Head & Neck Masses
Choleosteatoma
Basically ball of keratin similar to epidermoid cyst
Can erode into bone, typically temporal bone - caution for tympanic membrane perforation
Broadly grouped based on acquired (98%) or congenital (2%)
Acquired choleosteatomas
Two major types of acquired
Pars flaccida
Expands into prussak space
Displace the ossicles medially
Pars tensa
Displaces ossicles laterally
T1 hypointense, T2 hyperintense, non-enhancing, will restrict diffusion
Usually seen near mastoid air cells and tympanic membrane
Cholesterol Granuloma
Aka blue dome cyts, chocolate cyst of ear
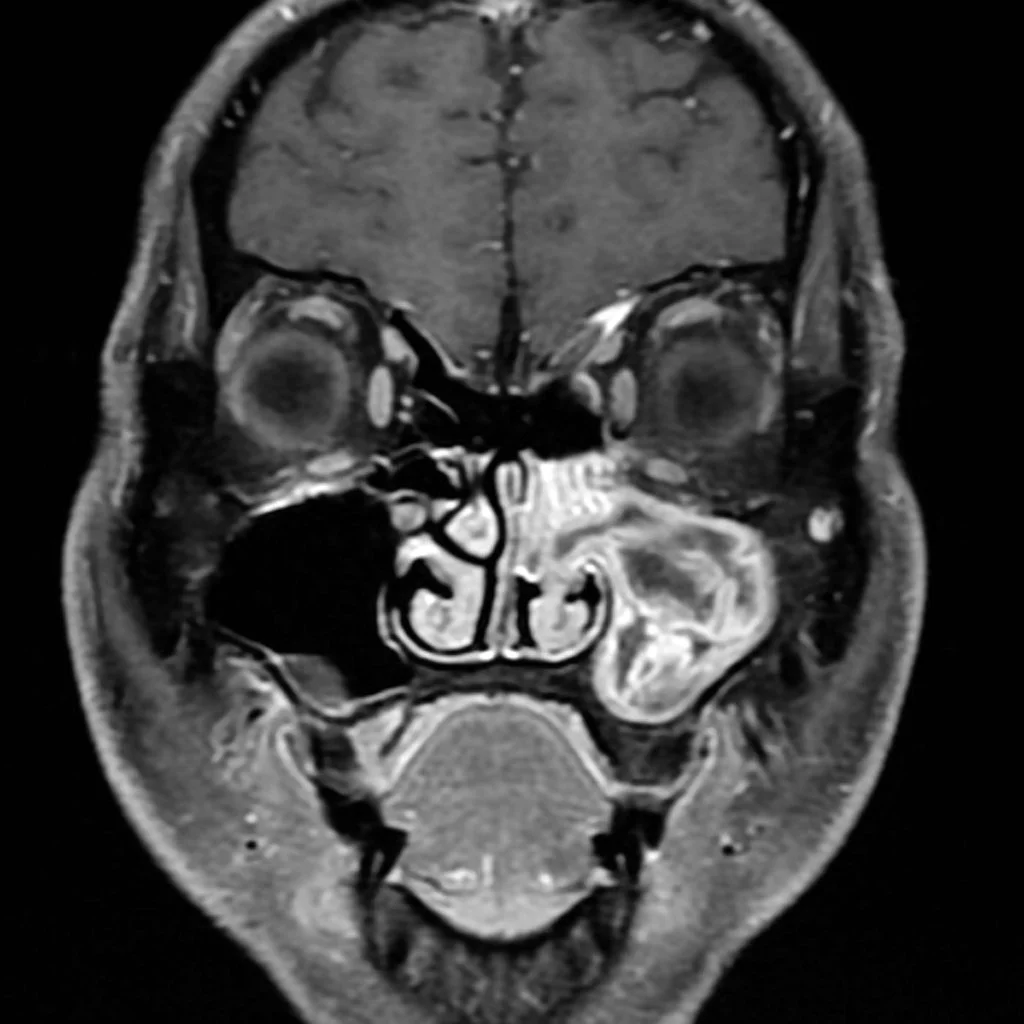
Inverted Papilloma
Non-cancerous sinonasal mass that rarely has malignant transformation
Presentation/Imaging
Typically middle aged men
Lateral wall of nasal cavity most commonly
Bony remodeling
Convoluted cerebriform pattern (alternating stripes of high and low intensity on MR)
T1: Isointense to muscle, heterogenous enhancement
T2: hyperintense to muscle
Carotid body paraganglioma
Hypervascular mass in carotid space which splays the internal and external carotid arteries
Early washout
May have salt/pepper on MR
Salt = increased signal from hemorrhages (not a common finding)
Pepper = flow voids from vascularity - serpentine or punctate flow voids
Hypoechoic and vascular on US
Unilateral, may be bilateral in inherited syndromes
If multiple look for:
VHL
MEN-2A
NF-1
Paraganglioma syndromes
DDx
RCC mets - although these will not be symmetric and typically not in carotid space
Hemangiopericytoma - very rare, these will be a singular mass
Schwannoma - these will not splay the carotid arteries, less dense and less enhancement than paraganglioma
Shamblin grading system - who cares
Tx - cut it out
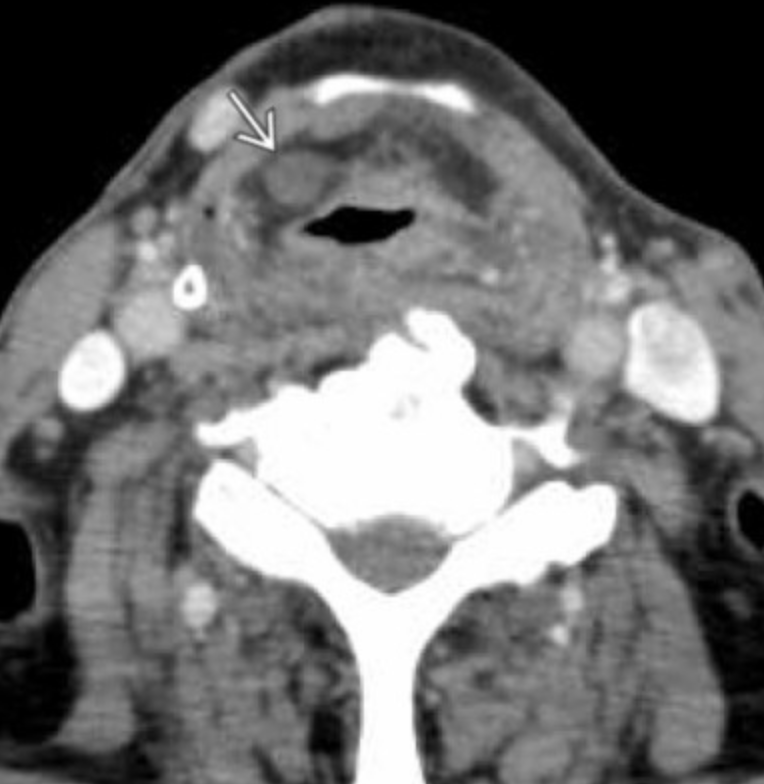
Thyroglossal duct cyst
Midline neck cyst
Can occur anywhere at midline from base of tongue to thyroid gland
Thyroglossal duct is basically a highway for thyroid gland to follow
Starts at foramen cecum —> anterior to hyoid —> moves under hyoid bone in pre-epiglottic space —> deep to strap muscles
Should normally go away in 5/6th weeks gestation
If persists then cysts can form due to persistent secretion from epithelial cells of the remaining duct
Bronchogenic Cyst
Classically in the sub-carina mediastinum
Esophageal Duplication cysts
Mediastinal cyst that is contiguous with the esophagus
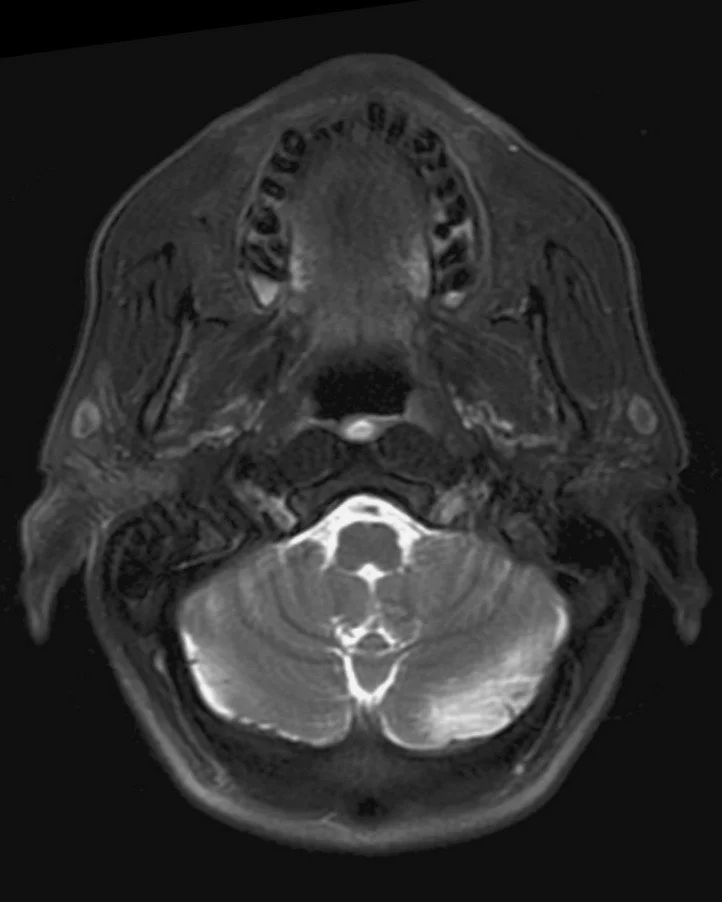
Tornwaldt Cyst
Benign cyst in mucosal space, remnant of notochord tissue
T1- variable
T2 - hyperintense
Does not enhance
Typically no treatment needed

Sinus Lesion with Osseous Erosions
Squamous cell carinoma
Fungal sinusitis
Enthesioneuroblastoma
Non-Hodgkin lymphoma
Most common
Squamous cell carinoma
Fungal sinusitis
Enthesioneuroblastoma
Non-Hodgkin lymphoma
Squamous Cell Carcinoma
Most commonly arises from maxillary antrum
Necrosis & hemorrhage
Less common
Wegeners
Adenocarcinoma (sinus)
Sarcoidosis
Rhabdomyosarcoma
Adenoid cystic carcinoma
Undifferentiated sinonasal carcinoma
Fungal Sinusitis
Immunocompromised
Aspergillus & Mucormycosis
Sinus Lesion No Osseous Destruction
Antrochoanal Polyp
Laryngocele
Unilateral, thin walled fluid (or air) collections in paraglottic space
Paraglottic space is basically anterior and lateral to pharynx/larynx
If infected —>pyolaryngocele
Secondary laryngocele
There is another obstructive lesion inferiorly which causes laryngeal obstruction and formation of a laryngocele superior to the obstructive lesion
Obstructive lesion may be SCC so be sure to look for this if you see a laryngocele
Branchial Cleft Cyst
Lateral neck cyst
Type 2 = most common
Make sure this is not a necrotic node - could be malignancy
Adenocarcinoma
Can arise from ethmoid sinuses
Rare
Osteosarcoma
Chondrosarcoma
Langerhans histiocytosis
Metastasis
Enthesioneuroblastoma
Age peaks: 11-20 yo & 50-60 yo
Aspergillus & Mucormycosis
References:
Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 9399 (inverted papilloma)