Benign Breast Findings
General
Benign things requiring no follow up
Fibroadenoma
Lipoma
Hamartoma
PASH
Intramammary lymph node
Fat necrosis
Fibcrocystic changes/cysts
Benign findings that still warrant surgical evaluation
Phyllodes tumor
Granular cellt umor
Desmoid Tumor
Granulomatois mastitis
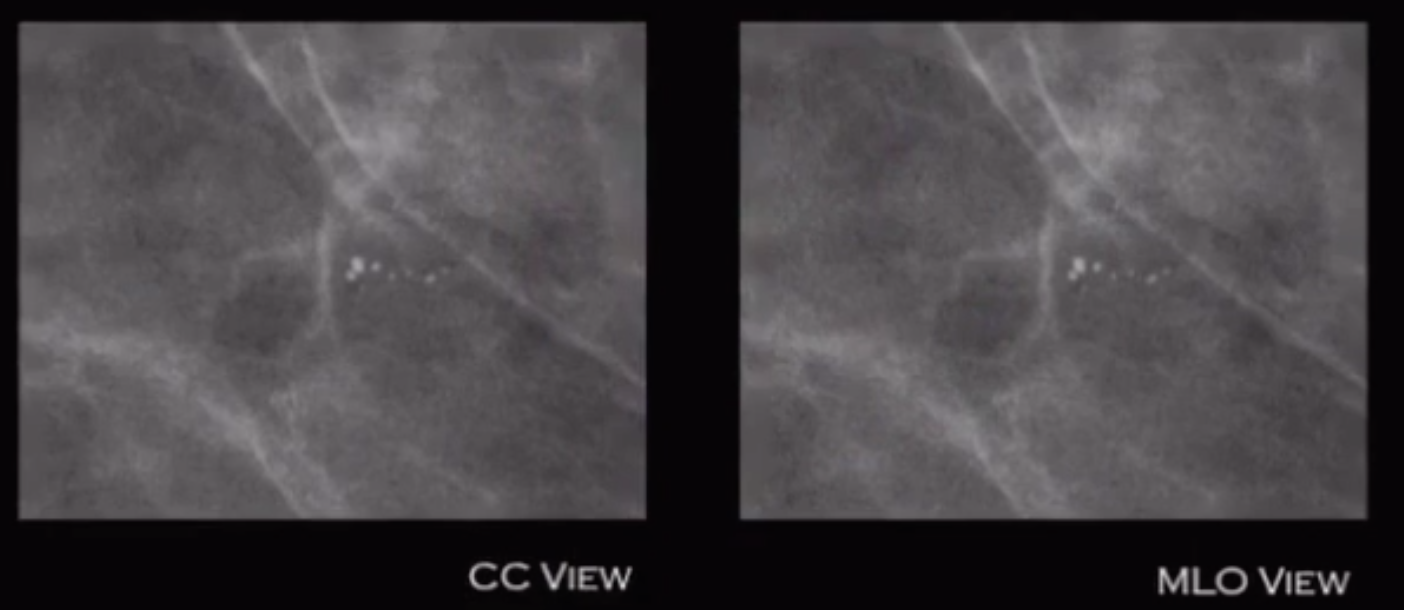
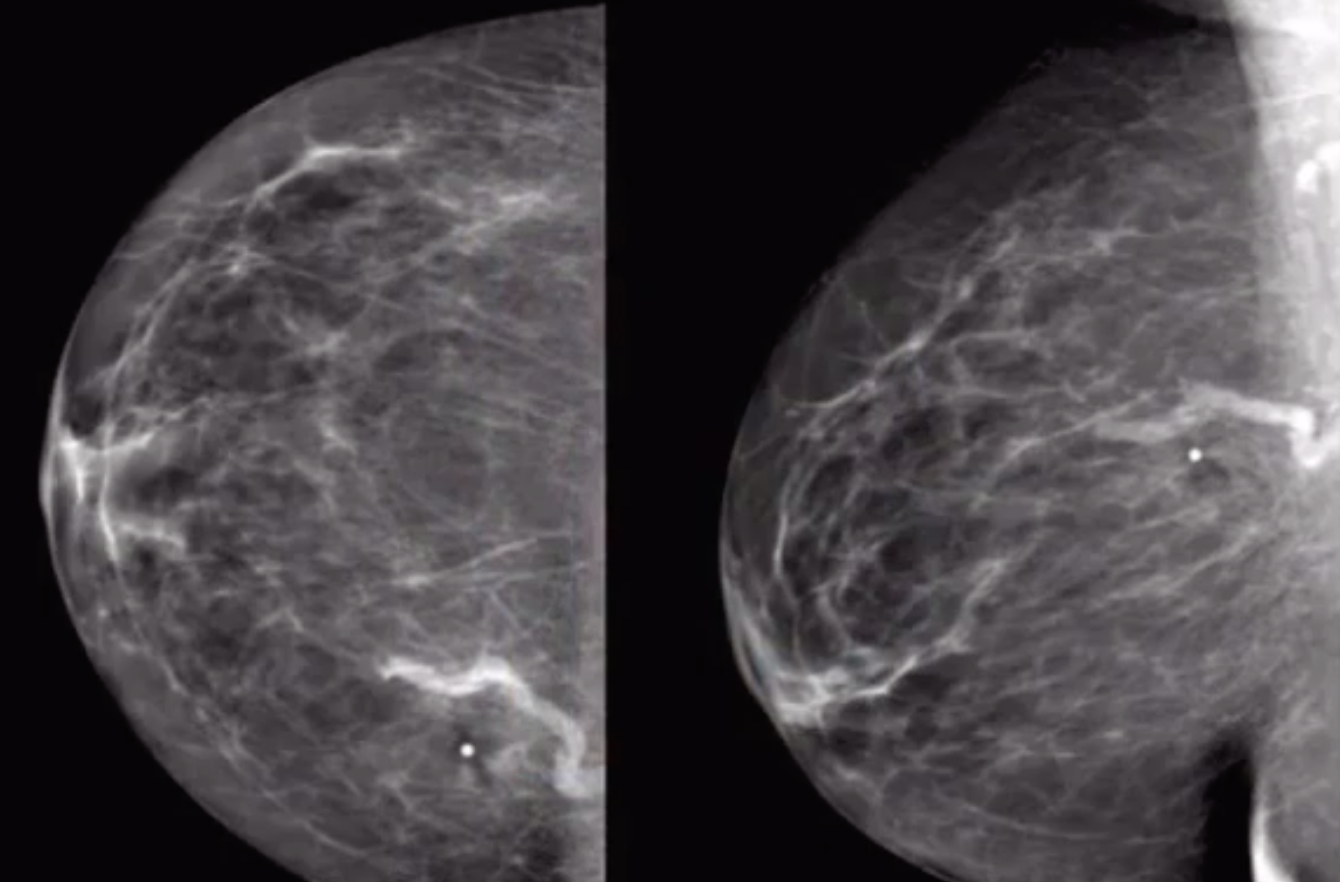
Dermal Calcifications
Clustered calcs that are about same size and shape and do not change on CC & MLO views
Tend to be near folds (i.e. axilla)
Can get a tangential view to prove they are dermal calcs
Granular Cell Tumor
Rare benign mass arising from Schwann cells
Typically arise medially from the supraclavicular nerve
Looks like a mass, therefore needs biopsy
Rarely malignant
Treated with wide local excision
Fibrocystic Changes
Basically catch all term for crunchy breasts, including
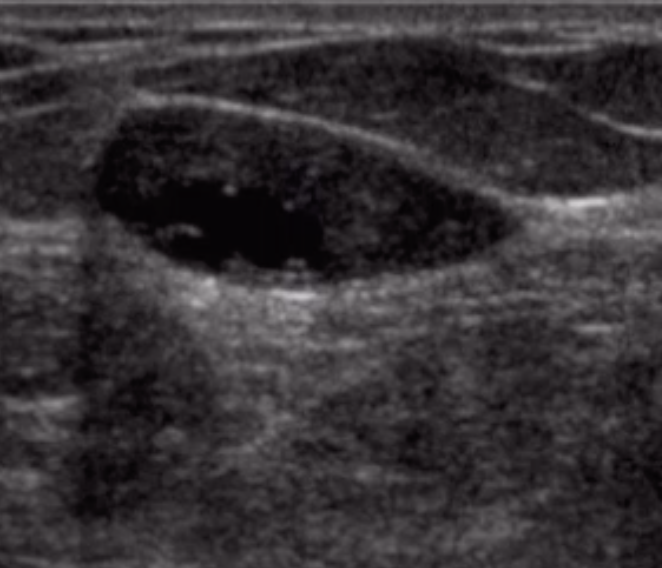
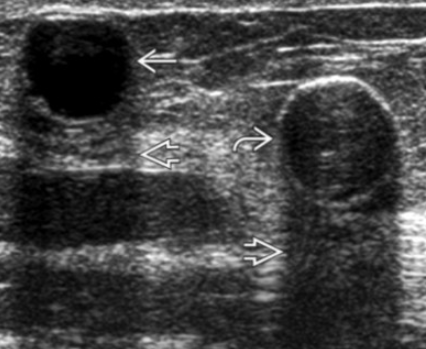
Cysts
Microscopic cysts may have milk of calcium
Apocrine metaplasia
Transformation of normal breast cells to apocrine sweat glands - benign, normal process
Fibrosis
Sometimes calcifications
No follow up needed
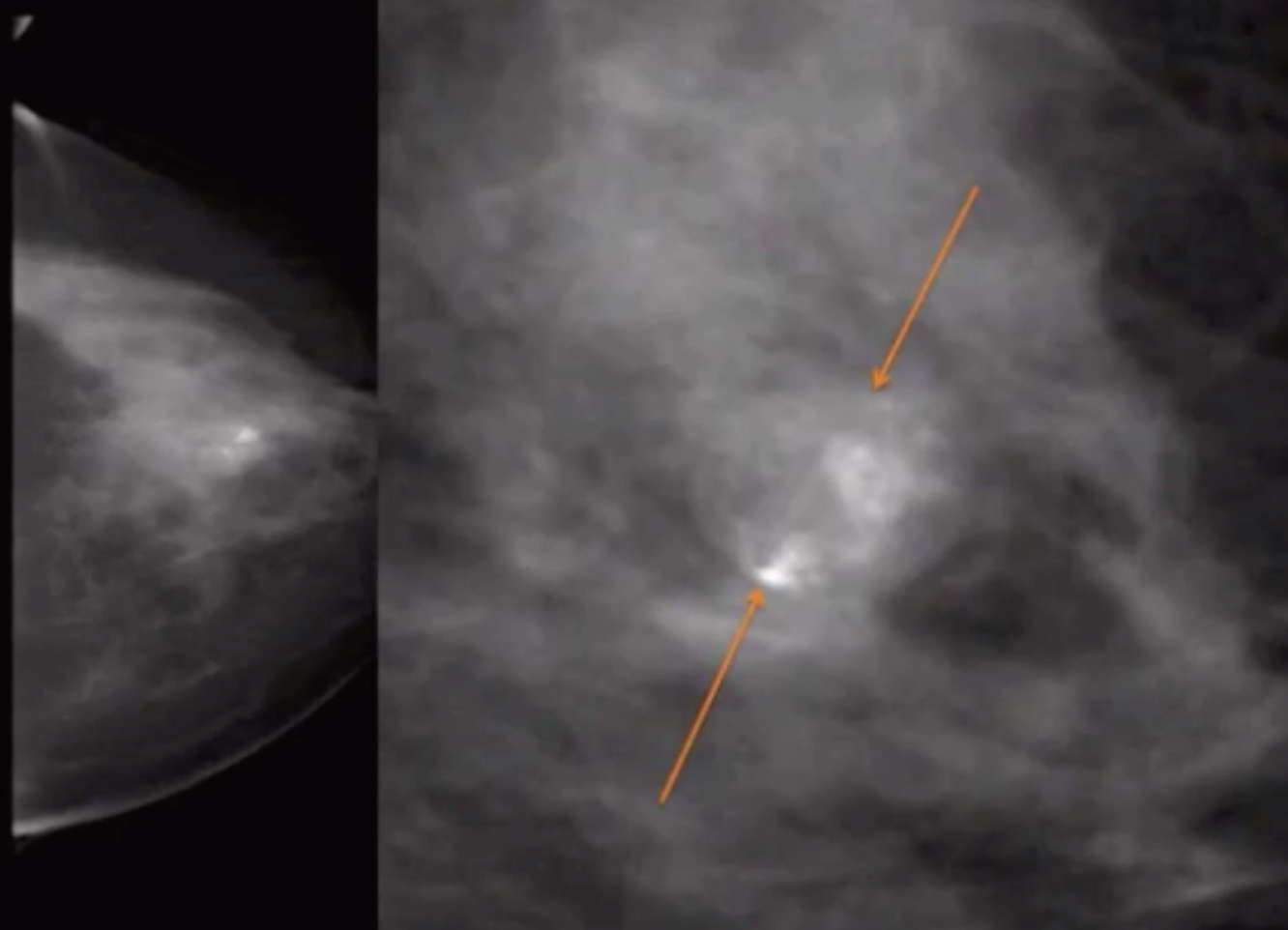
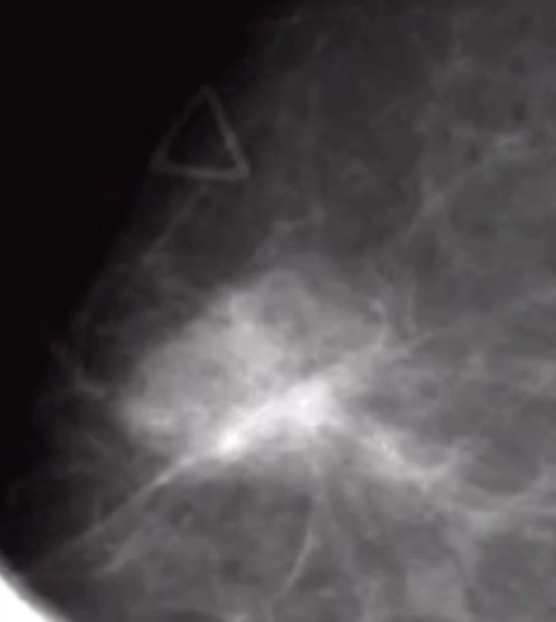
Granulomatous Mastitis
Idiopathic inflammation of breast
Pre-menopausal women
Classically occurs within a few months of a recent/last regnancy
Seen usually as subtle focal asymmetry with indistinct margins
Present with
Galactorrhea
Pain
Skin chnages
Possible palpable mass
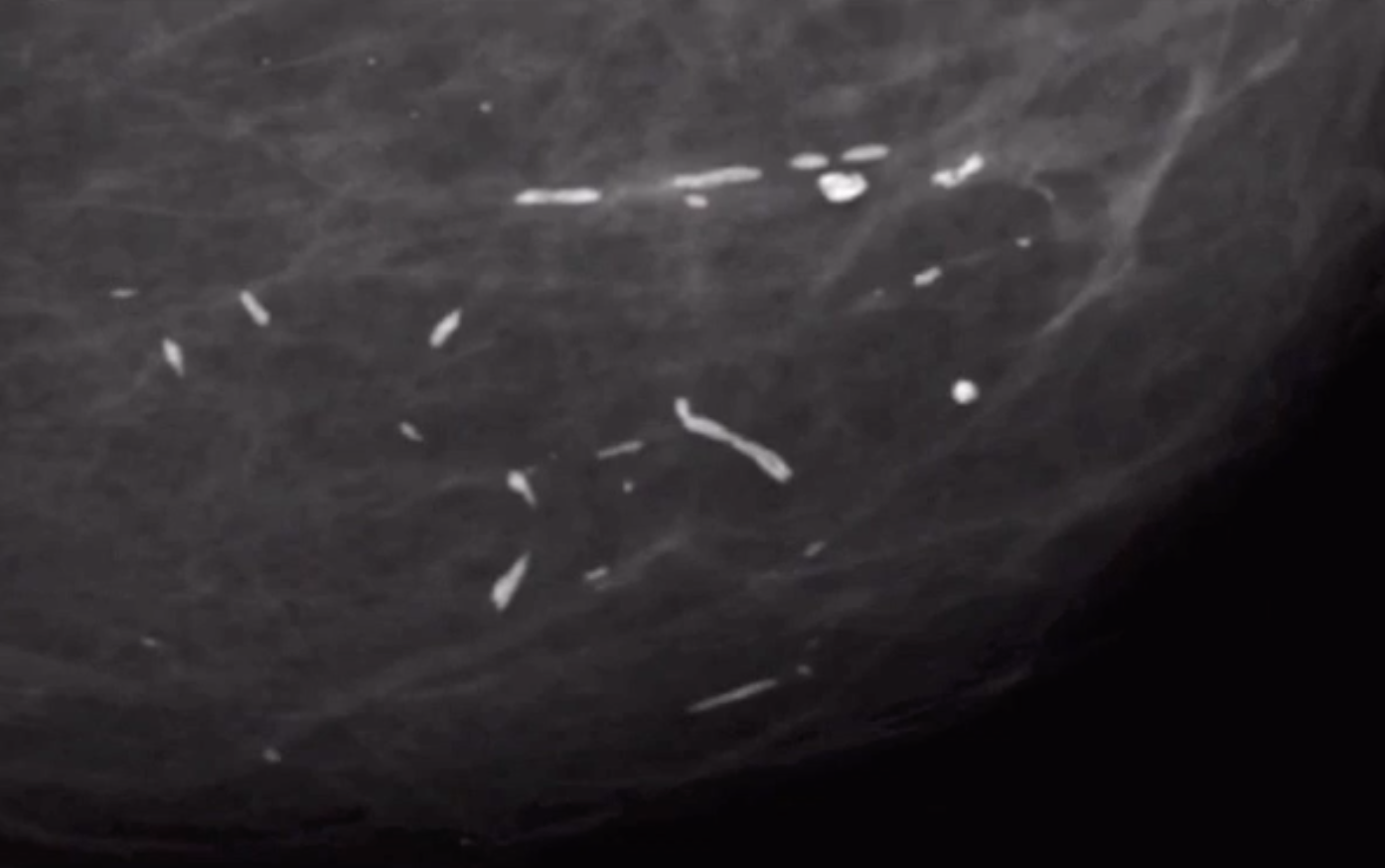
Secretory Calcifications
Rod like/cigar shaped calcifications with a dash-dash pattern
Calcs point toward nipple
Typically bilateral
Seen in older women 10-20 years after menopause because it is from duct involution
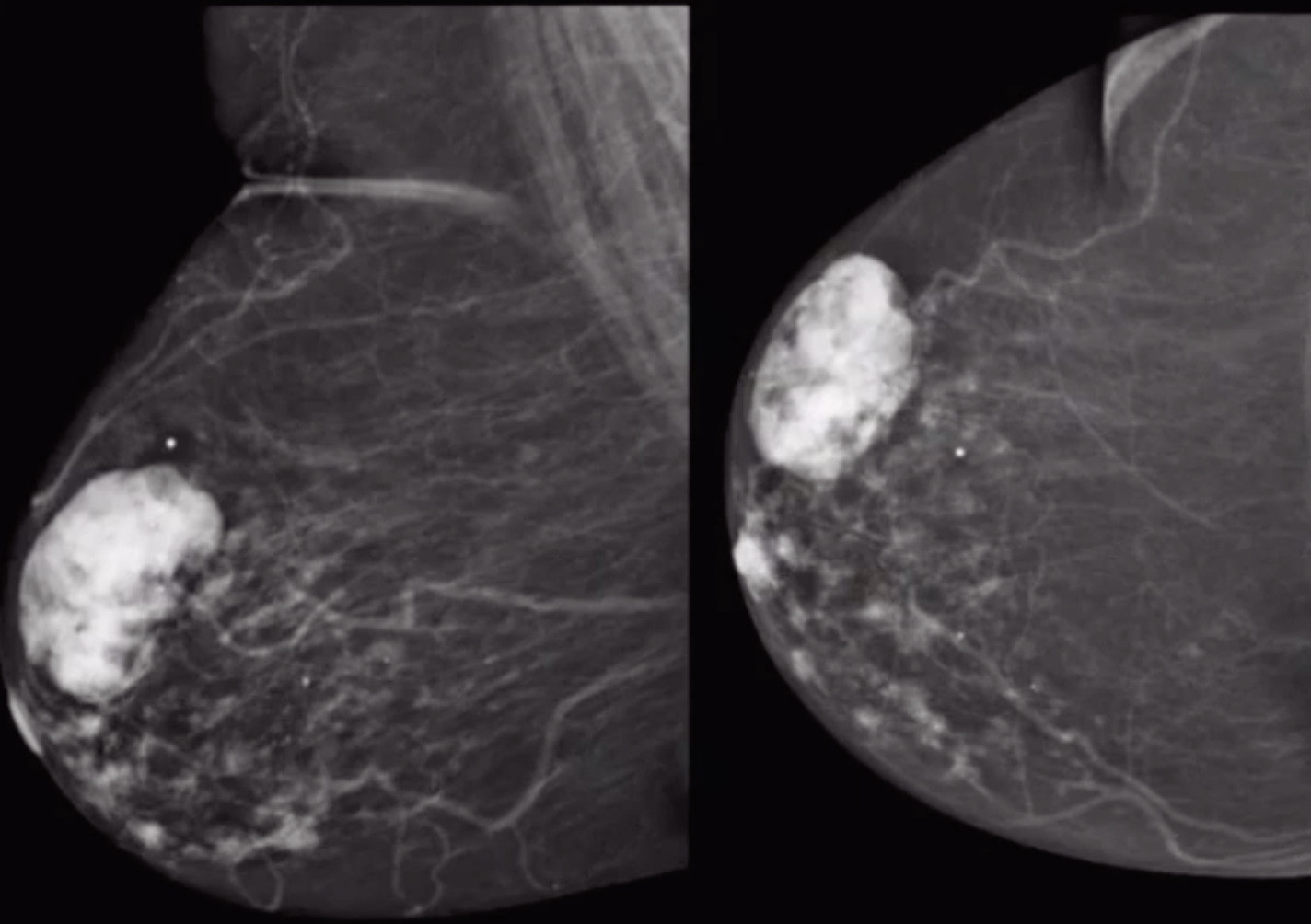
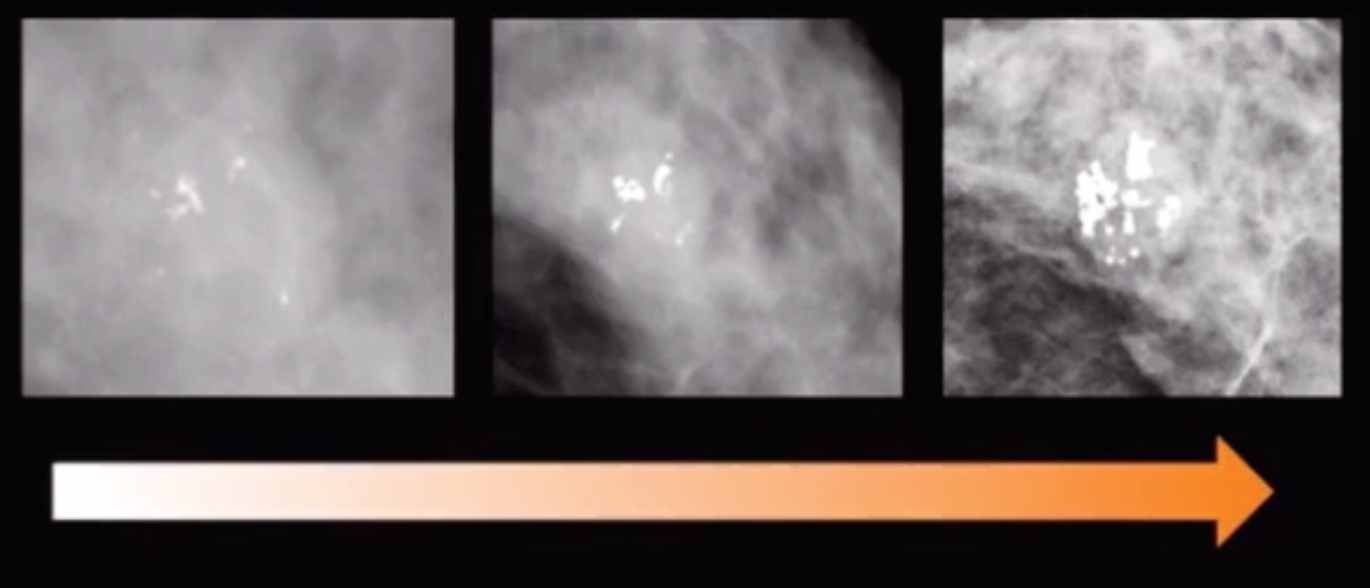
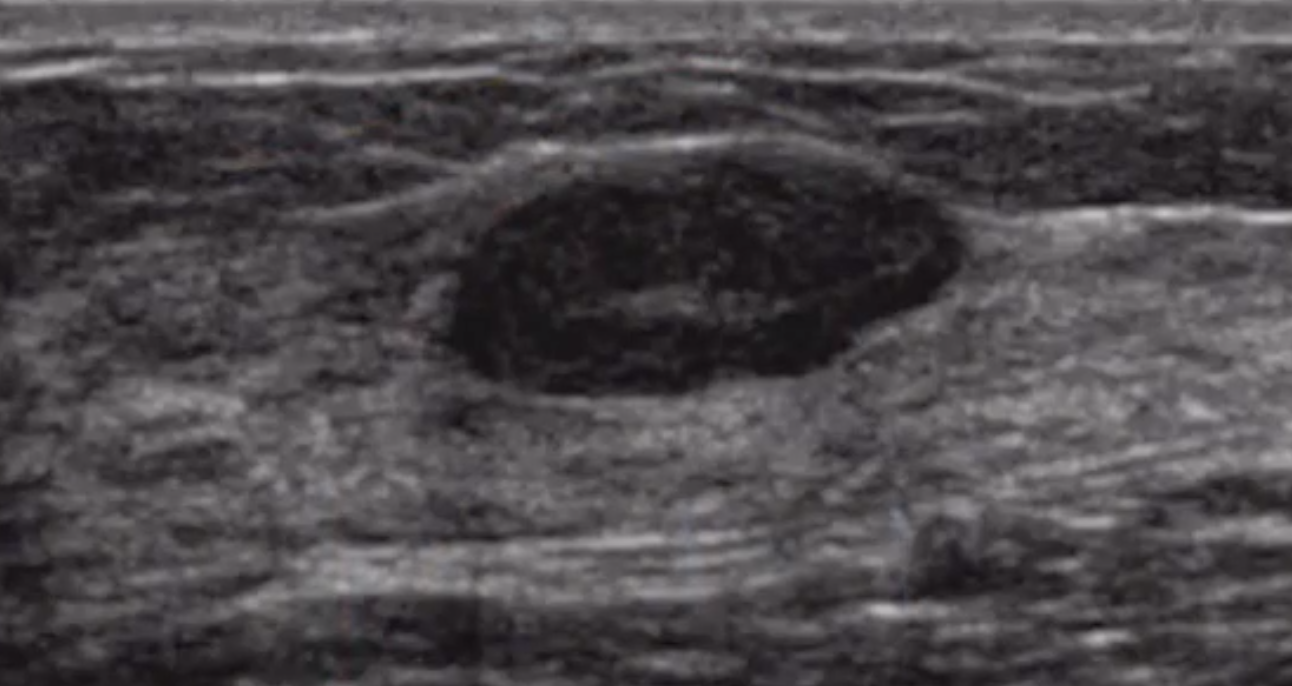
Fibroadenoma
Round well circumscribed mass with central scar
Largely hypoechoic with hyper-echoic central scar
Mass in pre-menopausal woman (estrogen dependent)
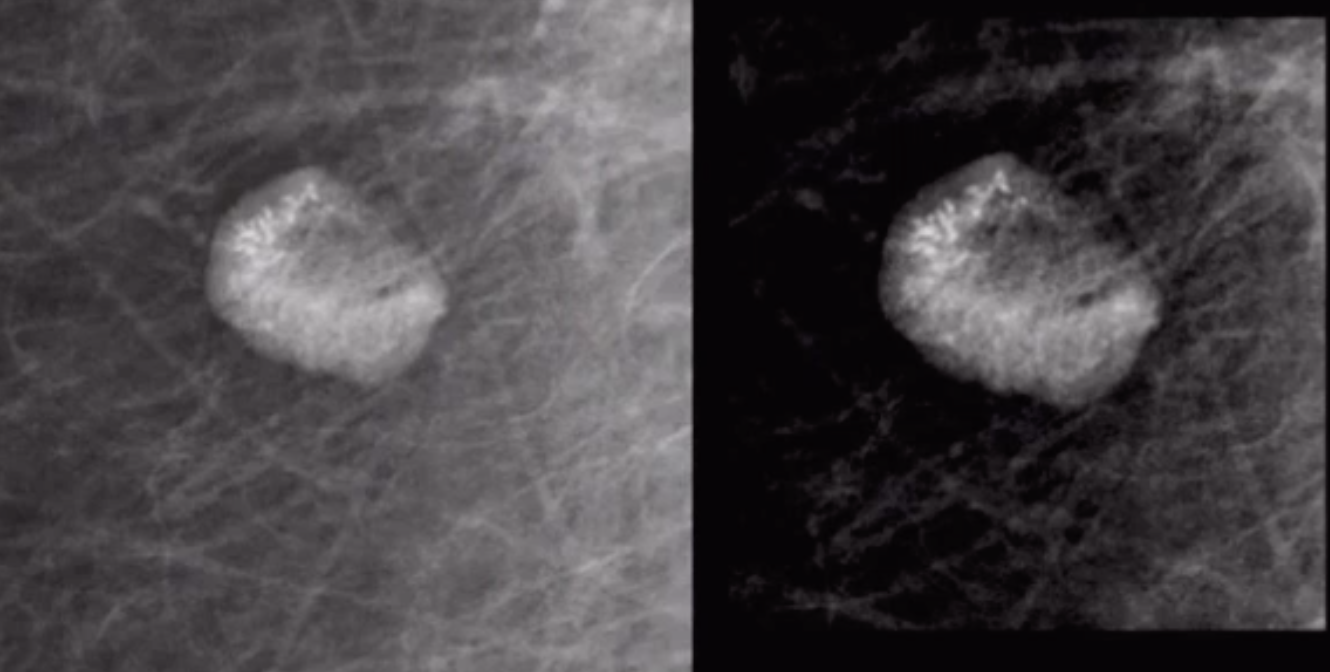
If seen in an older person it will have bulky popcorn calcs, with increased calcs in it over time - means degenerating
if > 5 cm = giant fibroadenoma
If grows > 20% in 6 months —> need biopsy to exclude phyllodes
MR findings
T2 bright
T1 post
Homogenous
Thin non-enhancing septa (Type 1 enhancement pattern)
Do not always enhance
Phyllodes tumor
Basically a fibroadenoma that grows too much and is in older women (50+)
Also reoccur more than fibroadenoma
Tend to be large on presentation, > 5 cm
Middle to older women
Homogenously hypoechoic, well circumscribed mass on US
If large, may have internal cystic components
Classified into
Benign
Borderline
Malignant (25% of cases are malignant)
All of these are treated with wide local excision even if benign
~20% of malignant phyllodes will metastasize, hematogenously to
Liver
Lung
Bone
Breast Hamartoma
Dense, focally disorganized but normal breast tissue with internal areas of fat
So called “breast within a breast” appearance
Not well seen on US
No biopsy if classic features
No increased risk of cancer
Fat Necrosis/Oil cyst
Eggshell looking thing with low density centrally
Prior trauma (surgery, true trauma)

Multiple Bilateral Masses
3+ masses bilaterally
Technically benign, idk not explained well
References:
Fat Containing Lesions (5) = benign = BR-2
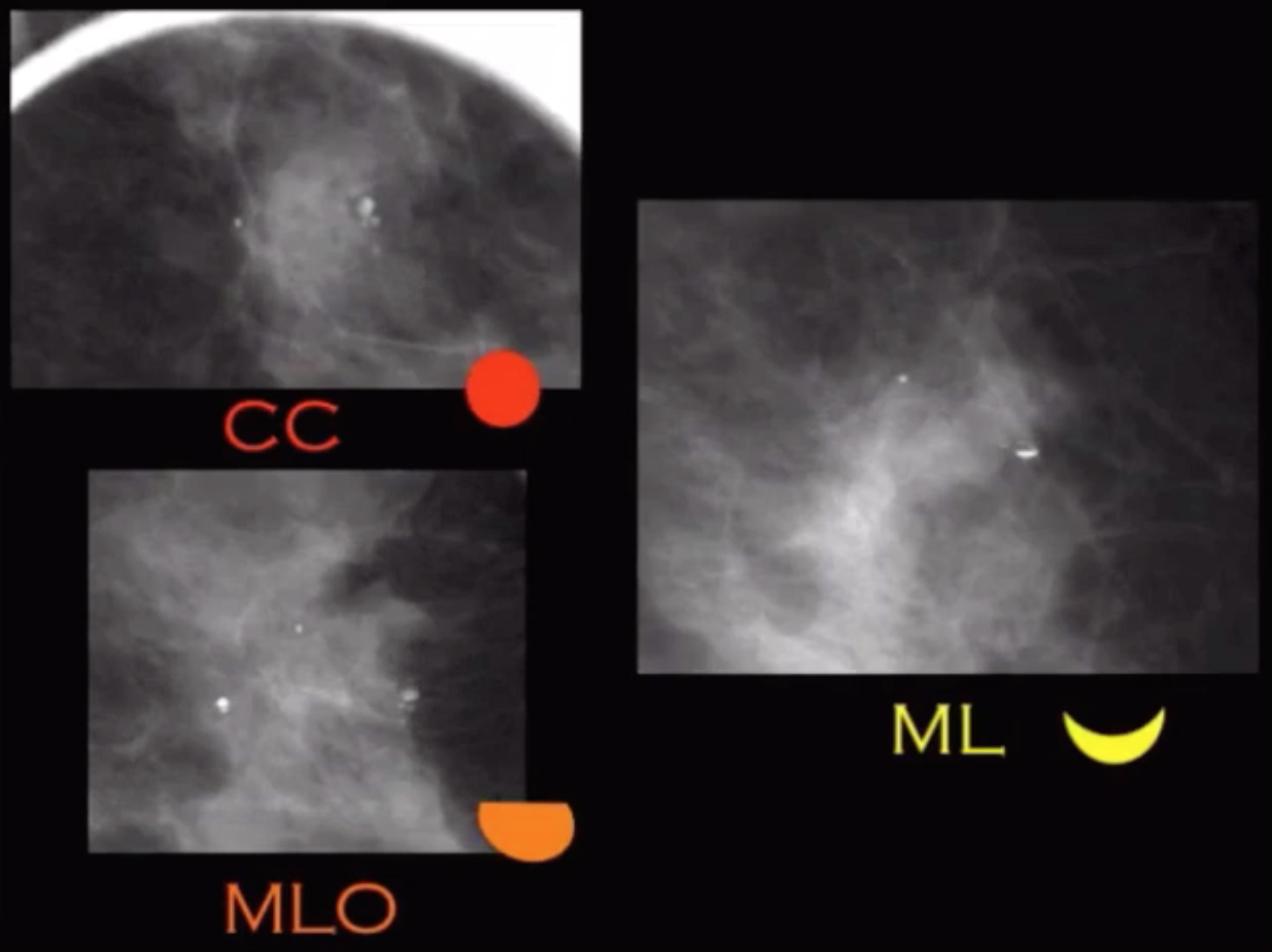
Milk of Calcium
Round calcs on CC that flatten on MLO
Get an ML view to prove, will really flatten out
Caused by dilated lobules in fibrocystic changes
BR-2 that shit
If you biopsy it and do not see calcs
Need to use polarized light to assess birefringence to see them
Mondor’s
Tubular looking thing
May have some doppler flow
Tender palpable cord
This is a thrombosed superficial vein
No need for AC
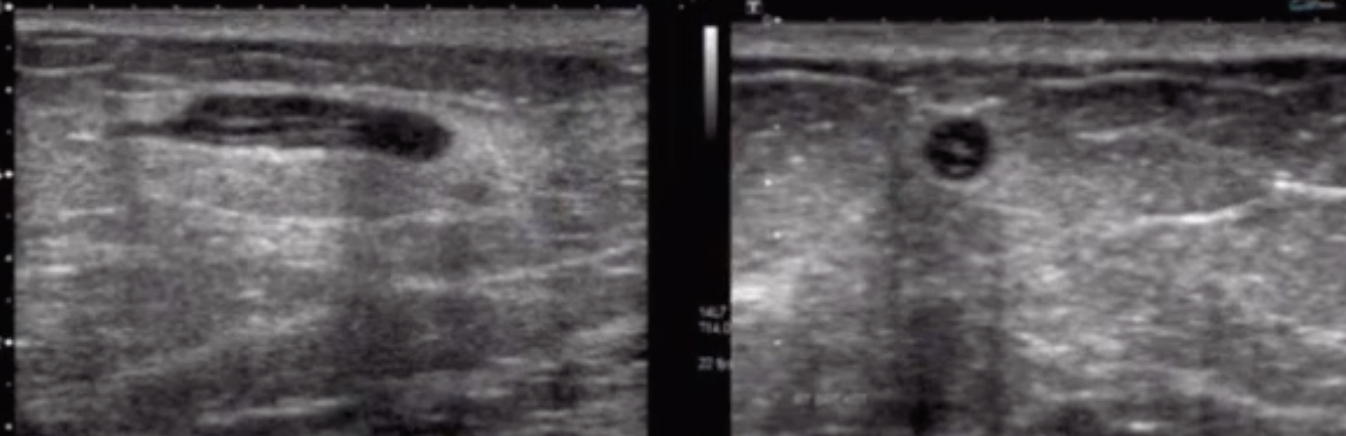
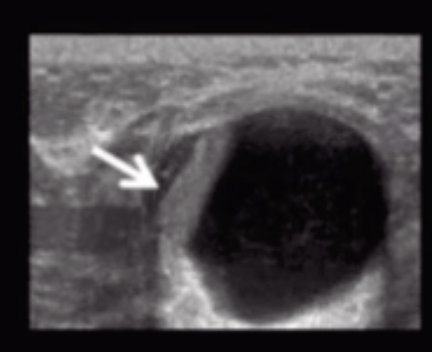
Galactocele
Subareolar
Fluid-fluid level on US
Only seen in lactating patient
Do not biopsy - can cause milk fistula
Lymph Nodes
Commonly in posterior third of breast
Pseudoangiomatosis Stromal Hyperplasia (PASH)
Benign myofibroblastic hyperplastic process
Mimics vascular lesions - hence pseudo-angiomatosis
Usually large (4-6 cm)
Solid, oval shaped mass with well defined borders
Typically no calcifications
Need to biopsy these because could be a huge fucking mass and you’re the idiot who said not do because could be PASH
Desmoid Tumor
Rare, benign but locally aggressive mass
Mass from proliferation of fibroblasts/myofibroblasts
Present as hard, palpable mass
Associated with prior injury
Associated with Gardner syndrome & FAP
Treated with wide local excision, sometimes with radiation
Recur in 1/3 of cases but do not metastasize
Benign Non-Mass Breast Changes
Other, Seemingly not so important benign breast changes?
Stromal fibrosis
Benign stromal proliferation that obliterates the ducts and acini
Causes fibrotic tissue with little fat in between
Can look like anything on mammo and needs biopsy
Seems more like a path thing that rads thing tbh
Usual ductal hyperplasia
Benign proliferation of ductal epithelial cells but cells look normal where as atypical ductal hyperplasia cells look atypical
No increased risk, no surgery intervention, again prob path thing not so much for rads
Diabetic Mastopathy
Autoimmune reaction to glycosylated proteins
Present as a hard mass
Commonly associated with Type-1-DM
Commonly recurs and may worsen with excision, so leave it alone after diagnosis
Gold Therapy
Basically punctate calcs in a LN
Old treatment for RA
Lipoma
Isoechoic (bright) to fat on US
No need for biopsy