Fluoro Procedures
Contrast Agents
Barium
Pros:
Gives best images
Cons:
Cannot use if there is concern for perforation or leak due to risk of mediastinitis/peritonitis, etc.
Gastrograffin
Pros:
Water soluble can be used if there is concern for leak or perforation
Cons:
Omnipaque (Iohexol)
Pros:
Can be used i
Cons:
Can only use 150 ml
Expensive
Arthrogram Shoulder
Cocktail ~12 cc
MRI
0.1 cc gadolinium
5 cc omnipaque
15 cc saline
CT
8cc omnipaque
~8 of other shit i guess
Small Bowel Follow Through:
Indications
Bowel Obstruction
Steps
Pre-op plain AP film to asses for
Ensure NG tube is in proper position
Most patients will have this procedure ordered for obstruction so they will usually already have an NG tube
Ensure no evidence of perforation (air under diaphragm)
Residual contrast from prior procedure
Obtain multiple films 15 min, 30 min, 1 hour, and so on until contrast is visualized in the large bowel/colon - look for haustra!
Once contrast is visualized in the colon/large bowel you are done and no longer need to get new pictures
Esophagram
Indications
Steps
Give sip of THIN contrast and check for aspiration - if patient aspirates then you are done
Give fizzies with water and allow this to distend stomach - tell patient to resist urge to burp
Give THICK contrast and take pictures (sine) in the following positions
AP
RPO
LPO
Single lateral (doesn’t matter if right or left)
If checking for reflux do the following steps
Lay patient down in RAO (stomach down, left leg bent up, right leg straight
Give patient one sip of THIN contrast and follow the esophagus to evaluate peristalsis flow while taking sine
Give patient multiple continuous sips of contrast to try and overload the stomach and focus on GE junction to see if there is reflux
Give barium pill with water and take sine
Cystogram
Indications
Evaluate for bladder leak (commonly done after prostatectomy)
Patient will have a foley catheter in place for injection of contrast
Steps
Inject 150 ml of contrast (maximum amount to be used) and take non-sine periodically to ensure contrast is actually filling in the bladder
Take non-sine in the following postions
AP
Right lateral
Left lateral (get femurs to overlie each other = good lateral)
Oblique (doesn’t matter which side)
Done
Modified Barium Swallow
Indications
Steps
Give several different mediums (cracker, apple sauce, liquids etc.) each with contrast added to them and take non-sines while eating/drinking to look for aspiration
Many times it is performed with speech therapy
Done
Urethrogram
Indications
Steps
Sterile procedure so will need to don gloves and prep & drape area
Inject contrast via pediatric catheter or directly from syringe into penis
Take sine while injecting contrast and evaluate for contrast to reach the distal urethra
Done
Upper GI Series
Indications
Need to see upper esophagus down to the duodenum and need to specifically see where the duodenum crosses midline
Steps
Esophagram
If doing in a kid or adult laying down, have patient lay on left lateral view while evaluating esophagus this way contrast stays within the stomach while doing the esophagram and does not pass into the duodenum which is the major thing you want to watch
Lay patient down and take lateral, RAO, LAO and evaluate stomach and duodenum
Duodenal roll - patient right side down and rapid rotation to supine position as bowel fills for the first time - allows you to see the duodenal-jejunal junction
Should be done as a continuous fluoro video
Done
Retrograde Urethrogram
Prep penis and surrounding area
Want patient in oblique positioning to start
Lube the catheter
Insert catheter and inject contrast with holding catheter through the penis firmly
Inject contrast until you can see the bladder/proximal urethra
Ensure to take image with penis elongated (hold out to the side)
You will be taking fluoros, not sine/exposures
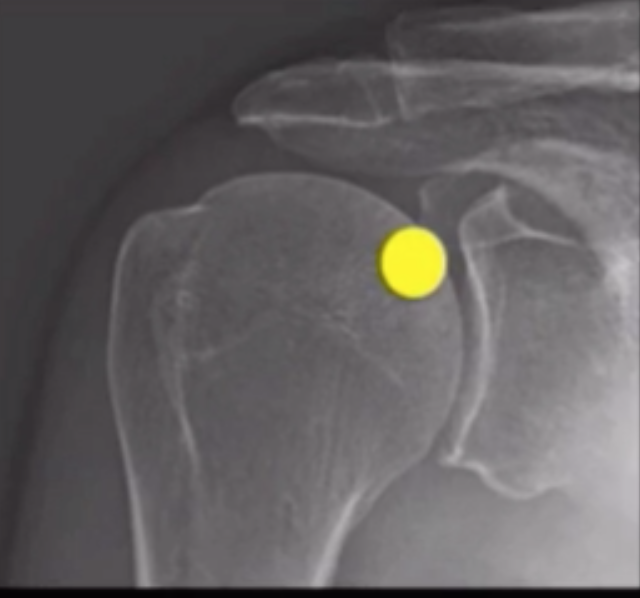
Arthrogram
Shoulder
Mix contrast agents - ratio used here is
15 ml NS : 5 ml omnipaque : 0.1 ml gadolinium
Position patient with arm externally rotated
Mark target location
Target area is upper and inner aspect of head of humerus
Ideally should be near level of coracoid?
Prep area
Numb skin
Drop needle in
Inject contrast - look to ensure contrast is within the joint space
Loopogram
Used to evaluate ileal conduit
pseudo-sterile - since dealing with open bowel essentially, it is not sterile but should wear sterile gloves and clean area with betadine
use omni
insert largest foley catheter you can into stoma
inject contrast
will likely need to inflate foley balloon and pinch insertion of tube into foley because contrast will push out otherwise
look for reflux of contrast into ureters and calyces
reflux is normal and what you want, if there is no reflux that is abnormal
take sine and stills
Fistulagram
Used to assess fistula (typically enterocutaneous fistula)
clean stoma
insert tube into stoma
inject contrast and see where the contrast goes
VCUG
Patient supine and inject contrast into the bladder - take spot fluoro as the bladder is filling
Take spot images as the bladder fills looking to see if there is any opacification of the ureters or kidneys (may look like dark bowel at first!)
Put lateral and check insertion site of the ureters if they are opacified
Keep spot fluoroing the bladder until patient starts to urinate
once they urinate you want to be fluoro-ing the urethra as they pee to see the contrast leave the urethra - need a fluoro image of the urethra
If everything was normal you will need to repeat this process again as sometimes first pass does not allow reflux to show adequately
This is typically only done for kids <1 yo in whom adequate distention was not achieved (i.e. <75 ml was given before voiding)
If you see bad reflux you likely do not need to repeat the whole process twice
Tips - can put patient lateral while in filling phase and take fluoro spot to look for ureteroceles
Tips - some say you need to remove foley while peeing because it artificially keeps urethra open which gives in accurate results, others say it is wrong to insert foley twice in a kid (stricture risk, traumatic, etc.)
Tips - if kid refuses to pee, removing the foley commonly helps them to pee
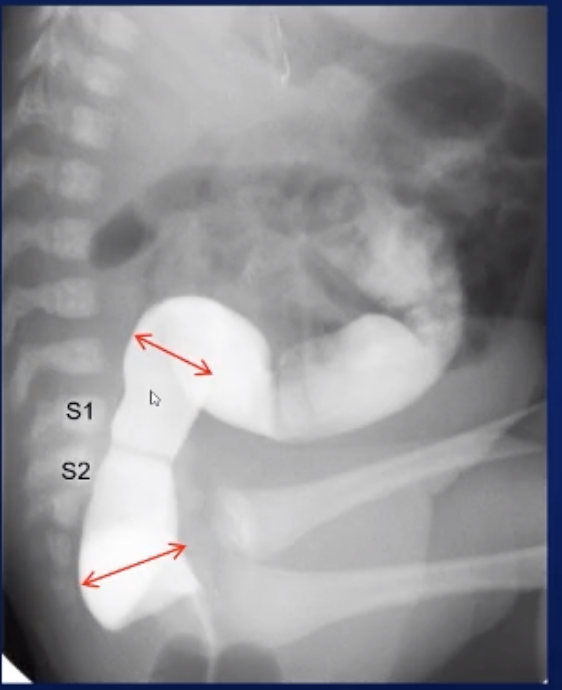
Contrast Enema
Pediatric
On lateral will see rectosigmoid junction at about S1-S2 and therefore would want to get a measurement on lateral view above and below this level to compare the recto-sigmoid ratio
All spot fluoro, not exposure, not sine
Start lateral and get rectosigmoid filling
Watch colon fill
Get RPO for splenic flexure (LUQ) and LPO for hepatic flexure (RUQ)
Need reflux into TI/small bowel
References:
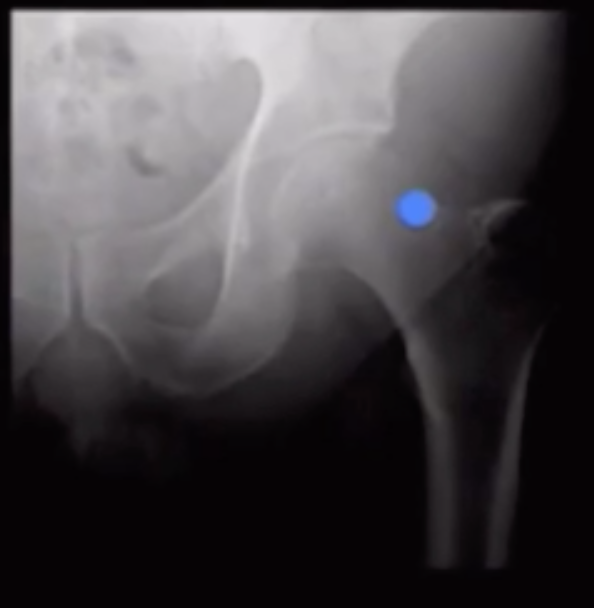
Arthrogram Hip
Cocktail ~15 cc
MRI
0.1 cc gadolinium
5 cc omnipaque
15 cc saline