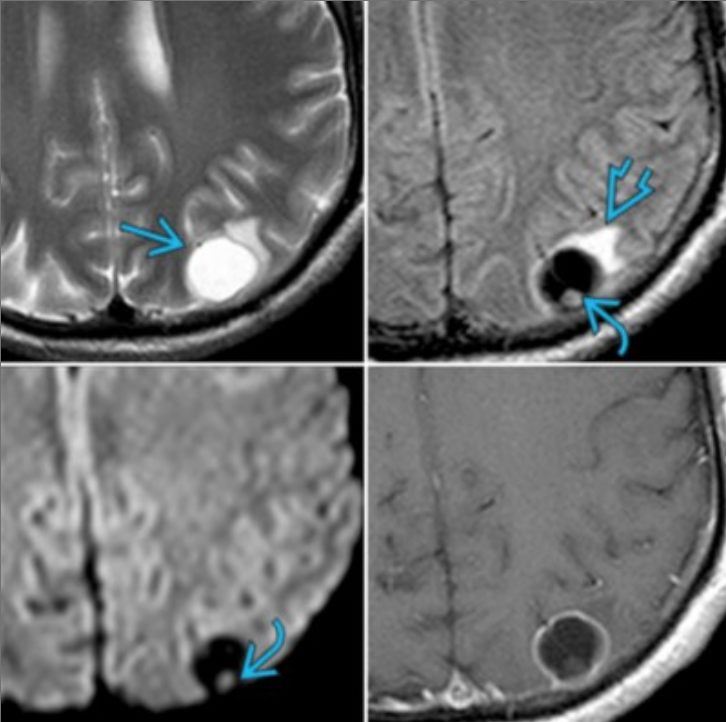
Cystic lesion with dot in the center
Other presentation is multiple grape like (racemose) lesions clustered together (top right image)
4 stages
Vesicular (top left)
Indicates visible larva
Smooth, thin-walled cyst, isodense to CSF, no edema
Hyperdense dot within cyst = protoscolex
Colloid Vesicular (Middle)
Hyperintense cyst with edema
Ring enhancing fibrous capsule
Indicates Dying larva
Granular nodular
Healing stage
Nodular calcified
Healed stage
Calcified dot
Can have lesions at different stages at same time
MR spectroscopy
↑ lactate, alanine, succinate, choline
↓ NAA and Cr

Neurosyphilis
Acute neurosyphilis
Leptomeningeal enhancement
Syphilic gummas - focal nodules adjacent to meninges -> low T1, high T2, enhance & restrict diffusion, may have dural tail sign
Meningomyelitis - long segment T2 hyperintensity, usually in thoracic cord
Later neurosyphilis
Tabes Dorsalis - cord atrophy and T2 hyperintensity of the dorsal columns (difficult to differentiate from SCID)
Vascular findings
Arteritis with concentric wall thickening and possible vascular beading
Abscess
Rim enhancing lesions which is vague but will have other features to help identify it as an abscess such as:
Strong restricted diffusion
Dural rim sign - outer hypointense rim with adjacent inner hyperintense rim