Female Genitourinary
Ovarian Malignancy
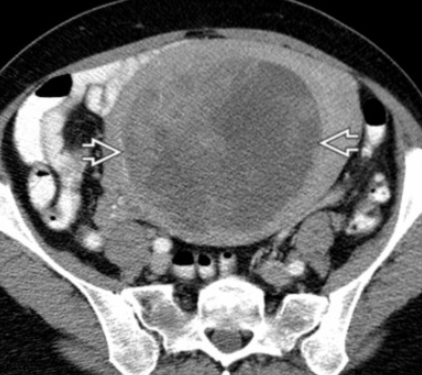
CT A&P is preferred first test for staging
MRI is degraded by bowel peristalsis motion and therefore is not preferred
PET for follow up but not for initial
General
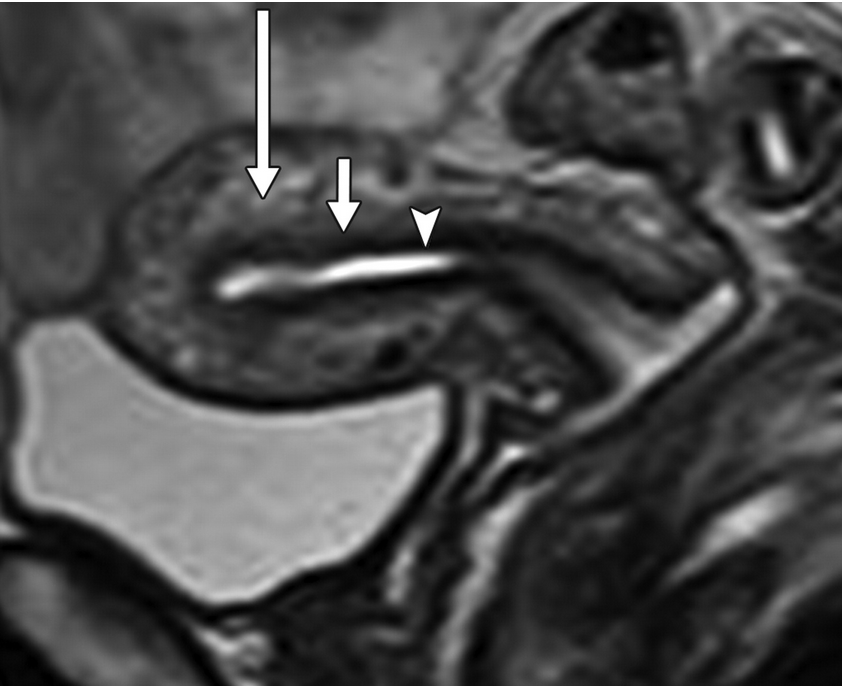
Junctional zone
Arrow head = endometrium
Middle arrow = junctional zone
Long arrow = Outer myometrium
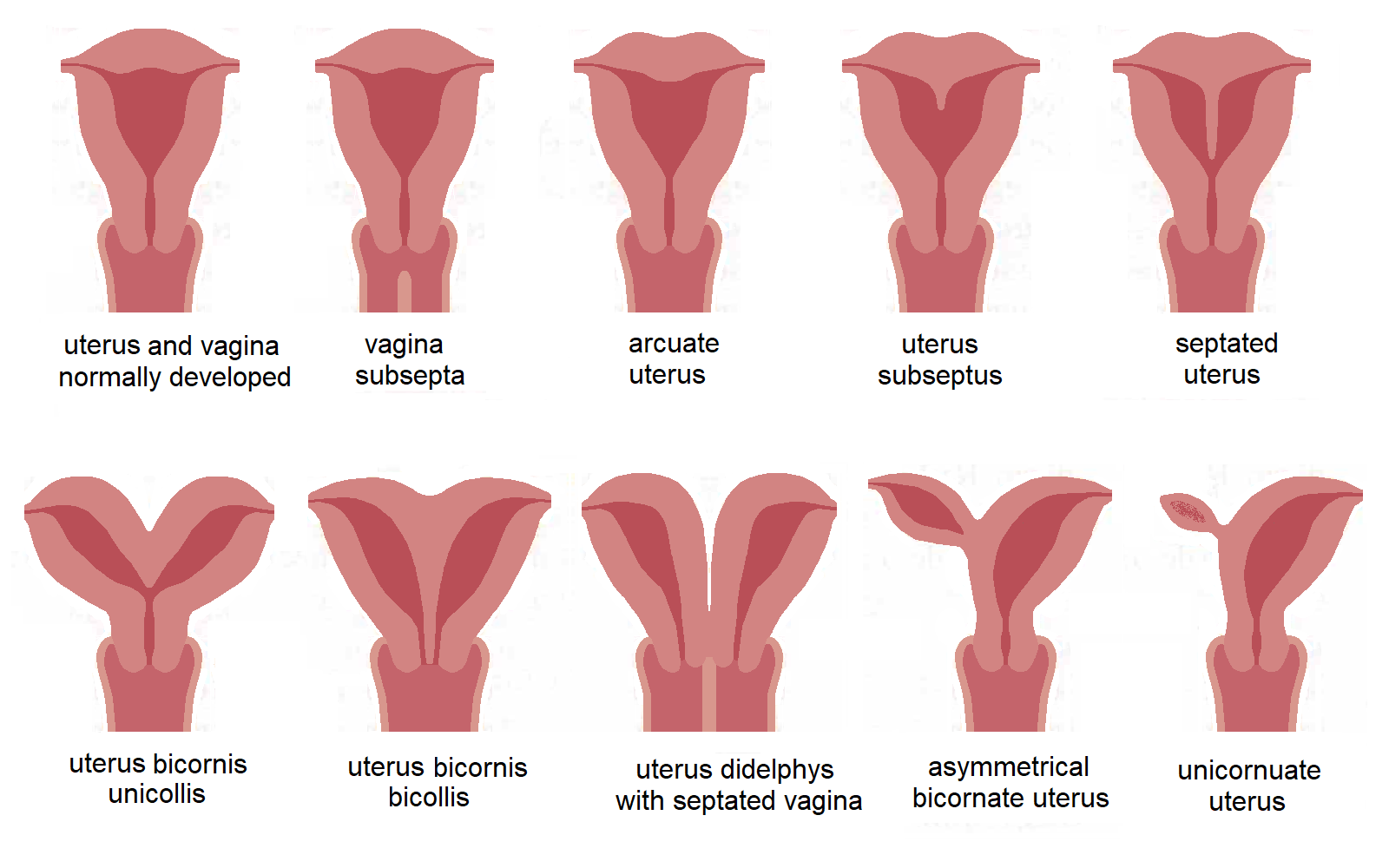
Mullerian Duct Anomalies
Can think of these as failure of the septum to resorb or failure of mullerian ducts to fuse
Agenesis
Always need to look at kidneys & GU system for additional abnormalities
Agenesis
Uterus doesn’t form basically because of interruption of mullerian duct early in development
Complete
No uterus, cervix or vagina
Partial
Has any part of the uterus, cervix or vagina present but everything
Ovaries are fine - can have a surrogate pregnancy
DES Exposure
Results in a T Shaped uterus
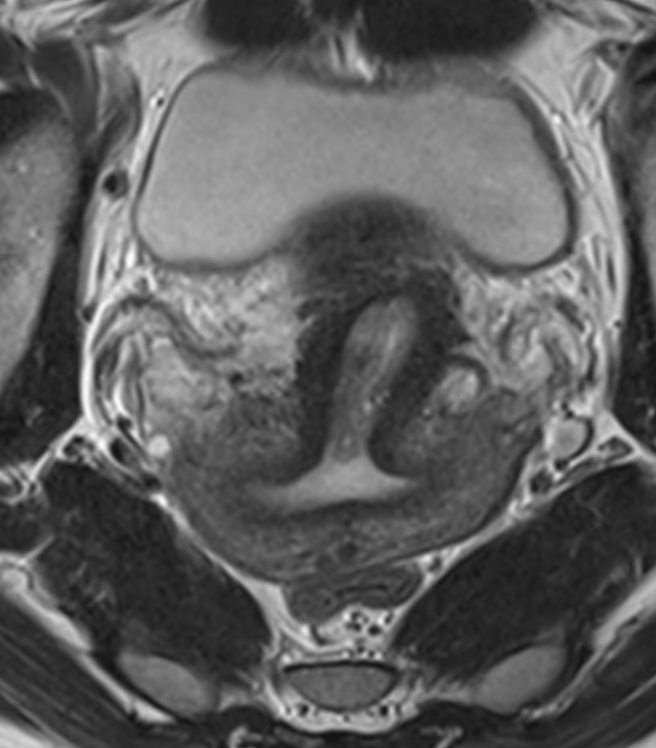
Septate Uterus
Failure of septum to resorb
No indentation at top of uterus (normal contour)
Look at T2 images to see if there is a fibrous or muscular septum - helps surgery
T2 dark = fibrous
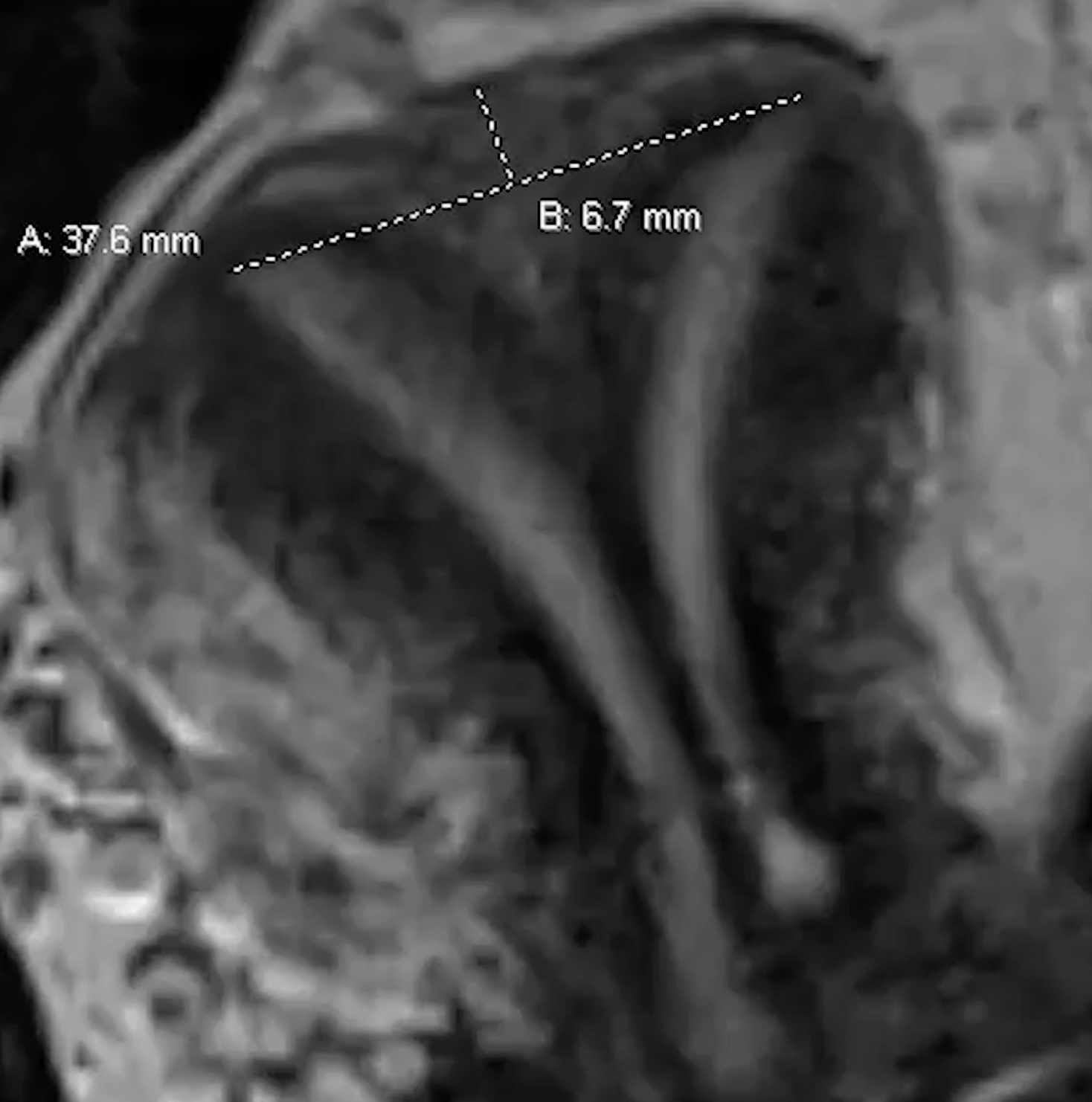
Should also measure the septum
Septate line
Drawn line across top of two tips (inter-cornuate line) and another from that line to the fundus
Needs to be > 5mm to be a septate uterus
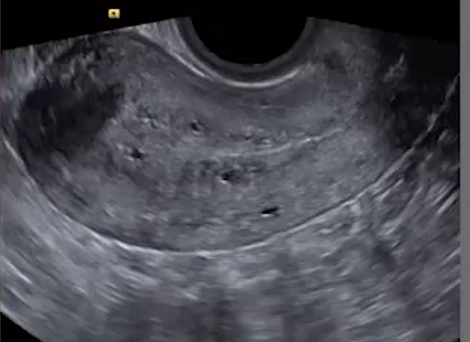
Adenomyosis
Ectopic endometrial glands in the myometrium
Technically myometrial glands 2.5 mm deep to the endometrial-myometrium interface
Findings
Ectopic endometrial glands
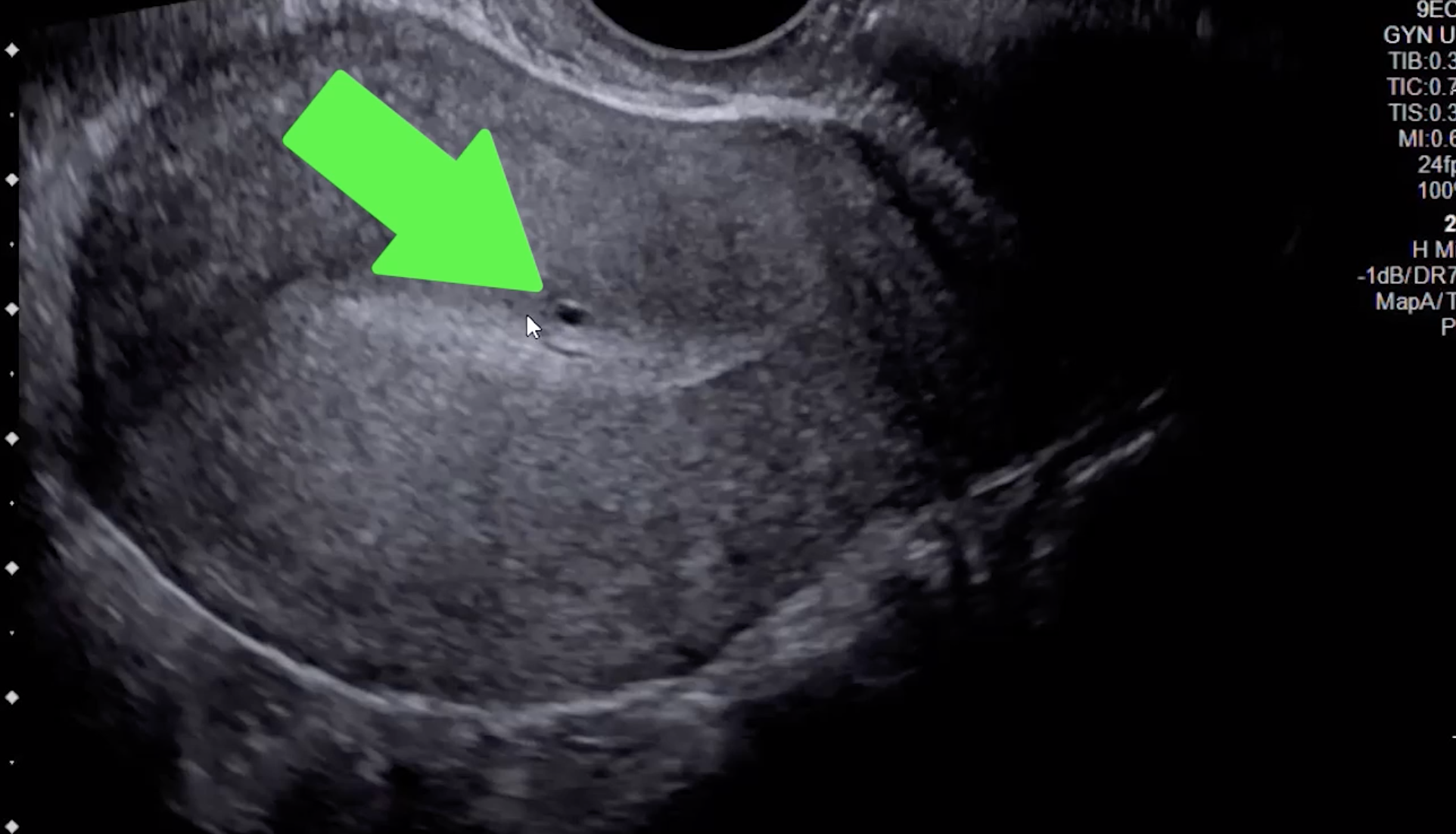
Echogenic nodules/striations or small cysts (US to R)
Small cysts at the endometrial-myometrial junction are most sensitive & specific finding for adenomyosis (green arrow)
Hypertrophy of myometrium
Junctional zone thickness >12 mm
Not required but high specificity
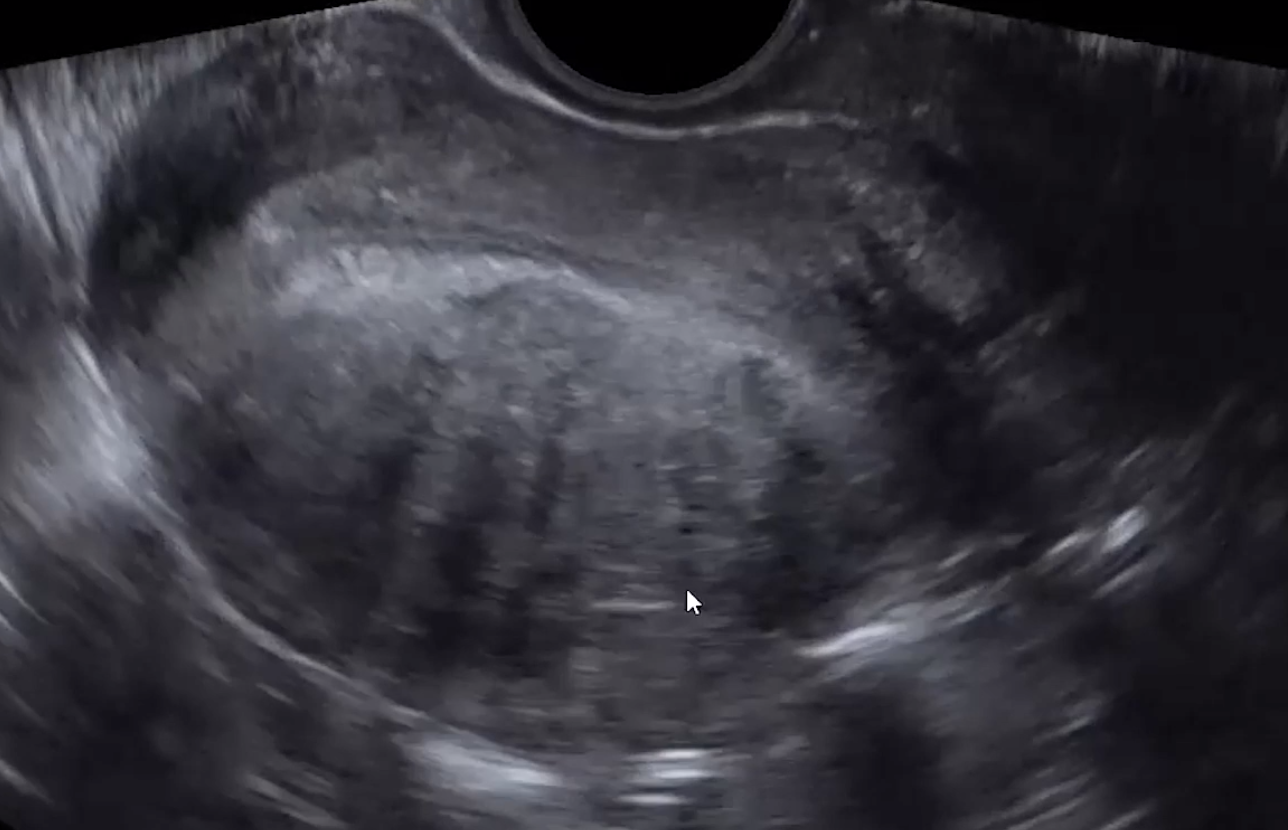
Venetian blinds appearance
Alternating stripes of increased and decreased echogenicity - looks like light coming through the blinds to me (bottom image)
Need to make sure the lines don’t go back to the arcuate arteries within the uterus itself, that’s just artifact
Ill defined endometrial-myometrial junction
Vascularity
Tortuous and increased vascularity
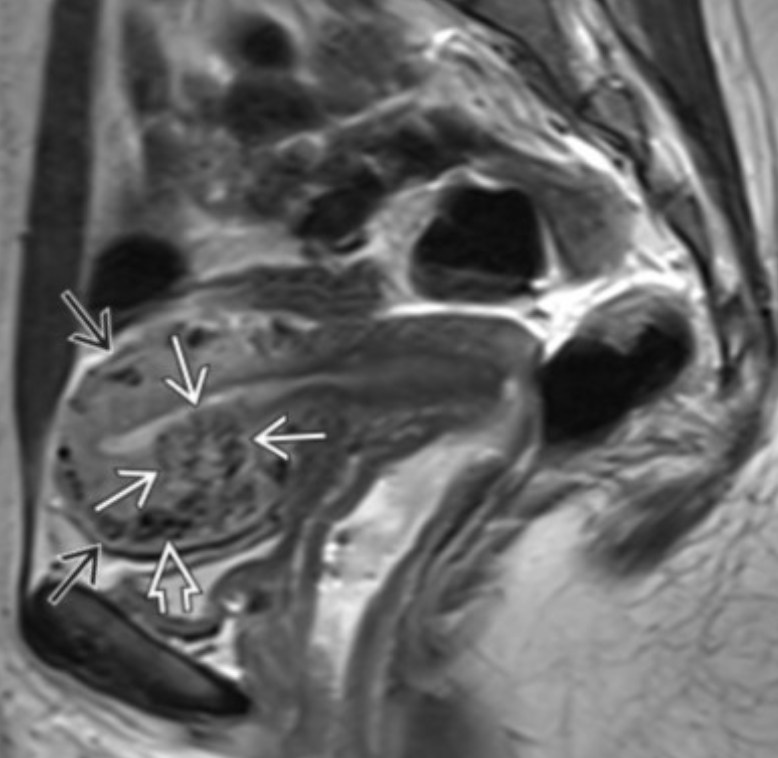
Specific to MR
Thick junctional zone with indistinct margins
T2 bright foci in endometrial & myometrium (sometimes T1 bright too)
This is how you differentiate it from a fibroid
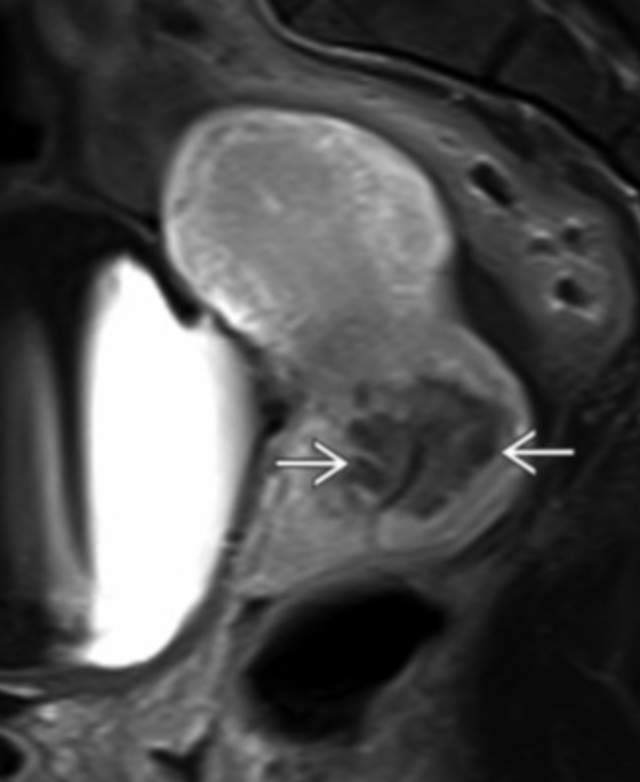
Adenomyoma
Basically adenomyosis in mass form
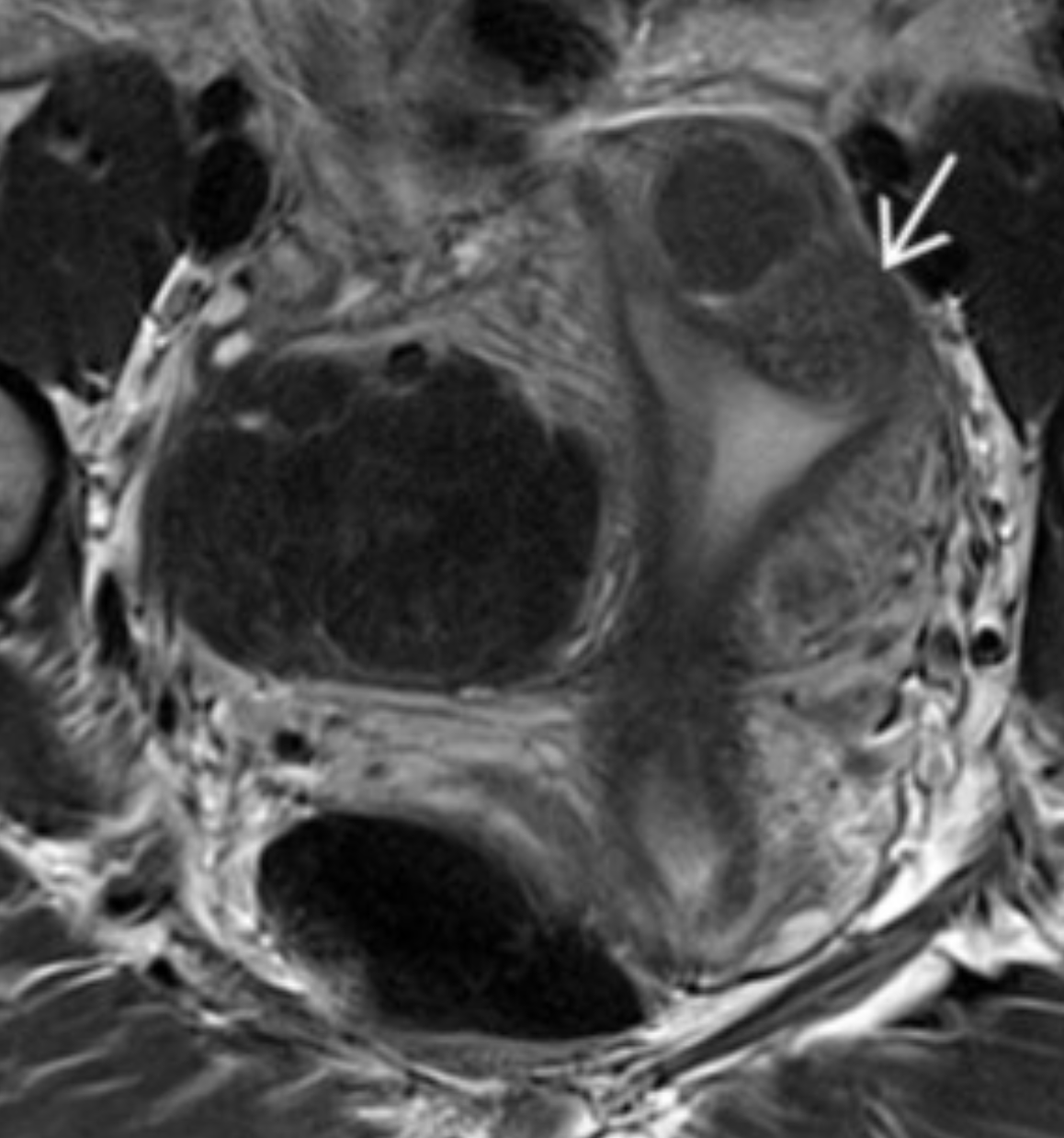
Leiomyosarcoma
Look for an enlarging uterine mass/uterus with internal areas of hemorrhage/necrosis
May look largely cystic with blood and shit in there
Look for mets
If none seen, should include degenerative/degenerating fibroid in ddx
Uterine AV malformation
Basically AV fistula in uterus
Risk factors
Trauma (curettage included)
Intrauterine contraception use
Treatment of prior trophoblastic disease
Pelvic Actinomycosis
Life threatening infection
Associated with IUD use (also surgery, trauma)
Falls under the umbrella of PID
Looks like really bad loculated abscess
Multiseptated fluid containing mass with enhancing walls and septa
OHVIRA Syndrome
Obstructed Hemivagina
Ipsilateral renal anomaly
So
Duplicated vagina, cervix, uterus
Renal anomly
Hematocolpos
Uterus
Rudimentary horn
Basically a little uterus next to the main uterus
May communicate with regular uterus or not
Caused by incomplete development of one of the mullerian ducts (the rudimentary horn) while the other duct forms normally (regular uterus)
Main uterus may be smaller than usual
Increased risk of preterm labor
Increased risk of IUGR (smaller uterus so smaller area for baby to grow)
Need to evaluate if the rudimentary horn has its own endometrial lining
Increased risk of ectopic if endometrium is present
Need to cut it out
Increased risk of
Uterine rupture
Miscarriage
GU anomaly will typically be on same side as the rudimentary horn
Fibroids
Endometriosis
Increased risk for
Endometriod cancers
Clear cell carcinoma
Hematosalpinx
If you see this need to look closely for small endometrial deposits outside the uterus because it is almost pathognomonic for endometriosis
Torus Uterinus
Sampson syndrome
Cullen syndrome
Kissing ovary sign
Unexpected ureter kinking or hydronephrosis
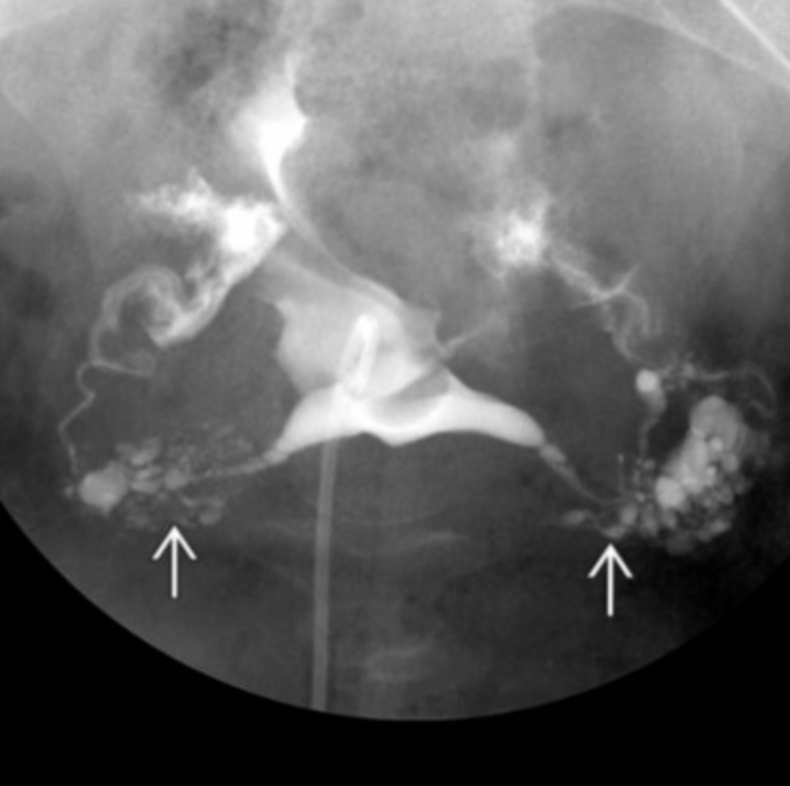
Salpingitis isthmica nodosa
Basically nodularity/diverticula of the fallopian tubes
Risk for ectopic pregnancy
Cervical glandular hyperplasia
Located along the inner aspect of the tissue (surrounding the canal)
Should not extend to the superficial surface
Well Defined
Random Uterine Pathology
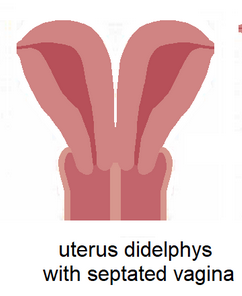
Uterine Didelphys
Bother mullerian ducts form but they don’t fuse together
Two horns, two cervix
Look for a hemi-vagina if you see didelphys
High vaginal septum (70% of cases)
wall of tissue blocking flow which results in back up of period blood
Pain
Patient comes to ED
Uterine Fibroids
Exist on a spectrum of benign to non-benign (but not necessarily malignant)
Benign
Non-Degenerated
Degenerated
Degeneration types
Mxyoid
Cystic
Hemorrhagic
Fatty
Hyaline
Non-Benign
Mitotically active, increased cellularity, Atypical appearance
STUMP (small muscle tumor of
Malignant sarcoma
Imaging Findings
US
Well circumscribed
Hypoechoic
Calcs which may have shadowing
May have increased vascularity
Really just looks like a heterogenous crock of shit
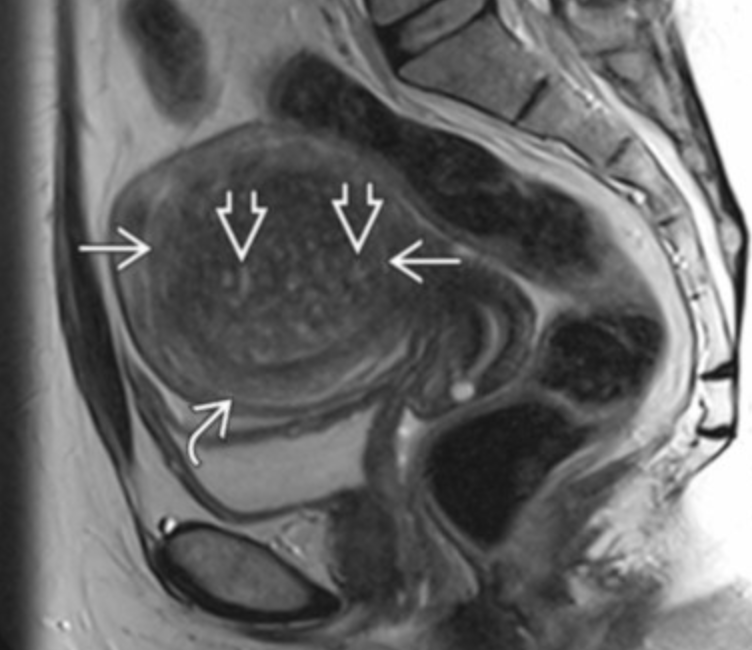
MRI
Classically T1 isointense to myometrium, T2 hypointense
T2 hypo-intensity should make you think of fibrous tissue, the most common of which is a fibroid
Areas of internal T1 hyperintensity —> consider hemorrhagic component/degen
The internal T1 hyperintensity looks slightly T1 hypointense tbh, not actually very T1 dark but bright relative to myometrium I suppose
Enhance
Some variation though
May have increased calcifications after necrosis or with increased (post-menopausal) age
Location
Submucosal
Intramural
Subserosal
Pedunculated (can torse and cause acute pain)
Others
Red fibroid
Basically acutely infarcted and hemorrhagic fibroid
T1 hyperintense (again not dramatic but kinda brighter than the myometrium)
Look at subtracted images because if already T1 bright internally then will be bright on post-contrast too because its already bright on the T1, so look at subtracted images and if looks like black hole (all dark inside) then likely red fibroid
Lipomyomyoma
Basically a fat fibroid
Bright mass on US
Look for no shadowing, if bright mass and shadows can be air or calcified fibroid
If fallopian tube fibroid
Should be in between the uterus and ovary
Need to look for a normal ipsilateral ovary otherwise a fibrous tumor of the ovary (fibroma) is in the ddx
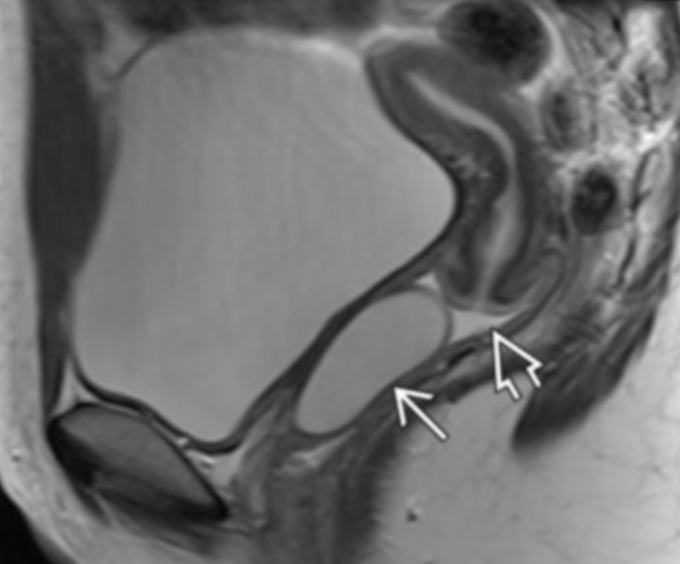
Nabothian Cyst

Cysts
Garter Duct Cyst
Upper vaginal cyst, usually anterior wall
Cervix

Adenoma Malignum
Solid and cystic mass
References: