Breast MRI
Indications for Breast MRI
Implant evaluation
Axillary mets of unknown primary
Evaluate extent of disease (particularly of invasive lobular carcinoma)
Evaluate response to therapy
High risk screening
Lifetime risk >20% (15-25%)
20 Gy of radiation to the chest as a child (lymphoma, etc.)
Diagnostic dilemma
Protocol
Basically everything is fat suppressed because breast is fatty so you need to get normal tissue suppressed
T2 with FS —> good to see the benign shit typically, cysts and whatever
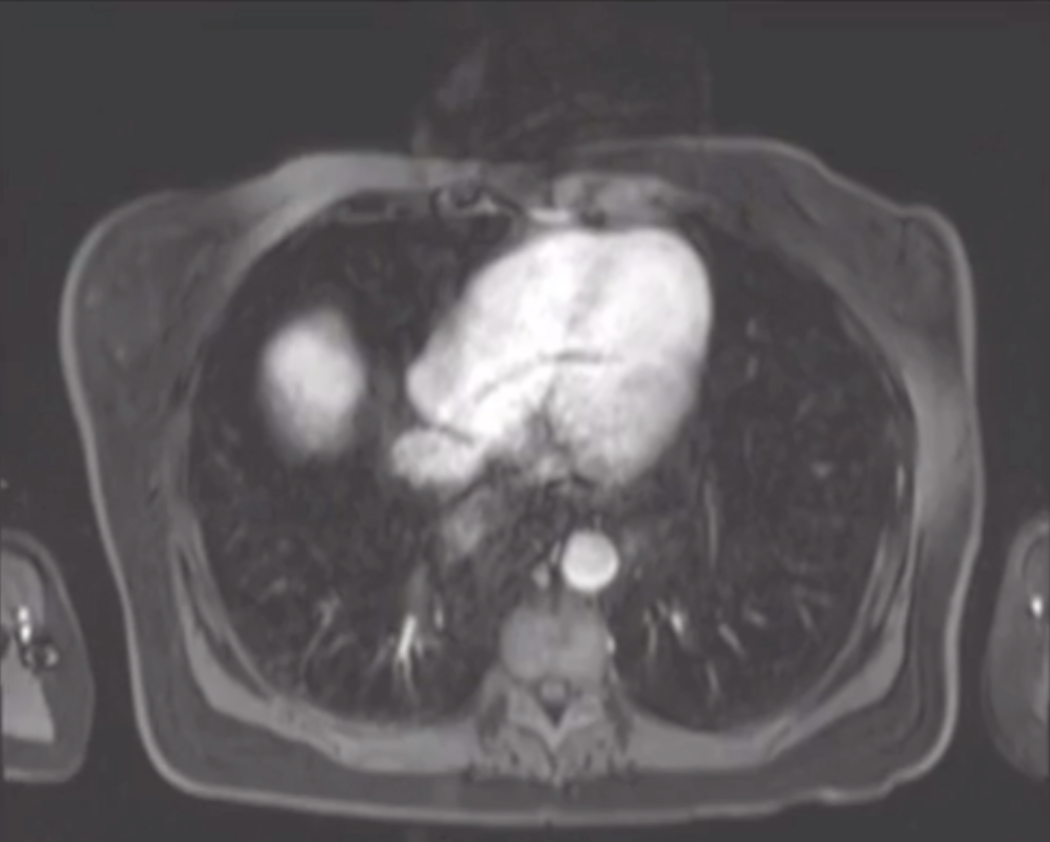
To identify sequence — no heart visualized = T2
Need a breast coil
Need to be positioned correctly
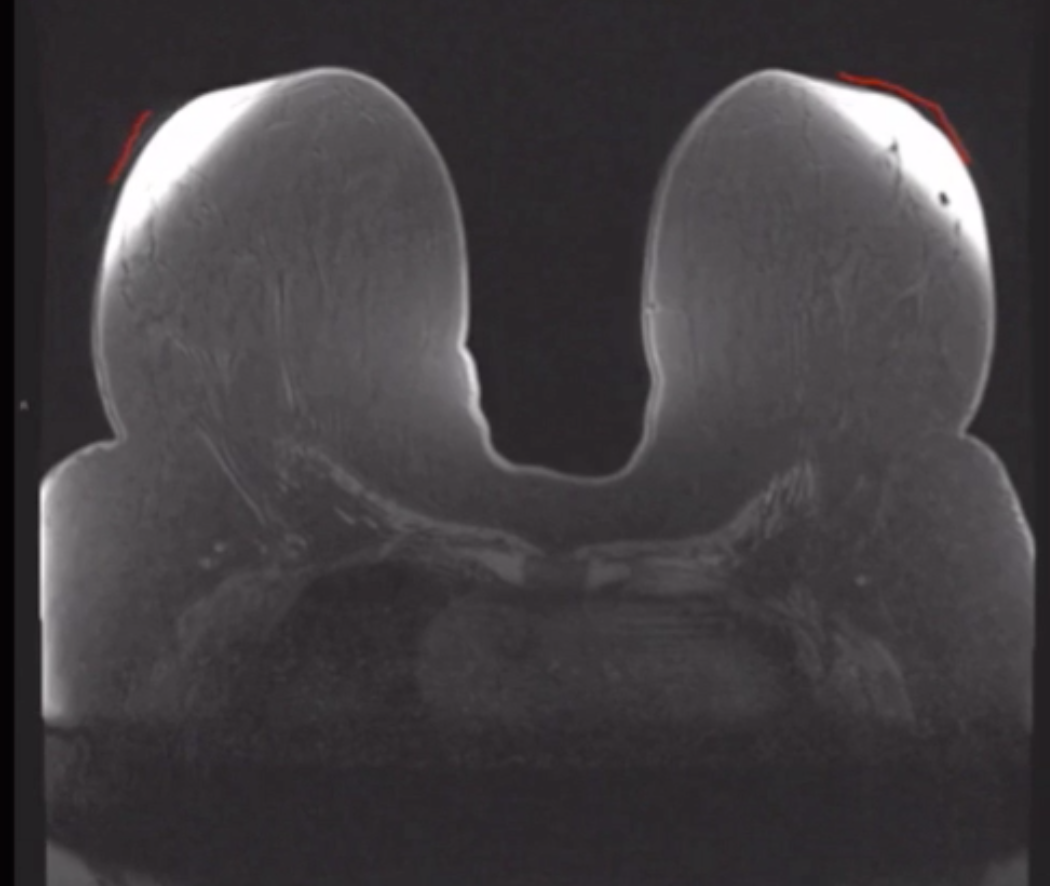
Fat saturation
Poor fat saturation in image below
Remember, cannot use an inversion sequence if you are giving gadolinium because it has similar inversion time as fat (STIR) it would null out the gadolidium
Need a homogenous field to tell difference in resonance between fat and water
Water typically has taller peak
Fat has lower peak
Can null the fat peak or
Can use shimming
Also, get rid of field inhomogeneities (flatten fat fold with air pocket for example)
Incomplete fat saturation
Background Parenchymal Enhancement
Varies based on many factors, including
Menstrual cycle
Contrast agent used
Optimal time to scan = between day 5-15 of menstrual cycle
More enhancement seen in later part of cycle
Need to scan on same time of cycle if a second exam
Need to be off hormonal replacement therapy for 2-3 months
Need to be at least 6 months after lumpectomy
Need to be at least 1 year after radiation therapy
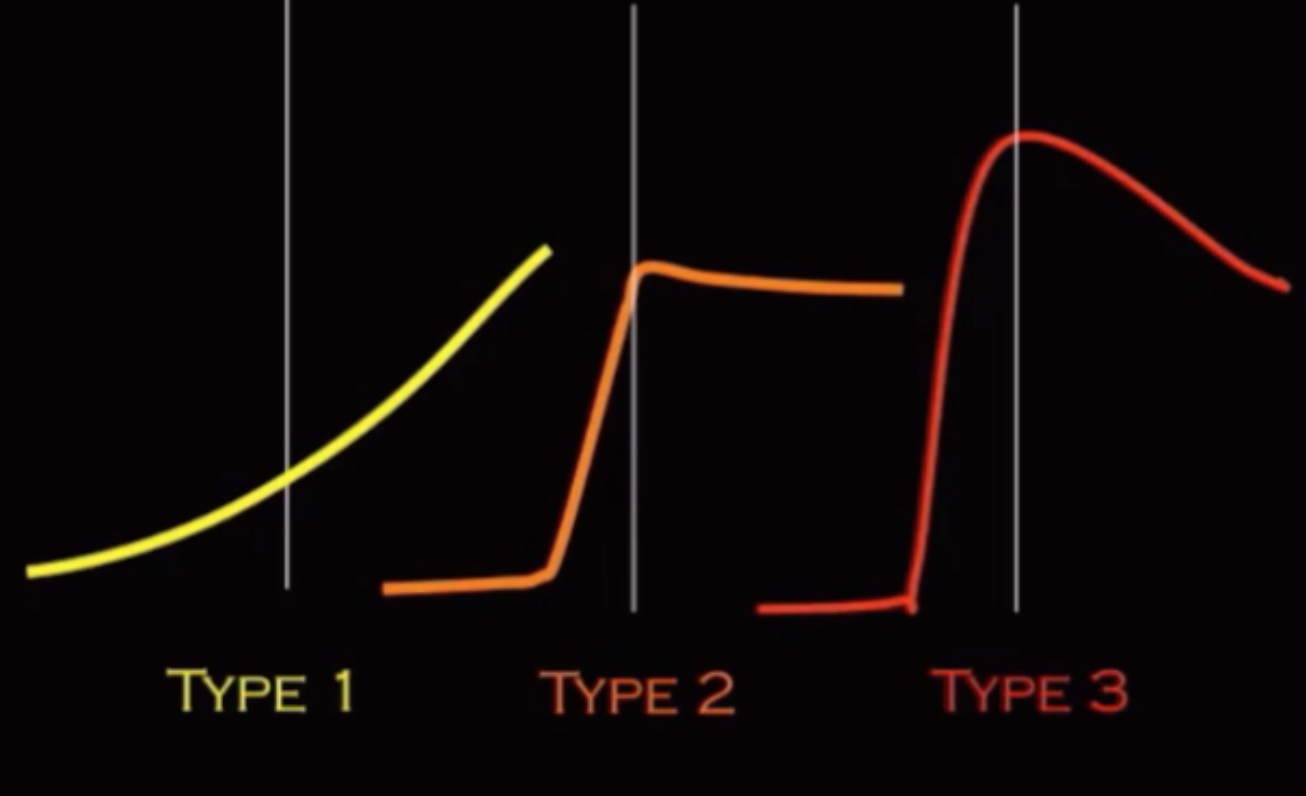
Type 1 = good
Type 3 = bad
Kinetics not really helpful for DCIS
Breast Pathology Pearls
Nipple normally enhances but will enhance more in Pagets
Enhancement alone does not necessarily indicate malignancy
LN, fibroadenomas, papillomas can all enhance
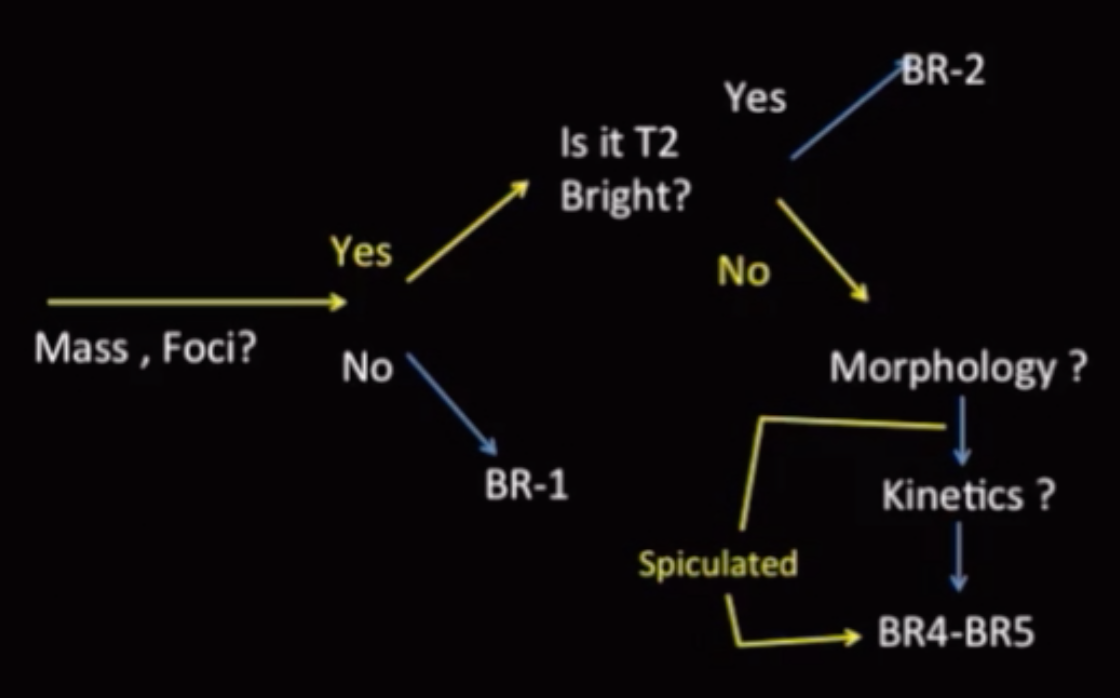
If lesions is T2 bright = likely benign
Exception = mucinous (colloid) cancer = bright on T2 and malignant
Mass margin is the feature most indicative of malignancy (more so than enhancement, bright/dark shit)
Margin of the mass should be evaluated on the first post contrast series
Spiculated = highest PPV of malignancy
Rim enhancement = bad
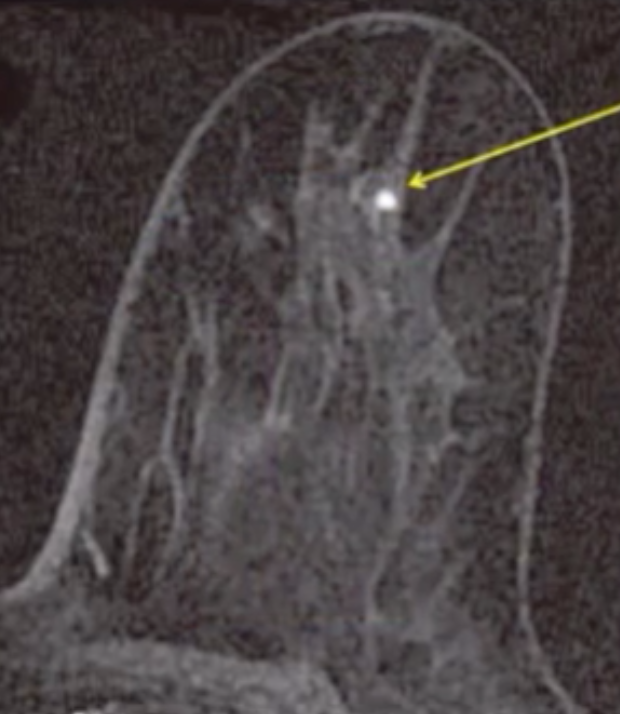
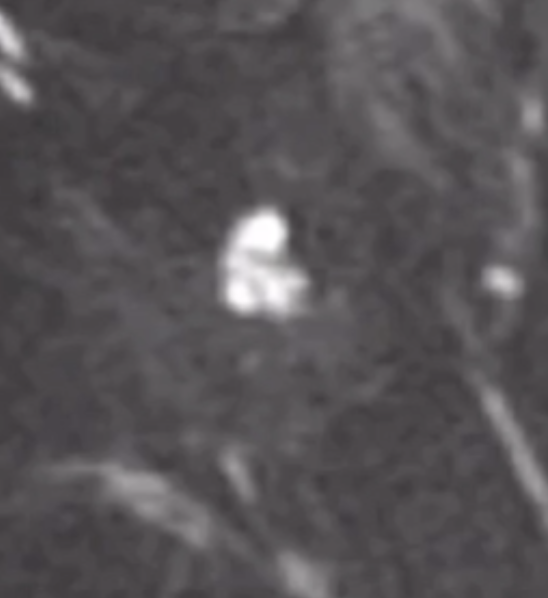
Foci
Dot of enhancement <5 mm
Too small to otherwise characterize
Multiple enhancing foci is lumped in with the background enhancement, not a BR2 just background breast tissue basically
References:
Flaring
Non uniform fat suppression when breast tissue to too close to the coil
NOT related to fat suppression process itself
Fix by putting a pad between the breast tissue and coild
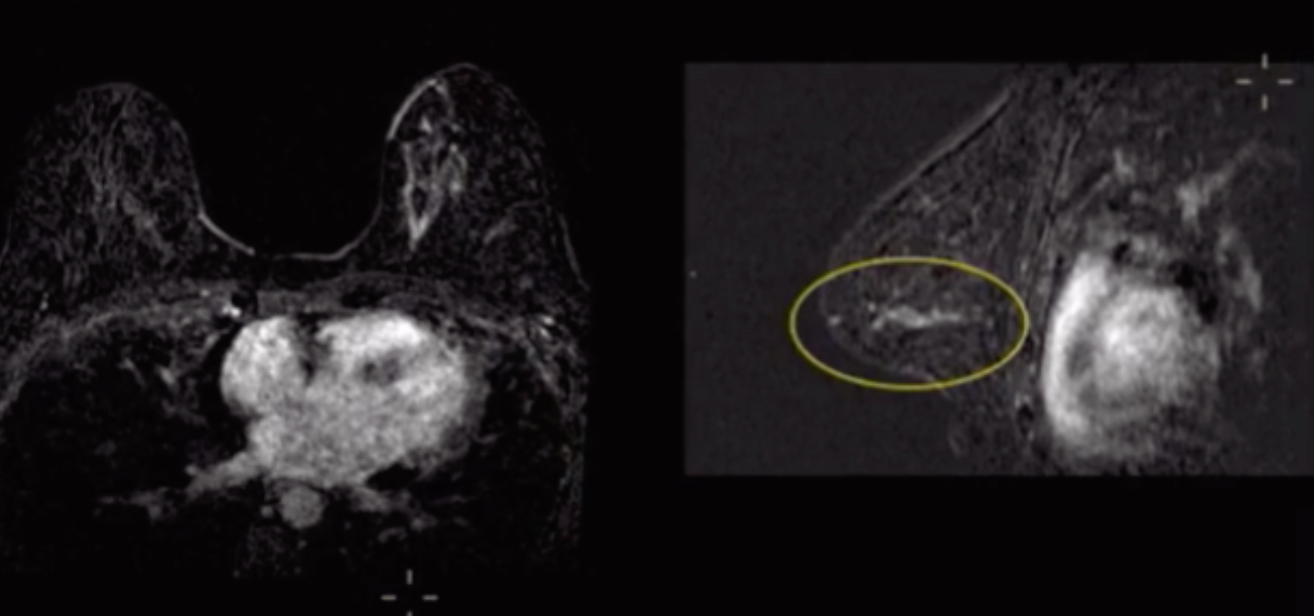
Kinetics
Pathology
Pulsation artifact
Occurs in phase encoding direction
Takes longer so done in shorter axis
In chest MR = AP
In breast MR = side to side
Even though sided to side is wider and therefore will take longer you cannot have artifact in front of the chest in the breast tissue
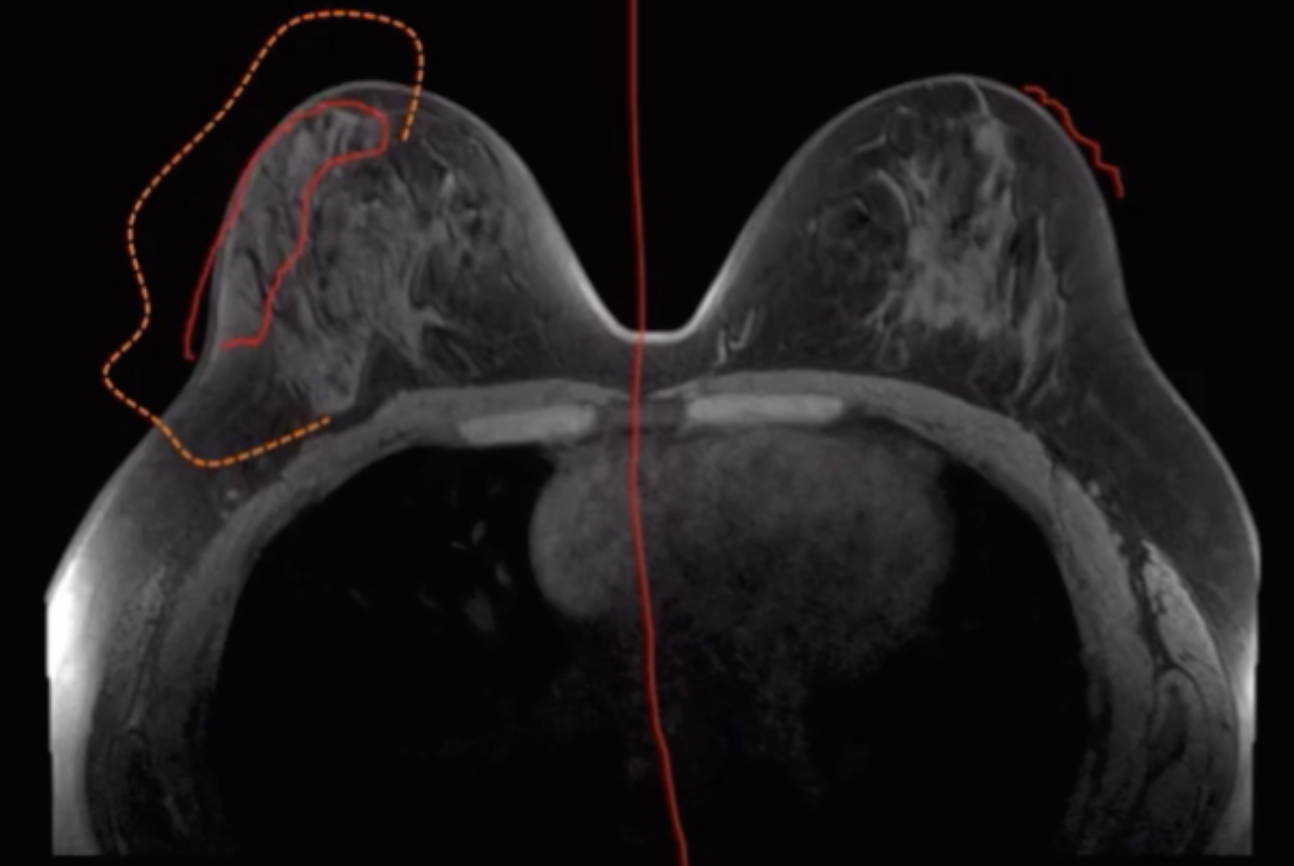
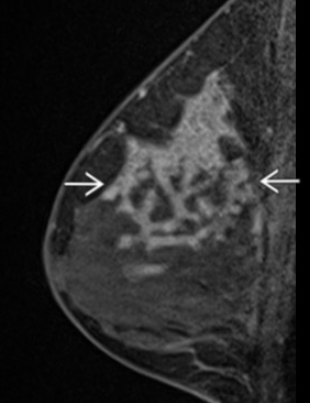
Non-mass enhancement
Weird clump like area of enhancement
Classified according to distribution
Distribution of NME is the most predictive feature
Segmental distribution has the highest PPV
More concerning patterns
Focal
Linear
Segmental
Somewhat triangular area extending toward the nipple
Less concerning patterns
Regional
Multiple regions
Diffuse
If you see NME, think DCIS
Fibroadenoma
Well circumscribed mass
T2 bight (varies)
T1 post = homogenous enhancement with non-enhancing septations
Segmental Non-mass enhancement
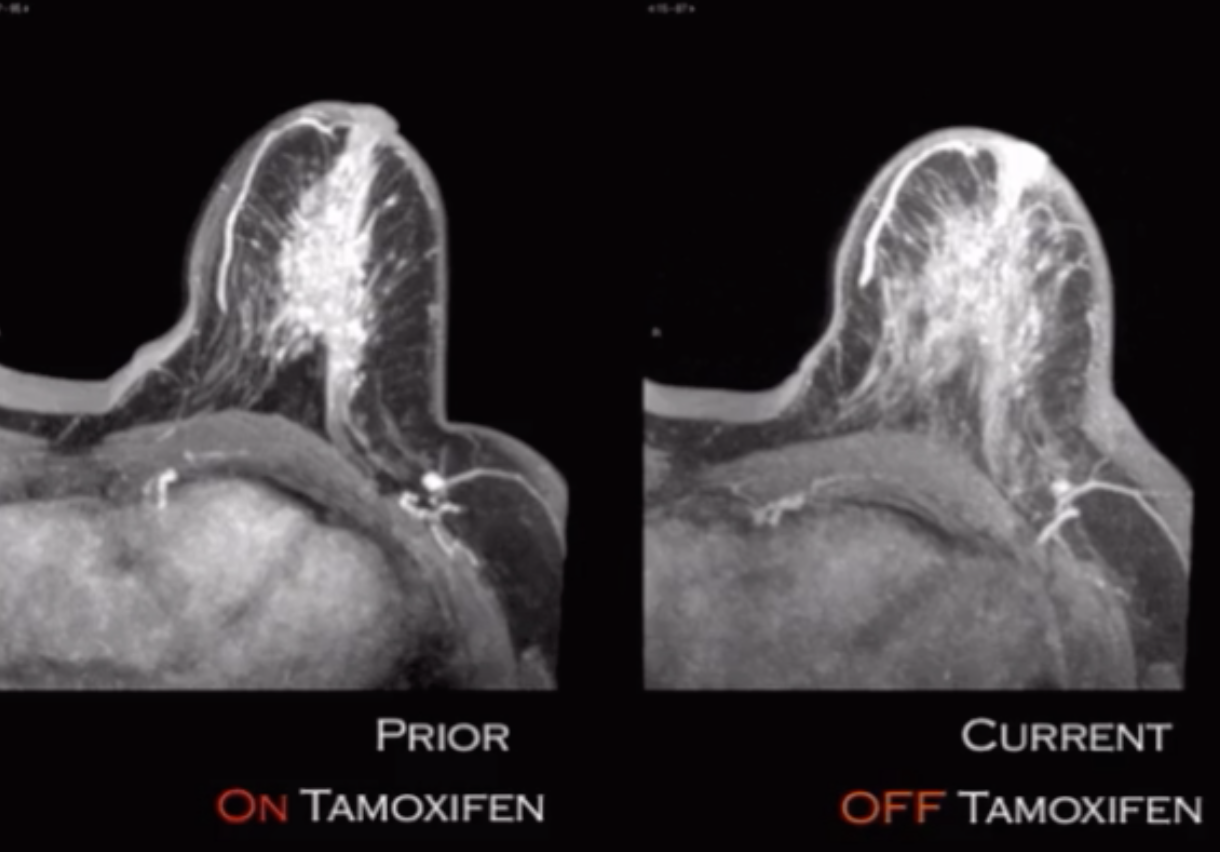
Rebound/Flare Affect
When on tamoxifen breast tissue is suppressed
When off tamoxifen breast tissue will go back to normal and get bigger